Practice Essentials
Osteosarcoma is the most common primary malignant tumor of bone, excluding plasma cell myeloma. Approximately 75% of all osteosarcomas are of the classic or conventional type, and the remaining 25% constitute the osteosarcoma variants. The variants are a heterogeneous group of osteosarcomas with a range of different imaging and behavioral features. [1, 2, 3, 4, 5] They include telangiectatic, [6, 7, 8] chondromyxoid fibroma–like, [9, 10] gnathic, [11, 12] parosteal, intracortical, and periosteal, among others.
Preferred modalities for evaluating primary disease are radiography, MRI, and sometimes CT scanning. MRI is the optimum technique for local staging of osteosarcomas. Histologic confirmation of the nature of the tumor is required [13] ; the analysis should be performed after MRI and in consultation with the tumor surgeon.
To detect pulmonary metastases, staging is performed by using chest CT scanning . Isotopic bone scanning is generally used to detect skeletal metastases or synchronous tumors, but whole-body MRI may replace this study. [14, 15]
Ultrasonography can demonstrate the soft-tissue extent of the tumor, but it cannot be used to evaluate the intramedullary component of the lesion. Ultrasonography is not routinely used in staging such lesions. Sonography can be useful in guiding percutaneous biopsy of the soft-tissue component of the tumor, again in consultation with an orthopedic oncologist.
The overall prognosis for patients with osteosarcoma depends on the stage of the tumor at presentation. Without metastases, long-term survival is in the order of 60-85%.
Telangiectatic osteosarcoma (as shown in the images below) has been considered more aggressive than classic osteosarcoma, but studies of long-term survival after optimum treatment now indicate that the aggressiveness of telangiectatic osteosarcoma is similar to that of the classic type.
 Frontal radiograph of the distal femur in a patient with telangiectatic osteosarcoma. The radiograph shows mixed medullary sclerosis and lucency, cortical destruction medially, aggressive periosteal changes, and a large soft-tissue mass with peripheral ossification.
Frontal radiograph of the distal femur in a patient with telangiectatic osteosarcoma. The radiograph shows mixed medullary sclerosis and lucency, cortical destruction medially, aggressive periosteal changes, and a large soft-tissue mass with peripheral ossification.
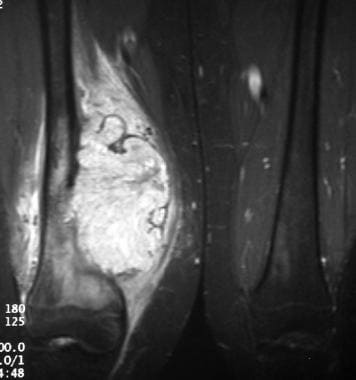 Coronal short-tau inversion recovery (STIR) magnetic resonance imaging (MRI) scan of the same patient (patient with telangiectatic osteosarcoma). Note the abnormal signal intensity of the bone marrow in the metaphysis of the femur, the cortical destruction, and the prominent soft-tissue mass with the surrounding edema or reactive zone.
Coronal short-tau inversion recovery (STIR) magnetic resonance imaging (MRI) scan of the same patient (patient with telangiectatic osteosarcoma). Note the abnormal signal intensity of the bone marrow in the metaphysis of the femur, the cortical destruction, and the prominent soft-tissue mass with the surrounding edema or reactive zone.
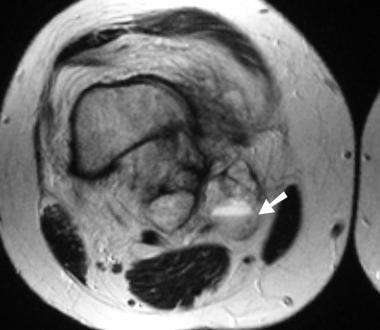 Axial T2-weighted magnetic resonance imaging (MRI) scan of the same patient (patient with telangiectatic osteosarcoma). A fluid-fluid level is present within the abnormal extraosseous tumor mass (arrow). The abnormal intramedullary tissue is less obvious in this sequence than in others.
Axial T2-weighted magnetic resonance imaging (MRI) scan of the same patient (patient with telangiectatic osteosarcoma). A fluid-fluid level is present within the abnormal extraosseous tumor mass (arrow). The abnormal intramedullary tissue is less obvious in this sequence than in others.
Intraosseous low-grade osteosarcoma generally has a good prognosis. Chondromyxoid fibroma–like osteosarcoma (CMF-OS) is among the rarest subtypes of low-grade central osteosarcoma (LGCO); It has a variable presentation on radiographs and is often misdiagnosed. Although classified as a low-grade tumor, it exhibits aggressive high-grade biological behavior, with a 10% metastatic rate. [16, 9, 10] Low-grade osteosarcoma, which is also known as intraosseous well-differentiated osteosarcoma, is an intramedullary bone-producing tumor accounting for about 1-2% of all osteosarcomas. [17]
Gnathic osteosarcoma (as shown in the images below) is less frequently associated with metastatic spread than is conventional osteosarcoma, but local disease recurrence is often problematic.
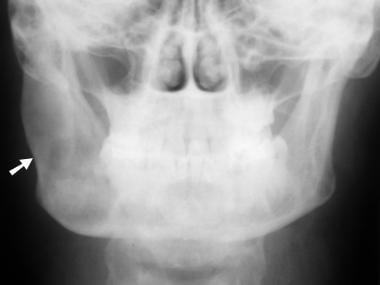 Frontal radiograph of the mandible in an adult with gnathic osteosarcoma. The radiograph shows a large, expansile lesion in the right ramus (arrow), with a mixed lytic and sclerotic appearance.
Frontal radiograph of the mandible in an adult with gnathic osteosarcoma. The radiograph shows a large, expansile lesion in the right ramus (arrow), with a mixed lytic and sclerotic appearance.
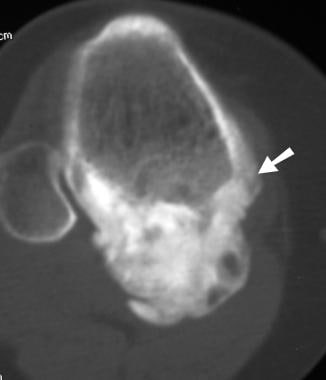
 Axial computed tomography (CT) scan obtained with bone window settings, in the same patient (adult with gnathic osteosarcoma). Osseous expansion and the mixed lytic and sclerotic process are again appreciated. A large soft-tissue component (arrow) also is now visible.
Axial computed tomography (CT) scan obtained with bone window settings, in the same patient (adult with gnathic osteosarcoma). Osseous expansion and the mixed lytic and sclerotic process are again appreciated. A large soft-tissue component (arrow) also is now visible.
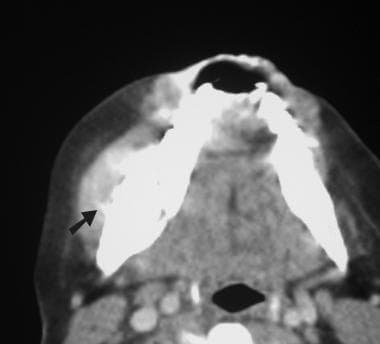 Axial computed tomography (CT) scan obtained with soft-tissue window settings, in the same patient (adult with gnathic osteosarcoma). Extension of ossified matrix into the soft-tissue component of the tumor is shown (arrow).
Axial computed tomography (CT) scan obtained with soft-tissue window settings, in the same patient (adult with gnathic osteosarcoma). Extension of ossified matrix into the soft-tissue component of the tumor is shown (arrow).
The prognosis for intracortical osteosarcoma is unclear because of its rarity. Both small-cell and secondary osteosarcoma are generally associated with a poor prognosis. [18, 1] High-grade surface osteosarcoma has a prognosis similar to that for a conventional osteosarcoma, and the prognosis for periosteal osteosarcoma (shown in the images below) is better than that for conventional osteosarcoma.
 Anteroposterior (AP) radiograph of the proximal tibia in a child with periosteal osteosarcoma. The metal pointer localizes the lesion for biopsy.
Anteroposterior (AP) radiograph of the proximal tibia in a child with periosteal osteosarcoma. The metal pointer localizes the lesion for biopsy.
 Coronal short-tau inversion recovery (STIR) magnetic resonance imaging (MRI) scan of the same patient (child with periosteal osteosarcoma). The ossified component of the tumor shows low signal intensity (white arrow), but superficially, hyperintense material (black arrow) is present. This may be chondroblastic soft-tissue extension of tumor, adjacent reactive edema, or a combination of both.
Coronal short-tau inversion recovery (STIR) magnetic resonance imaging (MRI) scan of the same patient (child with periosteal osteosarcoma). The ossified component of the tumor shows low signal intensity (white arrow), but superficially, hyperintense material (black arrow) is present. This may be chondroblastic soft-tissue extension of tumor, adjacent reactive edema, or a combination of both.
The prognosis for a parosteal osteosarcoma (as shown in the images below) is generally excellent. [2] Only a few cases of local recurrence with systemic metastasis occurring beyond 10 years have been reported. [19]
 Lateral radiograph of the proximal tibia in a patient with parosteal osteosarcoma. Note the opaque, lobulated, amorphous or cloudlike mass of abnormal, ossified tumor, which is inseparable from the posterior aspect of the tibia.
Lateral radiograph of the proximal tibia in a patient with parosteal osteosarcoma. Note the opaque, lobulated, amorphous or cloudlike mass of abnormal, ossified tumor, which is inseparable from the posterior aspect of the tibia.
 Axial computed tomography (CT) scan of the same patient (patient with parosteal osteosarcoma). The ossified tumor mass is readily shown, and the thickened cortex is visible at the junction of tumor and normal bone (arrow). The medullary cavity of the tibia appears normal.
Axial computed tomography (CT) scan of the same patient (patient with parosteal osteosarcoma). The ossified tumor mass is readily shown, and the thickened cortex is visible at the junction of tumor and normal bone (arrow). The medullary cavity of the tibia appears normal.
 Axial T1-weighted magnetic resonance imaging (MRI) scan of the same patient (patient with parosteal osteosarcoma). The medullary cavity of the tibia shows predominantly normal signal intensity, except posteriorly, where the slightly reduced signal intensity raises the possibility of early tumoral invasion (arrow). This area was normal on histologic examination.
Axial T1-weighted magnetic resonance imaging (MRI) scan of the same patient (patient with parosteal osteosarcoma). The medullary cavity of the tibia shows predominantly normal signal intensity, except posteriorly, where the slightly reduced signal intensity raises the possibility of early tumoral invasion (arrow). This area was normal on histologic examination.
The prognosis for multicentric osteosarcoma is dire.
Conventional osteosarcoma is most frequent in areas of high skeletal growth, especially the metaphyseal regions of the distal femur, proximal tibia, and proximal humerus. Most osteosarcoma variants follow a similar distribution, with the exception of gnathic (mandible and maxilla) lesions, intracortical lesions (rare but more typically diaphyseal), periosteal lesions (more typically diaphyseal), and secondary osteosarcomas. [3, 4, 20] The last osteosarcomas frequently occur in the pelvis and proximal femur, often in association with Paget disease (as demonstrated in the images below). Paget sarcomatous transformation is a rare and potentially fatal complication of Paget disease and is typically described as a high-grade, extremely aggressive malignancy. [17]
 Anteroposterior (AP) radiograph of the proximal femur in a patient with Paget disease demonstrates the typical features of cortical thickening, osseous expansion, and trabecular coarsening. In addition, irregular bone lucency and cortical destruction are shown in the medial aspect of the shaft; this is consistent with secondary sarcoma formation.
Anteroposterior (AP) radiograph of the proximal femur in a patient with Paget disease demonstrates the typical features of cortical thickening, osseous expansion, and trabecular coarsening. In addition, irregular bone lucency and cortical destruction are shown in the medial aspect of the shaft; this is consistent with secondary sarcoma formation.
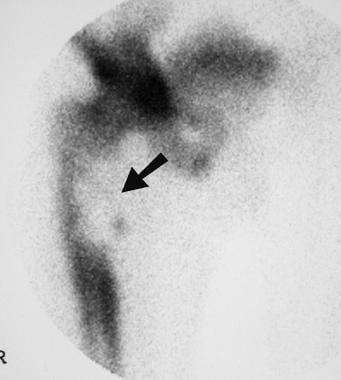 Localized isotopic bone scan in the same patient (patient with Paget disease) shows a large area of reduced uptake in the medial side of the proximal femoral shaft at the site of the secondary sarcoma (arrow).
Localized isotopic bone scan in the same patient (patient with Paget disease) shows a large area of reduced uptake in the medial side of the proximal femoral shaft at the site of the secondary sarcoma (arrow).
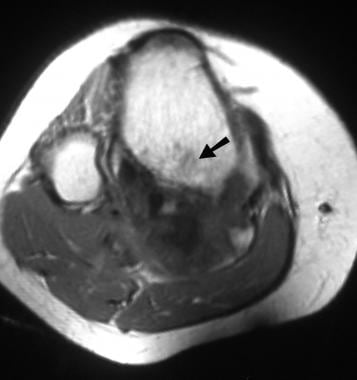
 Coronal T1-weighted magnetic resonance imaging (MRI) scan of the same patient (patient with Paget disease). The tumor is shown in the proximal shaft of the right femur (white arrow), with cortical destruction and a large soft-tissue component (black arrow).
Coronal T1-weighted magnetic resonance imaging (MRI) scan of the same patient (patient with Paget disease). The tumor is shown in the proximal shaft of the right femur (white arrow), with cortical destruction and a large soft-tissue component (black arrow).
Radiography
Telangiectatic osteosarcoma is generally lytic, with a periosteal reaction and soft-tissue mass. When the tumor margins are well defined, it may mimic an aneurysmal bone cyst. Small-cell osteosarcoma appears similar to a conventional osteosarcoma; it often has mixed areas of sclerosis and lysis. Intraosseous low-grade osteosarcoma may be lytic, sclerotic, or mixed; it often has deceptively benign features of well-defined margins and the absence of periosteal changes or a soft-tissue mass.
Gnathic tumors may be lytic, sclerotic, or mixed, and bone destruction, periosteal reaction, and soft-tissue extension are common. Intracortical osteosarcomas are described as radiolucent and geographic, and they contain a small amount of internal mineralization. High-grade surface osteosarcomas are shown as broad-based soft-tissue masses with varying degrees of mineralization arising from the surface of the bone.
Parosteal osteosarcomas are typically densely ossified tumors arising from a broad base on the adjacent bone. Unlike osteochondromas, parosteal osteosarcomas involve no continuation of the medullary cavity into the tumor.
Computed Tomography
CT scanning is helpful in the evaluation of a variety of the osteosarcoma variants. It may demonstrate fluid levels in telangiectatic osteosarcoma, and a contrast-enhanced CT scan can be helpful in discriminating such a lesion from an aneurysmal bone cyst. Telangiectatic osteosarcoma differs from an aneurysmal bone cyst in that the former has a rim of tumor cells that surrounds the cystic spaces. This tissue rim shows typically nodular enhancement after the intravenous administration of contrast material.
CT scanning is useful in the evaluation of bone changes occurring in areas of complex anatomy. Examples are the changes in the maxilla or mandible that are associated with gnathic osteosarcoma and those in the pelvis that are associated with secondary osteosarcoma. CT scanning provides useful information about the surface osteosarcoma variants, including parosteal, periosteal, and surface high-grade tumors.
Gnathic osteosarcomas occur with Paget disease or fibrous dysplasia or as a late sequela to craniofacial radiotherapy. On CT, thin irregular spicules of new bone formation are seen that are perpendicular to the epicenter of the lesion (ie, the sunburst appearance). Three-dimensional CT reconstruction and MRI can be helpful in planning surgical treatment of the lesion. [17, 11, 12]
When appropriate and performed in consultation with an orthopedic oncologist, CT scanning can be useful in guiding biopsy.
Magnetic Resonance Imaging
MRI is the optimum technique for local staging of osteosarcomas. In certain cases, MRI is combined with CT scanning. MRI accurately demonstrates the extent of a tumor within bone and soft tissue. [14, 15, 21, 22]
At least 1 sequence, either a T1-weighted or a short-tau inversion recovery (STIR) sequence, should be performed to image the entire bone. This is necessary to exclude skip lesions that are present within the same bone but are distant from the primary lesion. Periosteal osteosarcoma is typically a chondroblastic lesion, and the tumor usually has high signal intensity on T2-weighted MRIs. [23, 5]
MRI is more sensitive than CT scanning in demonstrating fluid-fluid levels in telangiectatic osteosarcoma because of its greater intrinsic soft-tissue contrast. Fluid-fluid levels can be seen in benign bone lesions as well, particularly aneurysmal bone cysts.
Histologic confirmation of the nature of the tumor is required [13] ; the analysis should be performed after MRI and in consultation with the tumor surgeon. Biopsy must be performed after the MRI study because hemorrhage occurring at the time of biopsy alters the signal intensity characteristics of the tumor at subsequent MRI examinations. The site of the biopsy track must be planned to prevent contaminating the muscle compartments that the surgeon would not otherwise excise. The biopsy track is removed during surgery, and consideration should be given to marking the track with suture material or dye if there will be a delay between biopsy and formal excision.
Telangiectatic osteosarcoma is a rare high-grade malignant neoplasm accounting for less than 4% of all cases of osteosarcoma, and MRI is the best modality for identifying the multilocular cysts and the fluid-level sign. T1-weighted MRI shows heterogeneous low signal intensity, and T2-weighted images show high signal intensity with cystic foci, fluid levels, and extraskeletal extension of tumor. The criteria for telangiectatic osteosarcoma include a destructive, osteolytic tumor with little or no matrix mineralization or periosteal new bone formation; a cystic, cavitary gross specimen with little solid tumor tissue and no areas of dense bone; and single or multiple cystic cavities containing blood or necrotic tissue and septa composed of anaplastic tumor cells. [6, 22, 7, 8]
Assessing treatment response
Oka et al evaluated whether the average apparent diffusion coefficient (ADC) or the minimum ADC provides a better assessment of patient response to chemotherapeutic osteosarcoma treatment. [21] Diffusion-weighted and MRI scans were performed on 22 patients with osteosarcoma, before and after chemotherapy, using the average and minimum ADCs. The authors found that in patients who responded well to chemotherapy, the minimum ADC ratio (using the prechemotherapy and postchemotherapy scan results) was significantly higher than it was in patients who responded poorly to treatment. However, the average ADC ratio was not significantly different between good and poor responders. The authors concluded that the minimum ADC is a better tool than the average ADC for evaluating the chemotherapeutic response of patients with osteosarcoma.
Nuclear Imaging
Osteosarcomas typically show increased uptake of radioisotope; this characteristic makes bone scans sensitive but not specific. Bone scans are most useful in excluding multifocal disease. Multiple-gated acquisition (MUGA) cardiac scans may be required to monitor the toxic effects of certain chemotherapeutic agents. [1]
In a retrospective study, Kaste et al estimated the likelihood of developing second cancers and of related mortality in pediatric patients undergoing thallium-201 (201Tl) bone imaging for osteosarcoma. [24] The study's 73 patients each underwent three 201Tl studies, receiving a median dose of 4.4 mCi (162.8 MBq) (range, 2.2-8.4 mCi [81.4-310.8 MBq]) per study. Males received a total median cumulative radiation dose of 18.6 rem (186 mSv) (range, 8.4-44.2 rem [84-442 mSv]), and females received a total of 21.5 rem (215 mSv) (range, 7.0-43.8 rem [70-438 mSv]).
The authors estimated that the incidence of excess cancers was as follows [24] :
-
Exposure to 201Tl imaging by age 5 years: 6.0 cancers per 100 males; 13.0 cancers per 100 females
-
Exposure by age 15 years: 2.0 cancers per 100 males; 3.1 cancers per 100 females
The estimated mortality resulting from these excess cancers was as follows [24] :
-
Exposure to 201Tl by age 5 years: 3.0 deaths per 100 males; 5.2 deaths per 100 females
-
Exposure by age 15 years: 1.0 deaths per 100 for males; 1.4 deaths per 100 for females
The authors concluded that reduction of 201Tl exposure will be necessary before thallium becomes a viable means of imaging osteosarcoma in younger patients. [24]
-
Frontal radiograph of the distal femur in a patient with telangiectatic osteosarcoma. The radiograph shows mixed medullary sclerosis and lucency, cortical destruction medially, aggressive periosteal changes, and a large soft-tissue mass with peripheral ossification.
-
Coronal short-tau inversion recovery (STIR) magnetic resonance imaging (MRI) scan of the same patient (patient with telangiectatic osteosarcoma). Note the abnormal signal intensity of the bone marrow in the metaphysis of the femur, the cortical destruction, and the prominent soft-tissue mass with the surrounding edema or reactive zone.
-
Axial T2-weighted magnetic resonance imaging (MRI) scan of the same patient (patient with telangiectatic osteosarcoma). A fluid-fluid level is present within the abnormal extraosseous tumor mass (arrow). The abnormal intramedullary tissue is less obvious in this sequence than in others.
-
Lateral radiograph of the proximal tibia in a patient with parosteal osteosarcoma. Note the opaque, lobulated, amorphous or cloudlike mass of abnormal, ossified tumor, which is inseparable from the posterior aspect of the tibia.
-
Axial computed tomography (CT) scan of the same patient (patient with parosteal osteosarcoma). The ossified tumor mass is readily shown, and the thickened cortex is visible at the junction of tumor and normal bone (arrow). The medullary cavity of the tibia appears normal.
-
Axial T1-weighted magnetic resonance imaging (MRI) scan of the same patient (patient with parosteal osteosarcoma). The medullary cavity of the tibia shows predominantly normal signal intensity, except posteriorly, where the slightly reduced signal intensity raises the possibility of early tumoral invasion (arrow). This area was normal on histologic examination.
-
Anteroposterior (AP) radiograph of the proximal tibia in a child with periosteal osteosarcoma. The metal pointer localizes the lesion for biopsy.
-
Coronal short-tau inversion recovery (STIR) magnetic resonance imaging (MRI) scan of the same patient (child with periosteal osteosarcoma). The ossified component of the tumor shows low signal intensity (white arrow), but superficially, hyperintense material (black arrow) is present. This may be chondroblastic soft-tissue extension of tumor, adjacent reactive edema, or a combination of both.
-
Frontal radiograph of the mandible in an adult with gnathic osteosarcoma. The radiograph shows a large, expansile lesion in the right ramus (arrow), with a mixed lytic and sclerotic appearance.
-
Axial computed tomography (CT) scan obtained with bone window settings, in the same patient (adult with gnathic osteosarcoma). Osseous expansion and the mixed lytic and sclerotic process are again appreciated. A large soft-tissue component (arrow) also is now visible.
-
Axial computed tomography (CT) scan obtained with soft-tissue window settings, in the same patient (adult with gnathic osteosarcoma). Extension of ossified matrix into the soft-tissue component of the tumor is shown (arrow).
-
Anteroposterior (AP) radiograph of the proximal femur in a patient with Paget disease demonstrates the typical features of cortical thickening, osseous expansion, and trabecular coarsening. In addition, irregular bone lucency and cortical destruction are shown in the medial aspect of the shaft; this is consistent with secondary sarcoma formation.
-
Localized isotopic bone scan in the same patient (patient with Paget disease) shows a large area of reduced uptake in the medial side of the proximal femoral shaft at the site of the secondary sarcoma (arrow).
-
Coronal T1-weighted magnetic resonance imaging (MRI) scan of the same patient (patient with Paget disease). The tumor is shown in the proximal shaft of the right femur (white arrow), with cortical destruction and a large soft-tissue component (black arrow).






