Practice Essentials
Paget disease of bone (osteitis deformans) is a metabolic disorder characterized by abnormal osseous remodeling. Sir James Paget first described Paget disease in 1877 as a chronic inflammatory remodeling disease of bones. He termed the condition osteitis deformans. [1, 2, 3, 4] Paget disease of bone is caused by a localized increase in osteoclastic and osteoblastic activity and can progress to involve the entire bone. Deformed, enlarged bones are a common feature, especially in weight-bearing areas. [5] Genetic factors play an important role in pathogenesis, with evidence that susceptibility may be determined by variants in or near genes that regulate osteoclast function. [6, 7, 8, 9, 10, 11]
Paget disease of bone is the second most common bone disorder in elderly persons after osteoporosis. The disease occurs most commonly in the pelvis, spine, skull, and long bones. [12, 13] The disorder is most common in Europe, North America, and Australia but is rare in Asia and Africa. The prevalence of Paget disease has been found to be higher in regions with people of British descent, [10, 11, 14] but there is evidence that the disease has become less common and less severe in these regions over the past 25 years. [8, 10, 11] Linkage analysis identified SQSTM1, at chromosome 5q35, as directly related to the disease, [8] and genome-wide association studies have identified OPTN and RIN3 as causal genes. [9, 7]
Paget disease evolves through 3 stages: (1) an early lytic or hot phase; (2) an intermediate or mixed phase; and (3) a final or cold phase, marked by dense bone formation.
Imaging modalities
The radiographic findings of Paget disease are diagnostic in many patients, particularly in the lytic phase. [15, 16, 17] The lytic stage most commonly is observed in the skull and long bones. The typical appearance in the long bones is osteolysis, which begins in the epiphysis and advances along the diaphysis. Trabecular coarsening and distortion and cortical thickening are observed in the sclerotic phase, typically involving the axial skeleton. However, given the variable imaging appearance of Paget disease in different stages, as well as the many different bones involved, the differential diagnosis may vary substantially among patients. [1, 10]
The changes caused by Paget disease can also be detected by computed tomography (CT), magnetic resonance imaging (MRI), and positron emission tomography (PET) CT, which can help distinguish Paget disease from other potential causes and assess complications. Isotopic bone scans have been recommended to define the extent of metabolically active disease. [18, 19, 20]
(Paget disease is shown in the images below.)
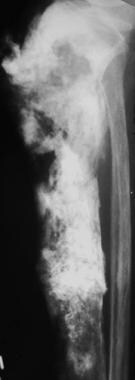 Lateral radiograph of the tibia in a patient with Paget sarcoma reveals a destructive bone-forming mass in the proximal tibia (osteosarcoma).
Lateral radiograph of the tibia in a patient with Paget sarcoma reveals a destructive bone-forming mass in the proximal tibia (osteosarcoma).
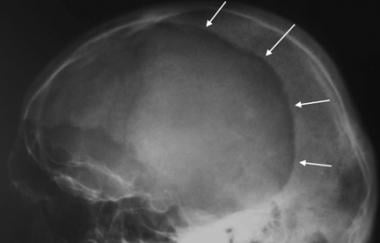 Lateral skull radiograph in a patient with Paget disease demonstrates a large, well-circumscribed lytic lesion (arrows) in the frontal and parietal bones (osteoporosis circumscripta).
Lateral skull radiograph in a patient with Paget disease demonstrates a large, well-circumscribed lytic lesion (arrows) in the frontal and parietal bones (osteoporosis circumscripta).
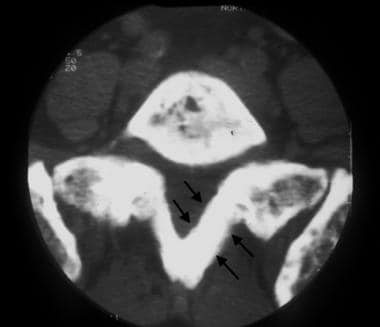 CT image of the first sacral vertebra demonstrates marked cortical thickening (arrows) and trabecular coarsening. Courtesy of Lee F. Rogers.
CT image of the first sacral vertebra demonstrates marked cortical thickening (arrows) and trabecular coarsening. Courtesy of Lee F. Rogers.
 Axial T1-weighted MRI of the knee in a patient with Paget disease reveals prominent dark lines in the medullary bone, indicating trabecular coarsening (arrows). Courtesy of Lee F. Rogers.
Axial T1-weighted MRI of the knee in a patient with Paget disease reveals prominent dark lines in the medullary bone, indicating trabecular coarsening (arrows). Courtesy of Lee F. Rogers.
 Whole-body bone scan in a patient with polyostotic Paget disease reveals intense uptake of radiopharmaceutical in the femur, pelvis, spine, and proximal right humerus. The cortical discontinuity of the proximal right humerus represents an insufficiency fracture (arrow). Courtesy of Lee F. Rogers.
Whole-body bone scan in a patient with polyostotic Paget disease reveals intense uptake of radiopharmaceutical in the femur, pelvis, spine, and proximal right humerus. The cortical discontinuity of the proximal right humerus represents an insufficiency fracture (arrow). Courtesy of Lee F. Rogers.
Paget disease rarely is diagnosed in the initial lytic phase. At this early point of the disease, osteoclastic activity is predominant. Paget disease usually begins at the end of a bone, except when it occurs in the tibia. A characteristic sharply demarcated zone of osteolysis may begin in the subcortical bone and advance along the diaphysis. Osteoblastic activity lags behind; thus, radiolucent fibrous tissue replaces normal bone.
The intermediate or mixed phase reveals evidence of osteolytic and disorganized osteoblastic activity. New bone forms abnormally and demonstrates characteristically coarsened trabeculae and cortical thickening in the cancellous and compact bone, respectively. Characteristic intracytoplasmic inclusions may be observed microscopically, supporting evidence for the viral etiology theory.
The final or cold phase demonstrates less evidence of continual osseous remodeling. Previously laid down woven bone is converted to dense lamellar bone. Histologic features of disorganized bone are prominent. The intersecting lines of remodeled bone have a characteristic mosaic pattern histologically.
Insufficiency fractures in patients with Paget disease may present with pain that can last up to several weeks. If pain is focal and severe, it may be a sign of an impending, complete fracture, and radiographic evaluation is warranted. Insufficiency fractures most frequently affect the femur and tibia. Involvement in critical weight-bearing locations may lead to fracture or severe secondary arthritis. [21, 22, 23]
(See the images below.)
 Anteroposterior radiograph of the hip in a patient with Paget disease demonstrates dense sclerosis involving the femoral head and neck (arrows). This is a high-risk area for insufficiency fracture.
Anteroposterior radiograph of the hip in a patient with Paget disease demonstrates dense sclerosis involving the femoral head and neck (arrows). This is a high-risk area for insufficiency fracture.
 Anteroposterior radiograph of the femur in a patient with late-stage Paget disease reveals a transverse insufficiency fracture through the proximal femoral shaft (banana fracture).
Anteroposterior radiograph of the femur in a patient with late-stage Paget disease reveals a transverse insufficiency fracture through the proximal femoral shaft (banana fracture).
Other complications incude deafness, hydrocephalus, and osteosarcoma. [18] Involvement of the spine may cause nerve entrapment and even spinal canal stenosis. Paget diesease is also associated with aortic stenosis, atherosclerosis, and intracardiac calcification. [19]
Treatment
Treatment with nitrogen-containing bisphosphonates (eg, zoledronic acid, pamidronate, alendronate, risedronate) is recommended in cases of active disease or in individuals at risk of possible complications such as arthritis, gait changes, hearing loss, nerve compression syndromes, or osteosarcoma. [13] Patients who do not tolerate bisphosphonates can be treated with calcitonin. [24]
Bisphosphonates are considered to be the treatment of choice because they are highly effective at suppressing increased bone turnover. Studies have shown that treatment with alendronate and risedronate, for example, can promote formation of lamellar bone in affected sites. Bisphosphonates have also been shown to improve bone pain. [25]
A single 5-mg intravenous infusion of zoledronic acid has been found to be able to normalize alkaline phosphatase levels for up to 6.5 years. [26] Increased serum alkaline phosphatase level correlates with disease activity. [24]
In a Cochrane database review by Corral-Gudino et al, 10 trials (801 participants) compared bisphosphonates (etidronate, tiludronate, ibandronate, pamidronate, olpadronate, alendronate, risedronate, zoledronate) with placebo, and the bisphosphonates were found to have tripled the percentage (31% versus 9%) of patients whose bone pain resolved. [27]
Guidelines
Guidelines for Paget disease of bone were developed by the Paget’s Association and include the following [28, 29, 30] :
-
Radionuclide bone scans, in addition to targeted radiographs, are recommended as a means of fully and accurately defining the extent of metabolically active disease.
-
Serum total alkaline phosphatase (ALP) is recommended as a first-line biochemical screening test in combination with liver function tests.
-
Bisphosphonates are recommended for the treatment of bone pain. Zoledronic acid is recommended as the bisphosphonate most likely to provide a favorable pain response.
Radiography
In the skull, the lytic phase (osteoporosis circumscripta) typically involves the frontal or occipital bones and progresses to a mixed pattern with multifocal sclerotic patches in the intermediate stage of the disease, referred to as a cotton wool appearance. [31]
(See the images below.)
Anteroposterior radiograph of the femur in a patient with late-stage Paget disease reveals a transverse insufficiency fracture through the proximal femoral shaft (banana fracture).
 Lateral radiograph of the calvarium in a patient with Paget disease reveals multiple patches of sclerotic bone in the calvarium (cotton wool appearance).
Lateral radiograph of the calvarium in a patient with Paget disease reveals multiple patches of sclerotic bone in the calvarium (cotton wool appearance).
The vertebral bodies typically become enlarged with a prominent cortical margin (picture frame vertebrae) or become densely sclerotic, mimicking lymphoma or metastatic disease (ivory vertebra). (See the images below.)
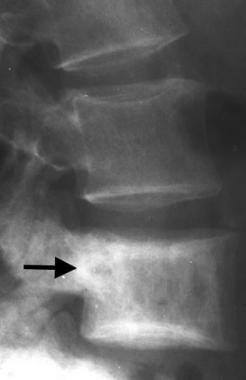 Lateral radiograph of the lumbar spine in a patient with Paget disease demonstrates enlargement of an involved vertebral body (arrow), with sclerosis more prominent at the vertebral endplates (picture frame vertebra).
Lateral radiograph of the lumbar spine in a patient with Paget disease demonstrates enlargement of an involved vertebral body (arrow), with sclerosis more prominent at the vertebral endplates (picture frame vertebra).
 Lateral radiograph of the upper thoracic spine reveals a densely sclerotic vertebral body (ivory vertebra) caused by Paget disease (arrow). The appearance mimics findings that can be observed with malignant neoplasm such as lymphoma or metastatic disease.
Lateral radiograph of the upper thoracic spine reveals a densely sclerotic vertebral body (ivory vertebra) caused by Paget disease (arrow). The appearance mimics findings that can be observed with malignant neoplasm such as lymphoma or metastatic disease.
In the pelvis, typical findings include thickening of the iliopectineal line in early stages, progressing to patchy sclerosis and lucency in later stages. (See the image below.)
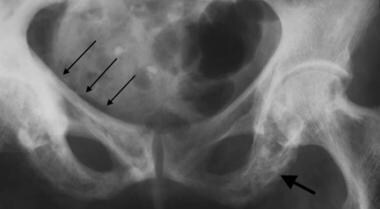 Anteroposterior radiograph of the pelvis demonstrates thickening of the right iliopectineal line (small arrows), as well as later-stage involvement with Paget disease, including trabecular coarsening and patchy sclerosis (large arrow).
Anteroposterior radiograph of the pelvis demonstrates thickening of the right iliopectineal line (small arrows), as well as later-stage involvement with Paget disease, including trabecular coarsening and patchy sclerosis (large arrow).
Weakening of the pagetic acetabular bone may lead to protrusio acetabuli and insufficiency fracture. (See the image below.)
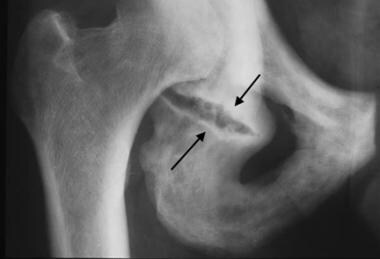 Anteroposterior radiograph of the right hip, coned down on the obturator ring, reveals patchy sclerosis and disorganized coarsened trabecula characteristic of late-stage Paget disease. An insufficiency fracture of the ischium inferior to the acetabulum (arrows) is present.
Anteroposterior radiograph of the right hip, coned down on the obturator ring, reveals patchy sclerosis and disorganized coarsened trabecula characteristic of late-stage Paget disease. An insufficiency fracture of the ischium inferior to the acetabulum (arrows) is present.
In the long bones, early involvement consists of lysis of the subarticular bone, which advances along the diaphysis with the characteristic shape of a blade of grass. Long bones are affected first in the epiphyseal region, with the exception of the tibia, where Paget disease frequently begins in the tubercle.
Later stages of disease show development of enlarged, sclerotic, deformed bones with thickened coarse trabeculae. The weakened femur and tibia eventually may become bowed under the stress of weight bearing. Insufficiency fractures may occur, characteristically involving the convex cortical surface. Conversely, Looser zones of osteomalacia typically occur on the concave cortical surface. (See the images below.)
 Coned down anteroposterior radiograph of the knee demonstrates an abnormal lucency in the distal femur with a flame-shaped or "blade of grass"-shaped proximal margin caused by the advancing lytic phase of Paget disease (black arrows). Courtesy of Lee F. Rogers.
Coned down anteroposterior radiograph of the knee demonstrates an abnormal lucency in the distal femur with a flame-shaped or "blade of grass"-shaped proximal margin caused by the advancing lytic phase of Paget disease (black arrows). Courtesy of Lee F. Rogers.
 Lateral coned down radiograph of the tibia reveals replacement of the tibial tubercle with pagetic bone that has mixed osteolysis and sclerosis (arrows).
Lateral coned down radiograph of the tibia reveals replacement of the tibial tubercle with pagetic bone that has mixed osteolysis and sclerosis (arrows).
 Anteroposterior radiograph of the distal forearm demonstrates mixed-phase Paget disease in the distal radius with lytic disease proximally (white arrows) and coarsened trabeculae more distally (black arrow).
Anteroposterior radiograph of the distal forearm demonstrates mixed-phase Paget disease in the distal radius with lytic disease proximally (white arrows) and coarsened trabeculae more distally (black arrow).
 Anteroposterior radiograph of the proximal femur involved with intermediate (mixed phase) Paget disease reveals characteristic insufficiency fractures on the convex surface of the bone (arrow).
Anteroposterior radiograph of the proximal femur involved with intermediate (mixed phase) Paget disease reveals characteristic insufficiency fractures on the convex surface of the bone (arrow).
Development of secondary sarcoma in pagetic bone is the most lethal complication of Paget disease, occurring in 1% or fewer of patients with Paget disease (see the image below). These sarcomas are aggressive and may be multicentric. Short-term interval follow-up and/or cross-sectional imaging may prevent diagnostic errors and initiate prompt attention to a newly developing lesion. [32, 33, 34]
Lateral radiograph of the tibia in a patient with Paget sarcoma reveals a destructive bone-forming mass in the proximal tibia (osteosarcoma).
Computed Tomography
Cross-sectional MRI and CT demonstrate the altered bone structure seen in Paget disease, such as coarsened trabeculae, thickened cortices, and bone hypertrophy. Findings that are present on plain radiography are often better displayed on CT. MRI does not depict the changes in mineralization as well as traditional radiography or CT. MRI, however, can show alterations in marrow characteristics that can mirror the pathologic changes occurring during the course of the disease. Thus, earlier in the disease, marrow signal can be normal or hypervascular, while later changes can show fatty replacement of the marrow. [35]
The anatomy is well demonstrated by cross-sectional imaging in complex structures, such as the spine, where spinal or nerve root compression may be an issue. Cross-sectional imaging also helps delineate the pathology in complicated Paget disease, which includes nerve or spinal cord compression, as well as basilar invagination at the skull base and osseous encroachment involving cranial nerve foramina.
Secondary sarcomatous development also is better evaluated with cross-sectional imaging. Additionally, should biopsy be indicated for the diagnosis of sarcoma, CT typically is the guidance modality of choice. (See the images below.)
CT image of the first sacral vertebra demonstrates marked cortical thickening (arrows) and trabecular coarsening. Courtesy of Lee F. Rogers.
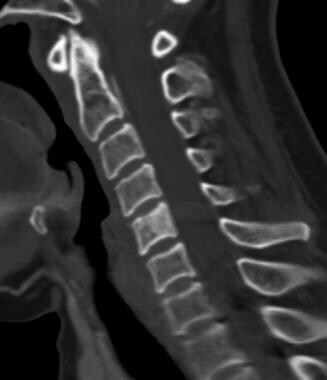 Sagittal CT image of the cervical spine demonstrates increased sclerosis within the C5 vertebral body. This is the CT version of the "ivory vertebra". Also note the subtle thickening of the cortex as compared with the adjacent vertebral bodies.
Axial T1-weighted MRI of the knee in a patient with Paget disease reveals prominent dark lines in the medullary bone, indicating trabecular coarsening (arrows). Courtesy of Lee F. Rogers.
Sagittal CT image of the cervical spine demonstrates increased sclerosis within the C5 vertebral body. This is the CT version of the "ivory vertebra". Also note the subtle thickening of the cortex as compared with the adjacent vertebral bodies.
Axial T1-weighted MRI of the knee in a patient with Paget disease reveals prominent dark lines in the medullary bone, indicating trabecular coarsening (arrows). Courtesy of Lee F. Rogers.
 Sagittal T1-weighted MRI of the lumbar spine demonstrates enlargement of the fourth lumbar vertebral body with no central canal encroachment (arrows). Courtesy of Lee F. Rogers.
Sagittal T1-weighted MRI of the lumbar spine demonstrates enlargement of the fourth lumbar vertebral body with no central canal encroachment (arrows). Courtesy of Lee F. Rogers.
 Sagittal T1-weighted MRI of the lumbosacral spine demonstrates Paget disease in the sacrum. There is increased signal intensity throughout the sacral marrow, indicative of fatty replacement. Compare with the marrow signal characteristics of the lumbar vertebrae, as well as the adjacent intra-pelvic fat.
Sagittal T1-weighted MRI of the lumbosacral spine demonstrates Paget disease in the sacrum. There is increased signal intensity throughout the sacral marrow, indicative of fatty replacement. Compare with the marrow signal characteristics of the lumbar vertebrae, as well as the adjacent intra-pelvic fat.
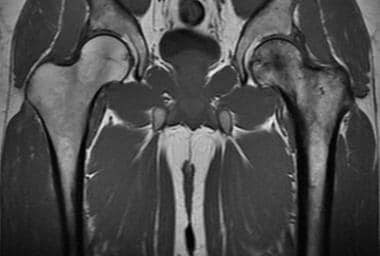 Coronal T1-weighted MRI of the hips shows Paget disease of the proximal left femur. Note the coarsened trabeculae and thickened cortex, changes which are low signal on MRI.
Coronal T1-weighted MRI of the hips shows Paget disease of the proximal left femur. Note the coarsened trabeculae and thickened cortex, changes which are low signal on MRI.
Magnetic Resonance Imaging
In a study of the use of MRI in patients with Paget disease of the spine, MRI showed a mixed pattern of increased/decreased T1 signal (fine trabecular or coarse) of the vertebral bodies. Band-like decreased T1 and T2 signal of the endplates was also present, correlating with the mixed osteolytic and blastic phase of the disease. Subtle or conspicuous picture-frame appearance was also noted. In most cases, there was expansion of the vertebral body and/or posterior elements/spinous process. [36]
(See the images below.)
Axial T1-weighted MRI of the knee in a patient with Paget disease reveals prominent dark lines in the medullary bone, indicating trabecular coarsening (arrows). Courtesy of Lee F. Rogers.
Sagittal T1-weighted MRI of the lumbosacral spine demonstrates Paget disease in the sacrum. There is increased signal intensity throughout the sacral marrow, indicative of fatty replacement. Compare with the marrow signal characteristics of the lumbar vertebrae, as well as the adjacent intra-pelvic fat.
Nuclear Imaging
Skeletal scintigraphy is useful. Radionuclide bone scans are more sensitive than radiographs for the diagnosis of Paget disease. Additionally, bone scans help survey the different sites of involvement with polyostotic disease.
Characteristically, a marked uptake of radiopharmaceutical in the involved bones is observed. However, late-stage involvement may not reveal intense radiopharmaceutical uptake, and osteoporosis circumscripta may demonstrate only a peripheral rim of increased uptake. Scintigraphy tends to follow the physiologic activity of disease and may monitor treatment.
Polyostotic Paget disease often can be distinguished from multiple metastatic lesions, although occasional difficulties occur. Perform radiographic correlation when this situation arises. Furthermore, the diagnosis of fracture or sarcoma may be challenging, often requiring multimodality correlation. (See the images below.)
Whole-body bone scan in a patient with polyostotic Paget disease reveals intense uptake of radiopharmaceutical in the femur, pelvis, spine, and proximal right humerus. The cortical discontinuity of the proximal right humerus represents an insufficiency fracture (arrow). Courtesy of Lee F. Rogers.
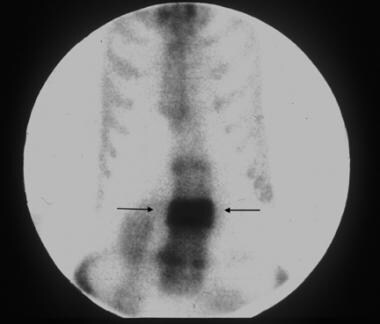 Anterior image of the thoracic and lumbar spine in a 75-year-old man demonstrates intense radiopharmaceutical uptake in the third lumbar vertebra, which is involved with Paget disease (arrows). Courtesy of Lee F. Rogers.
Anterior image of the thoracic and lumbar spine in a 75-year-old man demonstrates intense radiopharmaceutical uptake in the third lumbar vertebra, which is involved with Paget disease (arrows). Courtesy of Lee F. Rogers.
-
Lateral radiograph of the tibia in a patient with Paget sarcoma reveals a destructive bone-forming mass in the proximal tibia (osteosarcoma).
-
Anteroposterior radiograph of the hip in a patient with Paget disease demonstrates dense sclerosis involving the femoral head and neck (arrows). This is a high-risk area for insufficiency fracture.
-
Anteroposterior radiograph of the femur in a patient with late-stage Paget disease reveals a transverse insufficiency fracture through the proximal femoral shaft (banana fracture).
-
Lateral skull radiograph in a patient with Paget disease demonstrates a large, well-circumscribed lytic lesion (arrows) in the frontal and parietal bones (osteoporosis circumscripta).
-
Lateral radiograph of the calvarium in a patient with Paget disease reveals multiple patches of sclerotic bone in the calvarium (cotton wool appearance).
-
Lateral radiograph of the lumbar spine in a patient with Paget disease demonstrates enlargement of an involved vertebral body (arrow), with sclerosis more prominent at the vertebral endplates (picture frame vertebra).
-
Lateral radiograph of the upper thoracic spine reveals a densely sclerotic vertebral body (ivory vertebra) caused by Paget disease (arrow). The appearance mimics findings that can be observed with malignant neoplasm such as lymphoma or metastatic disease.
-
Anteroposterior radiograph of the pelvis demonstrates thickening of the right iliopectineal line (small arrows), as well as later-stage involvement with Paget disease, including trabecular coarsening and patchy sclerosis (large arrow).
-
Anteroposterior radiograph of the right hip, coned down on the obturator ring, reveals patchy sclerosis and disorganized coarsened trabecula characteristic of late-stage Paget disease. An insufficiency fracture of the ischium inferior to the acetabulum (arrows) is present.
-
Coned down anteroposterior radiograph of the knee demonstrates an abnormal lucency in the distal femur with a flame-shaped or "blade of grass"-shaped proximal margin caused by the advancing lytic phase of Paget disease (black arrows). Courtesy of Lee F. Rogers.
-
Lateral coned down radiograph of the tibia reveals replacement of the tibial tubercle with pagetic bone that has mixed osteolysis and sclerosis (arrows).
-
Anteroposterior radiograph of the distal forearm demonstrates mixed-phase Paget disease in the distal radius with lytic disease proximally (white arrows) and coarsened trabeculae more distally (black arrow).
-
Anteroposterior radiograph of the proximal femur involved with intermediate (mixed phase) Paget disease reveals characteristic insufficiency fractures on the convex surface of the bone (arrow).
-
CT image of the first sacral vertebra demonstrates marked cortical thickening (arrows) and trabecular coarsening. Courtesy of Lee F. Rogers.
-
Axial T1-weighted MRI of the knee in a patient with Paget disease reveals prominent dark lines in the medullary bone, indicating trabecular coarsening (arrows). Courtesy of Lee F. Rogers.
-
Sagittal T1-weighted MRI of the lumbar spine demonstrates enlargement of the fourth lumbar vertebral body with no central canal encroachment (arrows). Courtesy of Lee F. Rogers.
-
Whole-body bone scan in a patient with polyostotic Paget disease reveals intense uptake of radiopharmaceutical in the femur, pelvis, spine, and proximal right humerus. The cortical discontinuity of the proximal right humerus represents an insufficiency fracture (arrow). Courtesy of Lee F. Rogers.
-
Anterior image of the thoracic and lumbar spine in a 75-year-old man demonstrates intense radiopharmaceutical uptake in the third lumbar vertebra, which is involved with Paget disease (arrows). Courtesy of Lee F. Rogers.
-
Photomicrograph of bone involved with late-stage Paget disease demonstrates intersecting remodeling lines forming a mosaic pattern.
-
Sagittal CT image of the cervical spine demonstrates increased sclerosis within the C5 vertebral body. This is the CT version of the "ivory vertebra". Also note the subtle thickening of the cortex as compared with the adjacent vertebral bodies.
-
Sagittal T1-weighted MRI of the lumbosacral spine demonstrates Paget disease in the sacrum. There is increased signal intensity throughout the sacral marrow, indicative of fatty replacement. Compare with the marrow signal characteristics of the lumbar vertebrae, as well as the adjacent intra-pelvic fat.
-
Coronal T1-weighted MRI of the hips shows Paget disease of the proximal left femur. Note the coarsened trabeculae and thickened cortex, changes which are low signal on MRI.






