Practice Essentials
For the patient with a traumatized acetabulum, accurate radiographic diagnosis and classification are the cornerstones of effective clinical care. Acetabular fractures are caused by high kinetic energy, and satisfactory management requires differentiation of the fracture types. The classification system of Judet and Letournel has led to improved management of such injuries. [1, 2, 3, 4] However, trauma-related acetabular fractures are often complex, with multiple fragments and secondary fracture lines. Computed tomography (CT) provides information regarding the extent of the fracture and is complementary to radiography for ascertaining the spatial arrangement of fracture fragments. Three-dimensional (3D) reconstruction of CT data can be helpful in understanding the complex fracture patterns.
Acetabular fractures are often complex injuries and the result of high-energy trauma with associated injuries. Understanding and classification of these rare injuries using radiography can be difficult and are much facilitated by the addition of CT. Using multidetector CT (MDCT) with two-dimensional (2D) multiplanar reformatted (MPR) images and 3D volume-rendered images, the supplemental oblique radiographic Judet views can usually be omitted. MDCT is an indispensable tool in preoperative imaging of acetabular fractures, as well as postoperative imaging in complicated cases. MDCT is excellent for detailed imaging of fracture extent, joint congruency, step-offs or gaps in the joint surface, and entrapped osteochondral fragments. [1, 5, 6]
Most acetabular fractures occur in the setting of significant trauma secondary to either a moving vehicular accident or a high-velocity acute-deceleration injury. Blunt force is exerted on the femur, is transmitted through the femoral head, and is transferred to the acetabulum. The direction and magnitude of the force, as well as the position of the femoral head, determine the pattern of acetabular injury. The determination of the pattern of injury is key to the classification of an acetabular fracture, which, in turn, is critical to yield the highest quality orthopedic surgical treatment and therapy.
Once the acetabular fracture is classified, appropriate therapy may be planned and implemented. [7, 8, 9, 10, 11] The anatomy of the acetabulum and computed tomography (CT) images of fractures are depicted below.
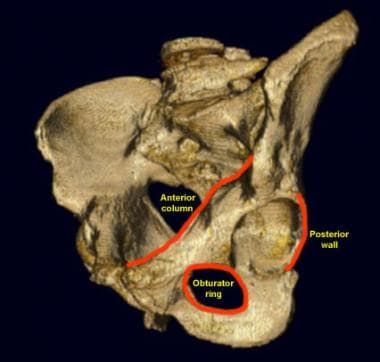
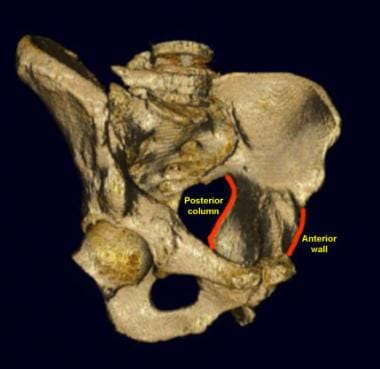
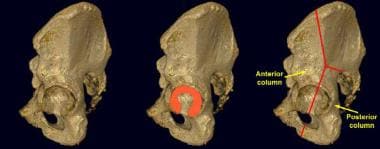 Lateral view of the left acetabulum. The left femur has been removed. The articular surface of the acetabulum is in the shape of an inverted horseshoe (outlined in red). The anterior column of the acetabulum includes most of the iliac wing, the anterior acetabulum, and the superior pubic ramus. The posterior column begins at the sciatic notch and includes the posterior portion of the acetabulum and the ischium.
Lateral view of the left acetabulum. The left femur has been removed. The articular surface of the acetabulum is in the shape of an inverted horseshoe (outlined in red). The anterior column of the acetabulum includes most of the iliac wing, the anterior acetabulum, and the superior pubic ramus. The posterior column begins at the sciatic notch and includes the posterior portion of the acetabulum and the ischium.
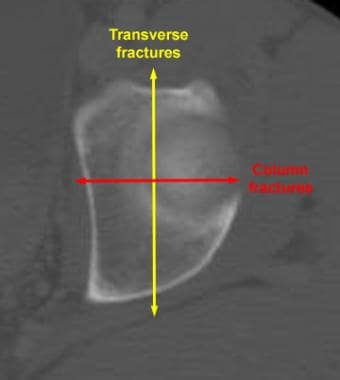 Acetabular fracture orientation with a computed tomography (CT) scan. A CT scan of the left acetabulum obtained at the level of the dome shows that transverse-type acetabular fractures have a vertical (sagittal) orientation. Column-type fractures have a horizontal (coronal) orientation.
Acetabular fracture orientation with a computed tomography (CT) scan. A CT scan of the left acetabulum obtained at the level of the dome shows that transverse-type acetabular fractures have a vertical (sagittal) orientation. Column-type fractures have a horizontal (coronal) orientation.
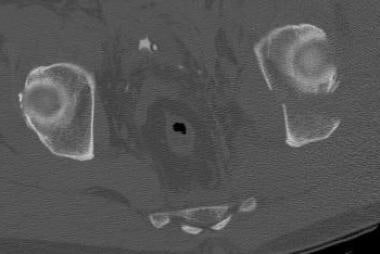
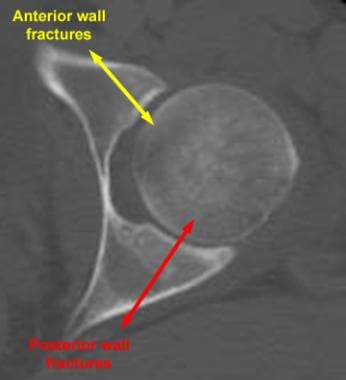 Acetabular fracture orientation with a computed tomography (CT) scan. A CT scan of the left midacetabulum shows that wall fractures have an oblique orientation.
Acetabular fracture orientation with a computed tomography (CT) scan. A CT scan of the left midacetabulum shows that wall fractures have an oblique orientation.
Mortality and morbidity
The events leading to acetabular fracture are of a nature such that contiguous bones, soft tissues, visceral organs, arteries, veins, and nerves are potentially injured. Open and closed fractures may occur, with the former predisposing to cellulitis, soft tissue/myopathic infection, superficial and deep abscesses, osteomyelitis, and vascular compromise and hemorrhage. Neurologic complications are well described.
The National Sample Program (NSP) of the National Trauma Databank was queried to identify all patients who sustained pelvic and acetabular fractures. The NSP contained 41,297 cases of pelvic trauma. In-hospital mortality was documented in 3,055 (7%) and one or more complications occurred in 6,932 (17%). Cardiac events transpired in 2% of patients, venous thromboembolic disease (VTED) in 4%, and infections in 3%. [12]
Increasing age, shock, time to procedure, and Glasgow Coma Scale (GCS) rating were predictive of mortality. Cardiac events were found to be influenced by obesity, diabetes, Injury Severity Score (ISS), GCS score, age, and trauma mechanism. VTED was impacted by obesity, history of respiratory disease, male sex, GCS score, and medical comorbidities. Injuries caused by mechanisms other than blunt trauma, shock, age, GCS score, and medical comorbidities were associated with infection.
Acetabular fractures are often associated with knee injuries. In one study, of 1273 patients with acetabular fractures, 193 (15%) were found to have ipsilateral knee symptoms within a period of 1 year from the date of injury, including 56 fractures (29%), 49 ligamentous lesions (25%), and 88 miscellaneous (46%) injuries, including bone bruises, wounds, and swelling. In the 193 cases of knee injury, other injuries included 85 patients with ipsilateral hip dislocation (45%), 59 pelvic injuries (31%), 61 extremity injuries (32%), 38 head injuries (20%), 37 chest injuries (20%), 23 abdominal and genitourinary injuries (12%), and 7 injuries of the spine (4%). [13]
Sex- and age-related considerations
Sex-related considerations
Acetabular and pelvic fractures occur in both men and women, but they are more common in men.
A low-energy fracture results in a fracture of the acetabulum without disrupting pelvic alignment (nondisplaced fracture), while a high-energy fracture may disrupt both the acetabulum and the overall alignment of the pelvic ring, and it is likely to lead to associated damage to the organs contained within the pelvis.
However, extension of force and subsequent tissue known to extend into the central, lower, and retroperitoneal portions of the pelvis will disrupt a different cadre of organs in men (posterior urethra, prostate, seminal vesicles) than occurs in women (posterior urethra, cervix, uterus, broad ligament, fallopian tubes and ovaries).
Of the 31,380 patients with pelvic fractures, 1,444 had genitourinary injury. Men more commonly sustained pelvic fractures with genitourinary injury than women (66.14% vs 33.86%). The incidence of urogenital, bladder, and urethral injuries for men and women was 5.34%, 3.41%, and 1.54%, respectively in men, and 3.62%, 3.37%, and 0.15%, respectively in women.
Age-related considerations
The primary cause in younger individuals is high-energy trauma. Fractures secondary to moderate or minimal trauma are increasingly of concern in those older than 35 years or in those with osteopenia/osteomalacia from a chronic underlying cause.
Radiographic anatomy
The anteroposterior (AP) view of the pelvis is the primary tool for radiographic evaluation of the acetabulum (see the images below). The iliopectineal, or iliopubic, line is the radiographic landmark for the anterior column. It begins at the sciatic notch and travels along the superior pubic ramus to the symphysis pubis. The ilioischial line demarcates the posterior column. It also begins at the sciatic notch, coursing inferiorly to the medial border of the ischium. The ilioischial line should pass through the acetabular teardrop. If it does not overlap the teardrop, the ilioischial line and, thus, the posterior column are disrupted. [14]
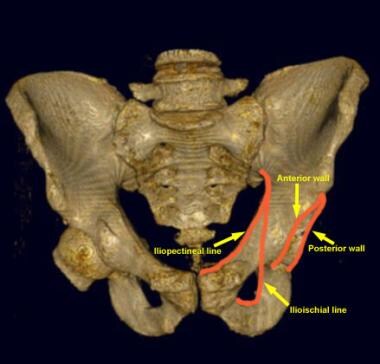 Anteroposterior view of the pelvis. The left femur has been removed for illustration purposes. The iliopectineal, or iliopubic, line is an important landmark for examining the anterior column of the acetabulum. The ilioischial line demarcates the medial border of the posterior column. The posterior wall of the acetabulum is larger and projects more laterally than does the anterior wall.
Anteroposterior view of the pelvis. The left femur has been removed for illustration purposes. The iliopectineal, or iliopubic, line is an important landmark for examining the anterior column of the acetabulum. The ilioischial line demarcates the medial border of the posterior column. The posterior wall of the acetabulum is larger and projects more laterally than does the anterior wall.
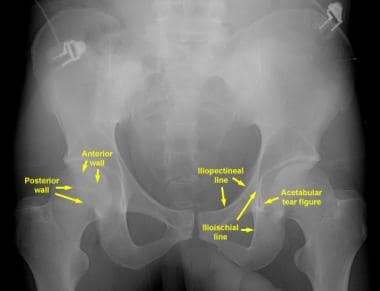 Anteroposterior (AP) radiograph of the pelvis. The iliopectineal (or iliopubic) and ilioischial lines serve as landmarks for the anterior and posterior columns, respectively. The larger and more lateral posterior wall is visualized more easily than is the smaller, more medial anterior wall. The acetabular tear figure is a composite shadow of the inferomedial structures that compose the acetabulum. The ilioischial line should pass through the teardrop on a true AP view of the pelvis.
Anteroposterior (AP) radiograph of the pelvis. The iliopectineal (or iliopubic) and ilioischial lines serve as landmarks for the anterior and posterior columns, respectively. The larger and more lateral posterior wall is visualized more easily than is the smaller, more medial anterior wall. The acetabular tear figure is a composite shadow of the inferomedial structures that compose the acetabulum. The ilioischial line should pass through the teardrop on a true AP view of the pelvis.
The iliac wing is considered to be part of the anterior column. An iliac wing fracture in the setting of an acetabular injury indicates anterior column involvement. An iliac oblique radiograph provides a better view of the iliac wing. The posterior wall of the acetabulum is more visible than the anterior wall on the AP view because of its more lateral position. The anterior wall may be difficult to appreciate on the AP view.
The obturator oblique view better depicts the posterior wall, and the iliac oblique view better depicts the anterior wall. The integrity of the obturator ring is an important feature to recognize. Certain fracture patterns (such as those of column and T-shaped fractures) characteristically include fractures through the obturator ring.
The oblique, or Judet, views of the pelvis are named relative to the side of interest (see the images below). [15, 16] For example, if the acetabular fracture is on the left side, the views are named with reference to the left side. The left posterior oblique radiograph displays the iliac wing en face; therefore, this view is termed the left iliac oblique view (see the image below). The right posterior oblique radiograph shows the obturator ring en face; therefore, this view is the left obturator oblique view. The iliac oblique view clearly demonstrates the iliac wing, sciatic notch, and ischial spine. In addition, the posterior column and anterior wall of the acetabulum are seen in profile.
 Left obturator oblique view of the pelvis. The left obturator ring is seen en face. The anterior column and posterior wall of the left acetabulum are profiled in this position.
Left obturator oblique view of the pelvis. The left obturator ring is seen en face. The anterior column and posterior wall of the left acetabulum are profiled in this position.
 Left iliac oblique view of the pelvis. The left iliac wing is demonstrated en face. The left posterior column and the anterior wall are seen in profile.
Left iliac oblique view of the pelvis. The left iliac wing is demonstrated en face. The left posterior column and the anterior wall are seen in profile.
The obturator oblique radiograph provides the best depiction of the obturator ring and shows the anterior column and posterior wall in profile.
Clinical details
Unfortunately, patients with fractures of the pelvis and/or acetabulum almost always also experience serious injury to surrounding soft tissue (skin and muscles) and neurovascular structures (nerves, arteries and veins). In addition, especially in the case of pelvic fractures, adjacent organs can be seriously injured. With both types of fracture, there is significant bleeding and risk of nerve damage.
In patients with multiple injuries, treatment begins with the trauma team at the scene and then subsequently in the emergency department (ED)—a team of general surgeons, anesthesiologists and nurses—who work together to control bleeding, address damage to the head and chest and other organs that may have been affected (eg, bladder, intestines), and to stabilize broken bones. During this early resuscitation phase of treatment, the orthopaedic surgeon may need to stabilize the fracture by using an external frame to temporarily hold the bones in proper alignment while other problems are treated. This is called temporary external fixation. Surgeons construct these frames using steel pins that are inserted into the bone and joined together by clamps and rods and can do so very rapidly.
Once the patient is stabilized—bleeding has stopped and other life-threatening injuries have been addressed—the fractures can be treated definitively. Successful treatment for both of these types of fractures requires the skills of an interdisciplinary team, with orthopedic surgeons working closely with the trauma team (general surgeons), the anesthesiologists, and nurses. Following surgery, rehabilitation specialists play a key role in recovery.
Because of the complex nature of these fractures and because many orthopedic surgeons do not regularly treat them, patients who initially go to a community hospital for emergency attention are often transferred to an institution that specializes in such injuries.
Classification
Fractures of the acetabulum are most commonly classified according to the system described by Judet and colleagues. [2] The system is based on the orientation of the fractures and the structures involved. In this system, the orientation of the fracture is based on its depiction on a lateral view of the acetabulum. In order to arrive at the correct classification, AP and oblique (Judet) radiographs of the pelvis are obtained and analyzed. [2, 3, 15, 17, 16] (See the image below.)
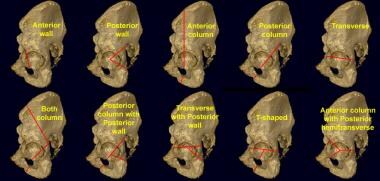 Acetabular fracture classification system. Judet and colleagues (1964) described the classification scheme that is most commonly used today. Of the 10 types, 5 are elementary fractures (top row), and 5 are associated fractures (bottom row). Elementary types involve 1 primary fracture plane. Associated types involve more than 1 fracture plane.
Acetabular fracture classification system. Judet and colleagues (1964) described the classification scheme that is most commonly used today. Of the 10 types, 5 are elementary fractures (top row), and 5 are associated fractures (bottom row). Elementary types involve 1 primary fracture plane. Associated types involve more than 1 fracture plane.
Some authors have questioned the necessity of oblique views of the pelvis in the age of multidetector CT scanning. Harris and colleagues have proposed a new classification system based on the multidetector CT scan appearance. [3] Other authors have defended the utility of the standard radiographic series in the evaluation of acetabular fractures. The Judet system will be presented in the remainder of this article. [2, 15]
In the system described by Judet and colleagues, 10 patterns of acetabular fracture are defined. The 10 patterns are divided into 5 elementary and 5 associated patterns. [15, 18, 16]
Elementary patterns include fractures with a single fracture orientation, whereas associated patterns usually involve combinations of the elementary fractures. Elementary patterns include anterior wall, posterior wall, anterior column, posterior column, and transverse fractures. Associated patterns include both-column fractures, posterior column fractures with posterior wall fractures, transverse fractures with posterior wall fractures, T-shaped fractures, and anterior column fractures with posterior hemitransverse fractures.
For simplicity, the 10 patterns can be grouped into 3 categories: wall, column, and transverse fractures. Some fractures fit into 2 categories. The following fractures are indicated by pattern type.
Wall fractures
Wall fractures include the following:
-
Anterior wall
-
Posterior wall
-
Posterior column with posterior wall (also a column fracture)
-
Transverse with posterior wall (also a transverse fracture)
Column fractures
Column fractures include the following:
-
Anterior column
-
Posterior column
-
Both-column
-
Posterior column with posterior wall (also a wall fracture)
-
Anterior column with posterior hemitransverse (also a transverse fracture)
Transverse fractures
Transverse fractures include the following:
-
Transverse
-
T-shaped
-
Transverse with posterior wall (also a wall fracture)
-
Anterior column with posterior hemitransverse (also a column fracture)
Fracture patterns
Isolated acetabular wall fractures typically do not involve the weight-bearing articular portion of the acetabulum. Fractures of the posterior wall are more common than are those of the anterior wall because of the preponderance of posteriorly directed forces responsible for acetabular fractures. Posterior wall fractures may occur in isolation (see the first three images below) or in combination with posterior column or transverse fractures. Anterior wall fractures are rare (see the last image below).
 Posterior wall acetabular fracture. Anteroposterior radiograph of the pelvis. The posterior wall of the left acetabulum is disrupted (arrow).
Posterior wall acetabular fracture. Anteroposterior radiograph of the pelvis. The posterior wall of the left acetabulum is disrupted (arrow).
 Posterior wall acetabular fracture. A left obturator oblique radiograph of the pelvis. The posterior wall fracture (arrow) is better depicted on this view than on the anteroposterior view.
Posterior wall acetabular fracture. A left obturator oblique radiograph of the pelvis. The posterior wall fracture (arrow) is better depicted on this view than on the anteroposterior view.
 Computed tomography (CT) scan of a posterior wall acetabular fracture. The oblique fracture of the left acetabulum is clearly depicted. The degree of displacement and marginal impaction can be determined more accurately with CT scanning than with radiography.
Computed tomography (CT) scan of a posterior wall acetabular fracture. The oblique fracture of the left acetabulum is clearly depicted. The degree of displacement and marginal impaction can be determined more accurately with CT scanning than with radiography.
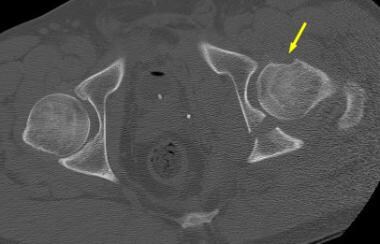
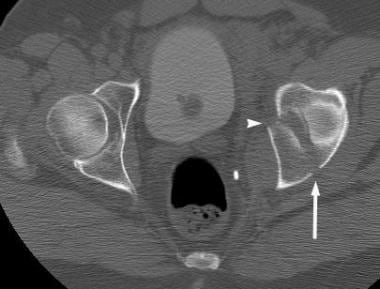
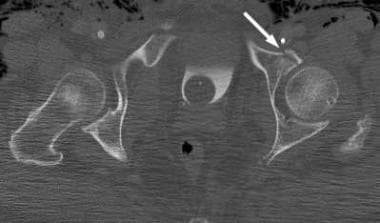 Anterior wall acetabular fracture. A computed tomography (CT) scan demonstrates an oblique fracture through the anterior wall of the left acetabulum (arrow). Such fractures are uncommon in isolation. The patient had other pelvic injuries.
Anterior wall acetabular fracture. A computed tomography (CT) scan demonstrates an oblique fracture through the anterior wall of the left acetabulum (arrow). Such fractures are uncommon in isolation. The patient had other pelvic injuries.
Both-column fractures are the most common acetabular injury. As the name implies, the anterior and posterior columns are involved. On AP radiographs, a disruption of the iliopectineal and ilioischial lines, as well as the obturator ring, may be seen (see the first image below). An iliac wing fracture may be seen on the AP view, but often, it is appreciated only on the iliac oblique radiograph (see the second image below). The pathognomonic spur sign is present on the obturator oblique view (see the third image below) and confirmed on a CT scan (see the last 3 images below).
 Both-column acetabular fracture. An anteroposterior radiograph of the pelvis shows that the right ilioischial and iliopectineal lines are completely disrupted. A right iliac wing fracture is noted above the level of the acetabulum (arrow). A nondisplaced fracture of the right inferior pubic ramus is subtle.
Both-column acetabular fracture. An anteroposterior radiograph of the pelvis shows that the right ilioischial and iliopectineal lines are completely disrupted. A right iliac wing fracture is noted above the level of the acetabulum (arrow). A nondisplaced fracture of the right inferior pubic ramus is subtle.
 Both-column acetabular fracture. A right iliac oblique radiograph of the pelvis. The posterior column (arrowhead) and iliac wing disruptions are shown.
Both-column acetabular fracture. A right iliac oblique radiograph of the pelvis. The posterior column (arrowhead) and iliac wing disruptions are shown.
 Both-column acetabular fracture. A right obturator oblique radiograph of the pelvis best depicts nondisplaced fractures of the obturator ring (arrowheads). The iliopectineal line disruption (short arrow) signifies anterior column involvement. The pathognomonic spur sign (long arrow) of the both-column fracture is best appreciated on this view. The spur represents a strut of bone extending from the sacroiliac joint. The fracture of both columns disconnects this piece of bone from the acetabulum and causes its spurlike appearance.
Both-column acetabular fracture. A right obturator oblique radiograph of the pelvis best depicts nondisplaced fractures of the obturator ring (arrowheads). The iliopectineal line disruption (short arrow) signifies anterior column involvement. The pathognomonic spur sign (long arrow) of the both-column fracture is best appreciated on this view. The spur represents a strut of bone extending from the sacroiliac joint. The fracture of both columns disconnects this piece of bone from the acetabulum and causes its spurlike appearance.
 Both-column acetabular fracture. A computed tomography (CT) scan obtained at the level of the sacroiliac joints shows that the horizontal (coronal) column fracture begins superiorly at the iliac wing in the both-column fracture. The CT scan equivalent of the spur sign can be seen (arrow).
Both-column acetabular fracture. A computed tomography (CT) scan obtained at the level of the sacroiliac joints shows that the horizontal (coronal) column fracture begins superiorly at the iliac wing in the both-column fracture. The CT scan equivalent of the spur sign can be seen (arrow).
 Both-column acetabular fracture. A computed tomography (CT) scan obtained just above the level of the acetabular dome shows that the CT scan spur sign is present (arrow).
Both-column acetabular fracture. A computed tomography (CT) scan obtained just above the level of the acetabular dome shows that the CT scan spur sign is present (arrow).
 Both-column acetabular fracture. A computed tomography (CT) scan obtained at the level of the acetabular dome shows the CT scan spur sign (arrow). Note how this spur does not connect to the articular portion of the acetabulum. In a both-column fracture, the articular surface of the acetabulum is completely disconnected from the axial skeleton.
Both-column acetabular fracture. A computed tomography (CT) scan obtained at the level of the acetabular dome shows the CT scan spur sign (arrow). Note how this spur does not connect to the articular portion of the acetabulum. In a both-column fracture, the articular surface of the acetabulum is completely disconnected from the axial skeleton.
Isolated anterior and posterior column fractures are uncommon. Anterior column fractures disrupt the iliopectineal line while preserving the ilioischial line. Conversely, posterior column fractures disrupt the ilioischial line but not the iliopectineal line (see the images below).
 Posterior column acetabular fracture. An anteroposterior radiograph of the pelvis shows that the left femoral head is dislocated posteriorly. The ilioischial line is broken, but the iliopectineal line remains intact.
Posterior column acetabular fracture. An anteroposterior radiograph of the pelvis shows that the left femoral head is dislocated posteriorly. The ilioischial line is broken, but the iliopectineal line remains intact.
 Posterior column acetabular fracture. Compared with the anteroposterior view, the left obturator oblique radiograph of the pelvis better depicts the posteriorly displaced posterior column, posterior wall, and femoral head.
Posterior column acetabular fracture. Compared with the anteroposterior view, the left obturator oblique radiograph of the pelvis better depicts the posteriorly displaced posterior column, posterior wall, and femoral head.
 Posterior column acetabular fracture. A left iliac oblique radiograph of the pelvis shows that the posterior column is markedly displaced.
Posterior column acetabular fracture. A left iliac oblique radiograph of the pelvis shows that the posterior column is markedly displaced.
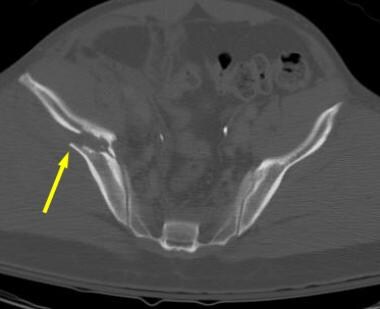
 Computed tomography (CT) scan of a posterior column acetabular fracture at the level of the acetabular dome. The characteristic horizontal (coronal) orientation of the column fracture is appreciated easily by using CT scanning.
Computed tomography (CT) scan of a posterior column acetabular fracture at the level of the acetabular dome. The characteristic horizontal (coronal) orientation of the column fracture is appreciated easily by using CT scanning.
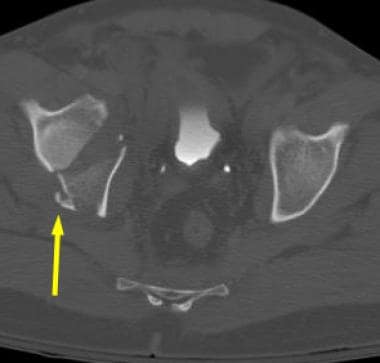
 Posterior column acetabular fracture. A computed tomography (CT) scan obtained at the level of the midacetabulum shows the horizontally oriented column fracture. The femoral head is relocated, but the recent posterior dislocation is evident in the anterior impaction fracture (arrow).
Posterior column acetabular fracture. A computed tomography (CT) scan obtained at the level of the midacetabulum shows the horizontally oriented column fracture. The femoral head is relocated, but the recent posterior dislocation is evident in the anterior impaction fracture (arrow).
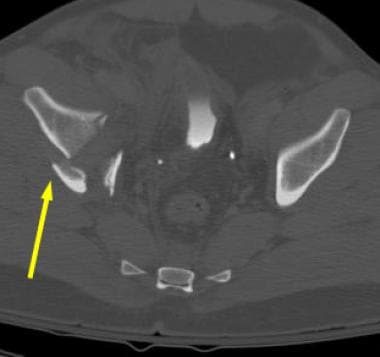
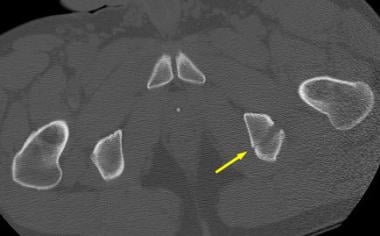 Posterior column acetabular fracture. A computed tomography (CT) scan obtained at the level of the ischial tuberosities shows that posterior column fractures sometimes can exit through the ischial tuberosity (arrow) rather than through the obturator ring.
Posterior column acetabular fracture. A computed tomography (CT) scan obtained at the level of the ischial tuberosities shows that posterior column fractures sometimes can exit through the ischial tuberosity (arrow) rather than through the obturator ring.
Column fractures divide the acetabulum into front and back halves (see the first image below). The posterior column fracture with a posterior wall fracture has the features of each of its components (see the second image below). The slightly more common anterior column fracture with a posterior hemitransverse fracture is the most complex acetabular fracture to classify.
Acetabular fracture orientation with a computed tomography (CT) scan. A CT scan of the left acetabulum obtained at the level of the dome shows that transverse-type acetabular fractures have a vertical (sagittal) orientation. Column-type fractures have a horizontal (coronal) orientation.
Acetabular fracture classification system. Judet and colleagues (1964) described the classification scheme that is most commonly used today. Of the 10 types, 5 are elementary fractures (top row), and 5 are associated fractures (bottom row). Elementary types involve 1 primary fracture plane. Associated types involve more than 1 fracture plane.
The combination of column fractures and transverse fractures may be difficult to appreciate radiographically (see the first image below). The iliopectineal and ilioischial lines are broken, and an iliac wing fracture should be evident. Unlike the both-column fracture, which shares these features, the obturator ring is intact and the spur sign is not present. On CT scans, the anterior column and the posterior transverse fracture planes may be appreciated (see the second image below).
 Anterior column fracture with a posterior hemitransverse acetabular fracture. An anteroposterior radiograph of the pelvis shows disruption of the iliopectineal (long arrow) and ilioischial (short arrows) lines. The obturator ring is intact.
Anterior column fracture with a posterior hemitransverse acetabular fracture. An anteroposterior radiograph of the pelvis shows disruption of the iliopectineal (long arrow) and ilioischial (short arrows) lines. The obturator ring is intact.
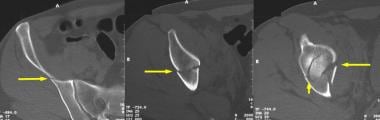 Anterior column fracture with a posterior hemitransverse acetabular fracture, as depicted on computed tomography (CT) scans obtained above and at the level of the right acetabulum. Left: The image shows an iliac wing fracture (arrow) that was not appreciated on the anteroposterior radiograph. (The oblique radiographs were not of good quality.) Middle: The image clearly depicts a column-type fracture (arrow) that is oriented horizontally on the CT scans. Right: The image again demonstrates the column fracture (long arrow), but now a transverse (vertically oriented) fracture can be seen posteriorly (short arrow).
Anterior column fracture with a posterior hemitransverse acetabular fracture, as depicted on computed tomography (CT) scans obtained above and at the level of the right acetabulum. Left: The image shows an iliac wing fracture (arrow) that was not appreciated on the anteroposterior radiograph. (The oblique radiographs were not of good quality.) Middle: The image clearly depicts a column-type fracture (arrow) that is oriented horizontally on the CT scans. Right: The image again demonstrates the column fracture (long arrow), but now a transverse (vertically oriented) fracture can be seen posteriorly (short arrow).
Transverse fractures are transverse because of their appearance when the acetabulum is examined from the lateral view. The iliopectineal and ilioischial lines are interrupted, but the obturator ring is spared. On CT scans, the fracture is oriented vertically (front to back).
Transverse fractures divide the acetabulum into top and bottom halves, as seen on the lateral view of the acetabulum. The transverse fracture with a posterior wall fracture is a common fracture that incorporates the features of transverse and posterior wall elementary fractures (see the images below).
 Transverse with posterior wall acetabular fracture. An anteroposterior radiograph of the pelvis shows that the central dislocation of the left femoral head results in the disruption of the iliopectineal and ilioischial lines. In addition, the left posterior acetabular wall is disrupted.
Transverse with posterior wall acetabular fracture. An anteroposterior radiograph of the pelvis shows that the central dislocation of the left femoral head results in the disruption of the iliopectineal and ilioischial lines. In addition, the left posterior acetabular wall is disrupted.
 Transverse fracture with a posterior wall acetabular fracture. Compared with the anteroposterior view, this left obturator oblique view of the pelvis view better demonstrates the anterior column and posterior wall disruption. The obturator ring is intact.
Transverse fracture with a posterior wall acetabular fracture. Compared with the anteroposterior view, this left obturator oblique view of the pelvis view better demonstrates the anterior column and posterior wall disruption. The obturator ring is intact.
 Computed tomography (CT) scan of a transverse fracture with a posterior wall acetabular fracture. The vertically oriented transverse fracture (arrow) of the left acetabulum is well depicted on CT scans. Note the oblique posterior wall fracture (arrowhead). Posterior wall fractures often are associated with femoral head dislocation.
Computed tomography (CT) scan of a transverse fracture with a posterior wall acetabular fracture. The vertically oriented transverse fracture (arrow) of the left acetabulum is well depicted on CT scans. Note the oblique posterior wall fracture (arrowhead). Posterior wall fractures often are associated with femoral head dislocation.
The T-shaped fracture is a fairly common acetabular injury. This fracture has the characteristics of an elementary transverse fracture with the addition of a medial acetabular wall fracture extending through the obturator ring (see the images below). The anterior column with posterior hemitransverse fracture is discussed earlier.
 T-shaped acetabular fracture. An anteroposterior radiograph of the pelvis shows that a transverse fracture (arrows) disrupts the left iliopectineal and ilioischial lines. The obturator ring also is interrupted (arrowheads). No iliac wing fracture is seen above the level of the acetabulum.
T-shaped acetabular fracture. An anteroposterior radiograph of the pelvis shows that a transverse fracture (arrows) disrupts the left iliopectineal and ilioischial lines. The obturator ring also is interrupted (arrowheads). No iliac wing fracture is seen above the level of the acetabulum.
 Computed tomography (CT) scan of T-shaped acetabular fracture. The transverse portion of the fracture has a vertical (sagittal) orientation (arrow). The extension of the fracture through the medial wall represents the stem of the T (arrowhead). More inferior CT scans demonstrated the obturator ring fractures.
Computed tomography (CT) scan of T-shaped acetabular fracture. The transverse portion of the fracture has a vertical (sagittal) orientation (arrow). The extension of the fracture through the medial wall represents the stem of the T (arrowhead). More inferior CT scans demonstrated the obturator ring fractures.
In a study by Brandser and colleagues, the following 3 most common types of acetabular fracture accounted for roughly two thirds of all fractures: both-column fractures, transverse fractures with posterior wall fractures, and posterior wall fractures. [19, 20] This number increased to 90% when the next 2 most common fracture types were considered: T-shaped and transverse fractures. The frequency of the fractures types is described below.
Commonly occurring acetabular fractures (90%) include the following:
-
Both-column
-
Transverse with posterior wall
-
Posterior wall
-
T-shaped
-
Transverse
Uncommonly occurring acetabular fractures (10%) include the following:
-
Anterior column
-
Anterior column with posterior hemitransverse
-
Posterior column with posterior wall
-
Posterior column
-
Anterior wall
Preferred examinations
Radiography
AP radiography of the pelvis is used in the initial radiographic assessment of patients with major trauma that is suggestive of pelvic and/or acetabular injury (see the images below). Images are obtained with the patient in the supine position and with the radiographic beam passing in an AP direction. This is the typical first radiographic examination performed, as a patient may arrive on a stretcher in the hospital ED in acute, severe pain and extremis, and time is of the essence to establish an immediate working diagnosis. Abnormalities depicted on the AP pelvis radiograph direct the need for the next set of radiographs, if indicated. Acetabular fractures are imaged by using bilateral oblique (ie, Judet) views of the pelvis. Pelvic ring fractures are imaged by using inlet and outlet views of the pelvis.
Anteroposterior view of the pelvis. The left femur has been removed for illustration purposes. The iliopectineal, or iliopubic, line is an important landmark for examining the anterior column of the acetabulum. The ilioischial line demarcates the medial border of the posterior column. The posterior wall of the acetabulum is larger and projects more laterally than does the anterior wall.
Anteroposterior (AP) radiograph of the pelvis. The iliopectineal (or iliopubic) and ilioischial lines serve as landmarks for the anterior and posterior columns, respectively. The larger and more lateral posterior wall is visualized more easily than is the smaller, more medial anterior wall. The acetabular tear figure is a composite shadow of the inferomedial structures that compose the acetabulum. The ilioischial line should pass through the teardrop on a true AP view of the pelvis.
In a retrospective review of 133 patients who underwent acetabular revision for pelvic discontinuity, preoperative radiographic studies were reviewed, including anteroposterior pelvis (AP; N = 133), true lateral hip (N = 132), Judet (N = 47), false profile (N = 4), and computed tomography scans (N = 14). Using only the AP view, the fracture line was visible in 116 (87%), medial migration of the inferior hemipelvis in 126 (95%), and obturator ring asymmetry in 114 (86%). A fracture line was visualized in 65 of 132 hips (49%) evaluated with laterals, 36 of 47 hips (77%) evaluated with Judet views, 3 of 4 (75%) evaluated with a false profile view, and 10 of 14 (71%) evaluated with computed tomography. [21]
Oblique, or Judet, radiographs of the pelvis are obtained with the patient in the left posterior oblique and right posterior oblique positions (see the images below). The patient should be at a 45º angle relative to the radiographic beam, which remains perpendicular to the cassette. This technique results in 2 orthogonal radiographs of the pelvis. The patient must be moved to the oblique position; the radiographic tube is not moved so as to be at a 45º angle relative to the patient and film cassette. Angling the tube results in unacceptable radiographic distortion.
Left obturator oblique view of the pelvis. The left obturator ring is seen en face. The anterior column and posterior wall of the left acetabulum are profiled in this position.
Left iliac oblique view of the pelvis. The left iliac wing is demonstrated en face. The left posterior column and the anterior wall are seen in profile.
A common mistake in this radiographic technique is the positioning of the patient in an oblique position that is not steep enough, with a resultant angle of less than 45º. On an oblique view obtained with good positioning, with the aid of a blocking device or on-site technologist to hold the patient in place, the coccyx should project over the femoral head.
CT scanning
Pelvic CT scans may be obtained alone or in combination with abdominal CT scans during the initial trauma evaluation. Pelvic CT scans allow the detection of subtle fractures and displacements that are not appreciated on radiographs. [22] Axial CT scans may be obtained, but helical CT scanning yields better 2D and 3D reformatted images. [18]
In a retrospective review of suspected occult hip fractures detected by CT or MRI following negative radiographs, of 179 patients investigated (mean age, 82±13 years), the ultimate diagnosis was an occult hip fracture in 71 cases and pelvic or acetabular fracture in 34 cases. The average time to further imaging was 2.0±2.7 days but was significantly shorter for CT. [23]
As opposed to older CT scanners, newer scanners use 2D axial helical continuous volumetric acquisitions of patient anatomy. Using MDCT with 2D MPR images and 3D volume rendering is the current state of the art for image acquisition in North America. Sixteen-, 32-, 64-, 128-, and 256-slice scanners are widely available at the time of authorship. After fast axial image acquisition over 15-25 seconds, depending on equipment, the "slab" of continuous anatomy is then created during the image reconstruction phase, during which image reformatting may occur, allowing the patient to leave the CT suite and be transported to another area to be treated for his or her injuries.
Rapid image acquisition is important in acutely injured, unstable patients with highly painful injuries, as it allows for rapid scan times, decreased motion artifact, and large volumes of tissue acquired in a single setting.
Traditional classification into anterior column, posterior column, and complex 2-column fractures is facilitated. CT is especially useful in evaluation of the 2-column fractures in which unique information concerning the configuration of the fracture and integrity of the acetabular dome and quadrilateral surface can be obtained. Helical CT scanning is also useful in determining the presence or absence of loose bodies in the joint. Evaluation of the femoral head and sacroiliac joint is also emphasized, as these structures may participate in the traumatic process. Fracture may occur in any part of the proximal femoral metaepiphysis, or fracture extension into the sacroiliac joint and/or distraction forces that create sacroiliac joint space widening.
Virtually all acetabular fractures may be correctly classified after careful interpretation of AP and oblique radiographs of the pelvis. However, excellent patient care does not stop at simple fracture classification. Intra-articular fracture fragments may be difficult to recognize on radiographs, as are loose bodies, subtle clinically significant malalignment, and fracture extension outside of the region of the hip joint proper.
Compared with radiography, pelvic CT scanning allows a more precise determination of the degree of articular involvement, as well as of fragment displacement and orientation. As above, pelvic CT scanning also permits the identification of intra-articular fracture fragments. In complex acetabular fractures, 3D reformatted images, so-called "virtual imaging" of the acetabular and pelvic bones, may help conceptualize the fracture pattern and thereby aid in the planning of orthopedic surgical intervention.
Limitations of techniques
All techniques are limited to the size and disposition of the patient. Many CT gantries have a weight limitation approaching 500 lb. Depending on the height, weight, and girth of the patient, the penetration of the x-ray beam varies, and larger patients have increasing image graininess, decreased signal-to-noise ratio, narrowing of the gray scale, and streak artifact off bowel and bony prominences.
Additionally, patient motion tends to blur and degrade the images. This is particularly important in the setting of high-velocity trauma and an acutely traumatized patient, as patients must lie on an x-ray table or CT gantry and are much less likely to hold still during an examination when in a great deal of pain.
Radiography
According to Brandser and Marsh, [20] the following radiographic observations can be used to determine the acetabular fracture pattern and the correct classification of most acetabular fractures:
-
A fracture of the obturator ring indicates either a T-shaped or a column fracture (with the exception of the hemitransverse type of fracture). An intact obturator ring eliminates these fractures from consideration.
-
Disruption of the ilioischial line occurs in fractures involving the posterior column or fractures in the transverse group.
-
Disruption of the iliopectineal line indicates anterior column involvement or one of the transverse-type fractures.
-
Iliac wing fractures are observed in fractures involving the anterior column.
-
Posterior wall fractures may occur in isolation or in combination with posterior column or transverse fractures.
-
The spur sign is observed exclusively in the both-column fracture. The spur is a strut of bone extending from the sacroiliac joint. Usually, this strut of bone connects to the articular surface of the acetabulum. In the both-column fracture, this connection is disrupted; a fractured piece of bone that resembles a spur remains.
The spur sign is best depicted on the obturator oblique view (see the first image below). In addition, the spur sign can be appreciated on CT scans (see the second image below).
Both-column acetabular fracture. A right obturator oblique radiograph of the pelvis best depicts nondisplaced fractures of the obturator ring (arrowheads). The iliopectineal line disruption (short arrow) signifies anterior column involvement. The pathognomonic spur sign (long arrow) of the both-column fracture is best appreciated on this view. The spur represents a strut of bone extending from the sacroiliac joint. The fracture of both columns disconnects this piece of bone from the acetabulum and causes its spurlike appearance.
Both-column acetabular fracture. A computed tomography (CT) scan obtained at the level of the sacroiliac joints shows that the horizontal (coronal) column fracture begins superiorly at the iliac wing in the both-column fracture. The CT scan equivalent of the spur sign can be seen (arrow).
Table 1 shows the combined set of radiographic and CT scan observations that are useful in acetabular fracture classification.
Table 1. Radiographic Features of Acetabular Fracture Types [20] (Open Table in a new window)
Fracture Type |
Obturator Ring Fracture |
Ilioischial Line Disrupted |
Iliopectineal Line Disrupted |
Iliac Wing Fracture |
Posterior Wall Fracture |
Pelvis Into Halves |
Spur Sign |
CT Scan Fracture Orientation |
Both-column |
Yes |
Yes |
Yes |
Yes |
No |
Front/back |
Yes |
Horizontal |
Anterior column |
Yes |
No |
Yes |
Yes |
No |
Front/back |
No |
Horizontal |
Posterior column |
Yes |
Yes |
No |
No |
No |
Front/back |
No |
Horizontal |
Posterior column with posterior wall |
Yes |
Yes |
No |
No |
Yes |
Front/back |
No |
Horizontal |
T-shaped |
Yes |
Yes |
Yes |
No |
No |
Top/bottom |
No |
Vertical |
Transverse with posterior wall |
No |
Yes |
Yes |
No |
Yes |
Top/bottom |
No |
Vertical |
Transverse |
No |
Yes |
Yes |
No |
No |
Top/bottom |
No |
Vertical |
Posterior wall |
No |
No |
No |
No |
Yes |
No |
No |
Oblique |
Anterior wall |
No |
No |
Yes |
No |
No |
No |
No |
Oblique |
Anterior column with posterior hemitransverse |
No |
Yes |
Yes |
Yes |
No |
N/A* |
No |
N/A |
*N/A indicates not applicable. |
||||||||
By using Brandser and Marsh's system, the accurate classification of acetabular fractures is possible in almost every patient. [20]
An accessory ossification center, the os acetabulum, may mimic an acetabular wall fracture. Its differentiating features include its characteristic superolateral location and well-corticated margins. Fractures of the anterior puboacetabular junction may be observed in pelvic ring fractures. These fractures may extend into the anterior column of the acetabulum, but they are not anterior column fractures per se. Such fractures are more correctly considered to be superior pubic ramus fractures.
Computed Tomography
Brandser and Marsh described several CT scan–based observations in the classification of acetabular fractures. The following may help in the classification of these fractures [20] :
-
Transverse-type fractures divide the acetabulum into top and bottom halves, as seen from the lateral perspective of the acetabulum. Column fractures divide the acetabulum into front and back halves. Isolated wall fractures do not divide the acetabulum. In other words, is the CT scan spur sign present? Only the both-column fracture causes the spur sign.
-
Transverse-type fractures have a vertical (sagittal) CT scan orientation. Column fractures have a horizontal (coronal) orientation. Wall fractures are oriented obliquely.
CT scan features of acetabulum fractures are demonstrated below.
Acetabular fracture orientation with a computed tomography (CT) scan. A CT scan of the left midacetabulum shows that wall fractures have an oblique orientation.
Computed tomography (CT) scan of a transverse fracture with a posterior wall acetabular fracture. The vertically oriented transverse fracture (arrow) of the left acetabulum is well depicted on CT scans. Note the oblique posterior wall fracture (arrowhead). Posterior wall fractures often are associated with femoral head dislocation.
Posterior column acetabular fracture. A computed tomography (CT) scan obtained at the level of the midacetabulum shows the horizontally oriented column fracture. The femoral head is relocated, but the recent posterior dislocation is evident in the anterior impaction fracture (arrow).
Both-column acetabular fracture. A computed tomography (CT) scan obtained just above the level of the acetabular dome shows that the CT scan spur sign is present (arrow).
Table 1 shows the combined set of radiographic and CT scan observations that are useful in acetabular fracture classification. (See Radiograph.)
Durkee and colleagues presented an algorithm for classification of the 5 most common types of acetabular fracture based on several observations. [9] The observations are similar to those presented in Table 1. [9]
Interpreted in conjunction with the pelvic radiographs, CT scans allow accurate fracture classification and appropriate surgical planning, as well as training in the diagnosis of acetabulum fractures. [24, 18, 25]
In a retrospective study of 300 acetabular fractures diagnosed by CT, femoral head fracture was found more likely to be present in patients with a posterior wall component of the fracture or associated hip dislocation. [18]
Magnetic Resonance Imaging
Magnetic resonance imaging (MRI) is not routinely used in the primary evaluation of acetabular fractures. Potter and colleagues described the use of MRI in the evaluation of occult femoral head injuries and in the detection of subclinical sciatic nerve injury. [26] Intra-articular fracture fragments may be missed on magnetic resonance images.
MRI is a valuable tool for these fractures because it can not only detect the fractures and the planes in which they course through the complex pelvic anatomy but also detect and gauge the extent of the adjacent soft tissue component of injury to muscle, ligament, tendon, fascia, acetabular labrum, and the investing fat planes.
Currently, the use of MRI in imaging deep venous thrombosis in patients with pelvic or lower extremity injuries is being evaluated. Magnetic resonance venography may be useful in depicting lower extremity and pelvic venous thrombosis. [27, 28, 29, 30]
Questions & Answers
Overview
What are acetabulum fractures?
What is the morbidity and mortality associated with acetabulum fractures?
How do acetabulum fractures differ between males and females?
How do acetabulum fractures differ between younger patients and those older than 35 years?
What is the anatomy of the pelvis relevant to acetabulum fractures?
What is the initial treatment of acetabulum fractures?
How are acetabulum fractures classified?
What are the patterns of acetabulum fractures seen on radiographs?
What are the most common types of acetabulum fractures?
What are the least common types of acetabulum fractures?
What is the role of radiography in the workup of acetabulum fractures?
What is the role of CT scans in the workup of acetabulum fractures?
What are the limitations of acetabulum fracture imaging?
Which findings on radiographs are characteristic of acetabulum fractures?
Which findings on CT scans are characteristic of acetabulum fractures?
Which findings on MRI are characteristic of acetabulum fractures?
-
Lateral view of the left acetabulum. The left femur has been removed. The articular surface of the acetabulum is in the shape of an inverted horseshoe (outlined in red). The anterior column of the acetabulum includes most of the iliac wing, the anterior acetabulum, and the superior pubic ramus. The posterior column begins at the sciatic notch and includes the posterior portion of the acetabulum and the ischium.
-
Anteroposterior view of the pelvis. The left femur has been removed for illustration purposes. The iliopectineal, or iliopubic, line is an important landmark for examining the anterior column of the acetabulum. The ilioischial line demarcates the medial border of the posterior column. The posterior wall of the acetabulum is larger and projects more laterally than does the anterior wall.
-
Anteroposterior (AP) radiograph of the pelvis. The iliopectineal (or iliopubic) and ilioischial lines serve as landmarks for the anterior and posterior columns, respectively. The larger and more lateral posterior wall is visualized more easily than is the smaller, more medial anterior wall. The acetabular tear figure is a composite shadow of the inferomedial structures that compose the acetabulum. The ilioischial line should pass through the teardrop on a true AP view of the pelvis.
-
Left obturator oblique view of the pelvis. The left obturator ring is seen en face. The anterior column and posterior wall of the left acetabulum are profiled in this position.
-
Left iliac oblique view of the pelvis. The left iliac wing is demonstrated en face. The left posterior column and the anterior wall are seen in profile.
-
Acetabular fracture classification system. Judet and colleagues (1964) described the classification scheme that is most commonly used today. Of the 10 types, 5 are elementary fractures (top row), and 5 are associated fractures (bottom row). Elementary types involve 1 primary fracture plane. Associated types involve more than 1 fracture plane.
-
Acetabular fracture orientation with a computed tomography (CT) scan. A CT scan of the left acetabulum obtained at the level of the dome shows that transverse-type acetabular fractures have a vertical (sagittal) orientation. Column-type fractures have a horizontal (coronal) orientation.
-
Acetabular fracture orientation with a computed tomography (CT) scan. A CT scan of the left midacetabulum shows that wall fractures have an oblique orientation.
-
Anterior wall acetabular fracture. A computed tomography (CT) scan demonstrates an oblique fracture through the anterior wall of the left acetabulum (arrow). Such fractures are uncommon in isolation. The patient had other pelvic injuries.
-
Posterior wall acetabular fracture. Anteroposterior radiograph of the pelvis. The posterior wall of the left acetabulum is disrupted (arrow).
-
Posterior wall acetabular fracture. A left obturator oblique radiograph of the pelvis. The posterior wall fracture (arrow) is better depicted on this view than on the anteroposterior view.
-
Computed tomography (CT) scan of a posterior wall acetabular fracture. The oblique fracture of the left acetabulum is clearly depicted. The degree of displacement and marginal impaction can be determined more accurately with CT scanning than with radiography.
-
Transverse with posterior wall acetabular fracture. An anteroposterior radiograph of the pelvis shows that the central dislocation of the left femoral head results in the disruption of the iliopectineal and ilioischial lines. In addition, the left posterior acetabular wall is disrupted.
-
Transverse fracture with a posterior wall acetabular fracture. Compared with the anteroposterior view, this left obturator oblique view of the pelvis view better demonstrates the anterior column and posterior wall disruption. The obturator ring is intact.
-
Computed tomography (CT) scan of a transverse fracture with a posterior wall acetabular fracture. The vertically oriented transverse fracture (arrow) of the left acetabulum is well depicted on CT scans. Note the oblique posterior wall fracture (arrowhead). Posterior wall fractures often are associated with femoral head dislocation.
-
T-shaped acetabular fracture. An anteroposterior radiograph of the pelvis shows that a transverse fracture (arrows) disrupts the left iliopectineal and ilioischial lines. The obturator ring also is interrupted (arrowheads). No iliac wing fracture is seen above the level of the acetabulum.
-
Computed tomography (CT) scan of T-shaped acetabular fracture. The transverse portion of the fracture has a vertical (sagittal) orientation (arrow). The extension of the fracture through the medial wall represents the stem of the T (arrowhead). More inferior CT scans demonstrated the obturator ring fractures.
-
Posterior column acetabular fracture. An anteroposterior radiograph of the pelvis shows that the left femoral head is dislocated posteriorly. The ilioischial line is broken, but the iliopectineal line remains intact.
-
Posterior column acetabular fracture. Compared with the anteroposterior view, the left obturator oblique radiograph of the pelvis better depicts the posteriorly displaced posterior column, posterior wall, and femoral head.
-
Posterior column acetabular fracture. A left iliac oblique radiograph of the pelvis shows that the posterior column is markedly displaced.
-
Computed tomography (CT) scan of a posterior column acetabular fracture at the level of the acetabular dome. The characteristic horizontal (coronal) orientation of the column fracture is appreciated easily by using CT scanning.
-
Posterior column acetabular fracture. A computed tomography (CT) scan obtained at the level of the midacetabulum shows the horizontally oriented column fracture. The femoral head is relocated, but the recent posterior dislocation is evident in the anterior impaction fracture (arrow).
-
Posterior column acetabular fracture. A computed tomography (CT) scan obtained at the level of the ischial tuberosities shows that posterior column fractures sometimes can exit through the ischial tuberosity (arrow) rather than through the obturator ring.
-
Both-column acetabular fracture. An anteroposterior radiograph of the pelvis shows that the right ilioischial and iliopectineal lines are completely disrupted. A right iliac wing fracture is noted above the level of the acetabulum (arrow). A nondisplaced fracture of the right inferior pubic ramus is subtle.
-
Both-column acetabular fracture. A right iliac oblique radiograph of the pelvis. The posterior column (arrowhead) and iliac wing disruptions are shown.
-
Both-column acetabular fracture. A right obturator oblique radiograph of the pelvis best depicts nondisplaced fractures of the obturator ring (arrowheads). The iliopectineal line disruption (short arrow) signifies anterior column involvement. The pathognomonic spur sign (long arrow) of the both-column fracture is best appreciated on this view. The spur represents a strut of bone extending from the sacroiliac joint. The fracture of both columns disconnects this piece of bone from the acetabulum and causes its spurlike appearance.
-
Both-column acetabular fracture. A computed tomography (CT) scan obtained at the level of the sacroiliac joints shows that the horizontal (coronal) column fracture begins superiorly at the iliac wing in the both-column fracture. The CT scan equivalent of the spur sign can be seen (arrow).
-
Both-column acetabular fracture. A computed tomography (CT) scan obtained just above the level of the acetabular dome shows that the CT scan spur sign is present (arrow).
-
Both-column acetabular fracture. A computed tomography (CT) scan obtained at the level of the acetabular dome shows the CT scan spur sign (arrow). Note how this spur does not connect to the articular portion of the acetabulum. In a both-column fracture, the articular surface of the acetabulum is completely disconnected from the axial skeleton.
-
Anterior column fracture with a posterior hemitransverse acetabular fracture. An anteroposterior radiograph of the pelvis shows disruption of the iliopectineal (long arrow) and ilioischial (short arrows) lines. The obturator ring is intact.
-
Anterior column fracture with a posterior hemitransverse acetabular fracture, as depicted on computed tomography (CT) scans obtained above and at the level of the right acetabulum. Left: The image shows an iliac wing fracture (arrow) that was not appreciated on the anteroposterior radiograph. (The oblique radiographs were not of good quality.) Middle: The image clearly depicts a column-type fracture (arrow) that is oriented horizontally on the CT scans. Right: The image again demonstrates the column fracture (long arrow), but now a transverse (vertically oriented) fracture can be seen posteriorly (short arrow).
Tables
Fracture Type |
Obturator Ring Fracture |
Ilioischial Line Disrupted |
Iliopectineal Line Disrupted |
Iliac Wing Fracture |
Posterior Wall Fracture |
Pelvis Into Halves |
Spur Sign |
CT Scan Fracture Orientation |
Both-column |
Yes |
Yes |
Yes |
Yes |
No |
Front/back |
Yes |
Horizontal |
Anterior column |
Yes |
No |
Yes |
Yes |
No |
Front/back |
No |
Horizontal |
Posterior column |
Yes |
Yes |
No |
No |
No |
Front/back |
No |
Horizontal |
Posterior column with posterior wall |
Yes |
Yes |
No |
No |
Yes |
Front/back |
No |
Horizontal |
T-shaped |
Yes |
Yes |
Yes |
No |
No |
Top/bottom |
No |
Vertical |
Transverse with posterior wall |
No |
Yes |
Yes |
No |
Yes |
Top/bottom |
No |
Vertical |
Transverse |
No |
Yes |
Yes |
No |
No |
Top/bottom |
No |
Vertical |
Posterior wall |
No |
No |
No |
No |
Yes |
No |
No |
Oblique |
Anterior wall |
No |
No |
Yes |
No |
No |
No |
No |
Oblique |
Anterior column with posterior hemitransverse |
No |
Yes |
Yes |
Yes |
No |
N/A* |
No |
N/A |
*N/A indicates not applicable. |
||||||||









