Practice Essentials
Temporal lobe epilepsy is the most common epilepsy syndrome in adults. Seizures usually begin in late childhood or adolescence. Virtually all patients have complex partial seizures, some of which generalize secondarily. In most patients, the epileptogenic focus involves the structures of the mesial temporal lobe (illustrated in the diagrams below). The structures of the mesial temporal lobe include the hippocampus, amygdala, and parahippocampal gyrus. Antiepileptogenic drugs usually suppress secondary generalized seizures successfully, but 50% of patients or more will continue to have partial seizures. When seizures persist, anterior temporal lobectomy is the treatment of choice. [1, 2]
Neuroimaging is vital for the identification of organic or structural anomalies, which may precipitate temporal lobe seizures, such as vascular malformations, tumors, and hippocampal sclerosis. Coronal oblique MRI through the temporal lobes is the preferred modality for temporal lobe biopsy. Thin, coronal, oblique slices of 1.5–2 mm with no gap, using spoiled gradient recall images (SPGR) are recommended. Patients with newly diagnosed temporal lobe epilepsy should have a high-resolution MRI scan with at least a 1.5-Tesla MRI. [3] Nuclear medicine scans (positron emission tomography [PET] scans or single-photon emission computed tomography [SPECT] scans) and electroencephalograms (EEGs) also play a role in localization. MRI is contraindicated in patients with pacemakers, certain metal prostheses (eg, cochlear implants), or a large number of cerebral aneurysm clips. Metallic foreign bodies within the eyes, as well as shrapnel or bullets when they are located near vascular structures, also are contraindications. [3, 4, 5, 6, 7, 8, 9, 10, 11, 12]
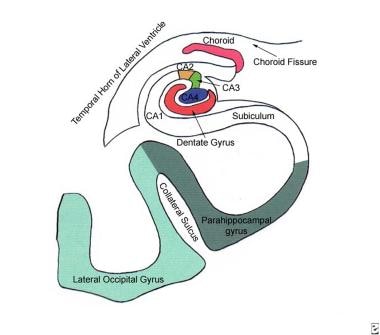 Diagram of the hippocampal anatomy and adjacent structures in the mesial temporal lobe. The cornu ammonis, a part of the hippocampus, can be divided into four fields: CA1, CA2, CA3, and CA4.
Diagram of the hippocampal anatomy and adjacent structures in the mesial temporal lobe. The cornu ammonis, a part of the hippocampus, can be divided into four fields: CA1, CA2, CA3, and CA4.
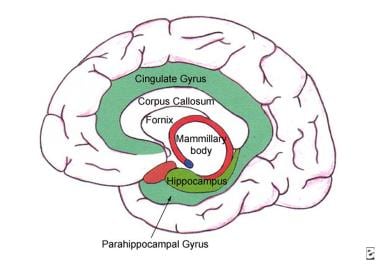 Anatomic diagram depicts the relationship of the hippocampus to other structures in the limbic system. Note that the cingulate gyrus is continuous with the parahippocampal gyrus.
Anatomic diagram depicts the relationship of the hippocampus to other structures in the limbic system. Note that the cingulate gyrus is continuous with the parahippocampal gyrus.
Chernov et al found that single-voxel proton magnetic resonance spectroscopy (MRS)–detected reduction of N-acetylaspartate content and unilateral presence of lactate in the mesial temporal lobe structures may serve as diagnostic clues for lateralization of the epileptogenic zone in mesial temporal lobe epilepsy. The investigators conducted a retrospective study to evaluate the role of single-voxel proton MRS in preoperative investigation of patients with mesial temporal lobe epilepsy. Metabolic imaging was found to have limited usefulness for differentiation of the hippocampal sclerosis and low-grade intra-axial brain tumor. In addition, the presence of significant bilateral metabolic alterations in the mesial temporal lobe structures was associated with worse postoperative seizure control. [4]
Investigators found that 3T magnetic resonance imaging (MRI) had better interobserver agreement, in a study comparing 3T with 1.5T phased array MRI in the presurgical workup of patients with epilepsy with complex focus localization. In the report, by Zijlmans et al, 3T was found to reveal more dysplasias, while 1.5T revealed more tissue loss and mesial temporal sclerosis. According to the authors, patients can benefit most from 3T scans when a dysplasia is suspected, and they advised reevaluation by another experienced neuroradiologist in cases of negative or equivocal MRIs. [3]
Provenzale et al confirmed that MRI findings of a markedly hyperintense hippocampus in children with febrile status epilepticus was highly associated with subsequent mesial temporal sclerosis. [5]
Focke et al explored the integrity of connecting networks using diffusion tensor imaging (DTI) and 2 whole-brain voxel-based methods: statistical parametric mapping (SPM) and tract-based spatial statistics (TBSS). DTI detected extensive changes in mesial temporal lobe epilepsy with hippocampus sclerosis. The affected networks were principally in the ipsilateral temporal lobe and the limbic system, but also in the arcuate fasciculus. SPM and TBSS provided complementary information, with higher sensitivity to fractional anisotropy changes using TBSS. [13]
Mitsueda-Ono et al concluded that high-resolution MRI suggests minute internal structural changes in the hippocampus that reflect neuronal cell loss or gliosis and more sensitively show laterality of changes. According to the study, other internal structural changes might further enable the subclassification of hippocampal sclerosis and predictions of the surgical outcomes of seizure control. [6]
Appel et al studied whether reduced resting regional cerebral blood flow affects the blood oxygen level-dependent signal during fMRI mapping and concluded that hypoperfusion in temporal lobe epilepsy does not affect fMRI clinical value. [14]
Lopez-Acevedo et al concluded that because of the large number of quantitative and quantitative variables that need to be considered in a conventional hippocampal MR report, such evaluations might benefit from predictive models generated by unconventional methods, such as discriminant analysis. [7]
Computed Tomography
Computed tomography (CT) scanning is typically insensitive for evaluation of mesial temporal sclerosis and for the workup of medically refractory epilepsy. In part, this is a result of surrounding bone artifact from the base of the skull and of the plane of acquisition.
Bronen and colleagues concluded that CT scanning is not useful for the diagnostic evaluation of medically refractory epilepsy because of the relatively low sensitivity of CT scanning compared with that of MRI in detecting abnormalities in patients undergoing surgery for medically refractory epilepsy. [15] In their study, a sensitivity of 32% was obtained for CT scanning, while MRI achieved a sensitivity of 95%. MRI was also demonstrated to be significantly better than CT scanning for the localization of mesial temporal sclerosis (98% vs 2%).
Magnetic Resonance Imaging
Classic MRI findings in mesial temporal sclerosis include decreased volume and an abnormally increased T2 signal of the hippocampus. The increased T2 signal is presumed to be a result of gliosis and the subsequent increase in free water content. [8, 9, 16] Hippocampal sclerosis is the most common abnormality observed in mesial temporal lobe epilepsy patients. The primary features of hippocampal sclerosis on MRI are volume loss on T1-weighted imaging and signal hyperintensity on T2-weighted or FLAIR sequence. [11]
(See the images below.)
 A 22-year-old patient with refractory temporal lobe epilepsy. Fluid-attenuated inversion recovery (FLAIR) magnetic resonance images of the left hippocampus show increased signal intensity and volume loss.
A 22-year-old patient with refractory temporal lobe epilepsy. Fluid-attenuated inversion recovery (FLAIR) magnetic resonance images of the left hippocampus show increased signal intensity and volume loss.
 T2-weighted magnetic resonance images reveal the increased signal and volume loss of the left hippocampus (same patient as in the image above).
T2-weighted magnetic resonance images reveal the increased signal and volume loss of the left hippocampus (same patient as in the image above).
Associated findings may include atrophy of the ipsilateral mammillary body, fornix, and other parts of the limbic system. Temporal sclerosis and atrophy are demonstrated in the images below. [17, 18]
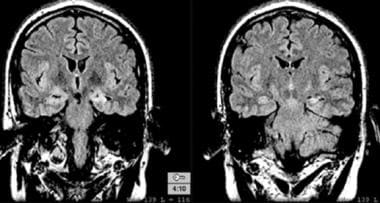
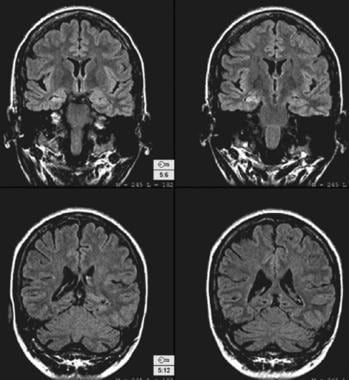 Fluid-attenuated inversion recovery (FLAIR) magnetic resonance images in a 40-year-old patient with complex partial seizures. The right hippocampus is atrophic and has increased signal intensity that is compatible with mesial temporal sclerosis. Other associated findings of mesial temporal sclerosis are present and are better demonstrated on coronal T2-weighted magnetic resonance images than they are on these images.
Fluid-attenuated inversion recovery (FLAIR) magnetic resonance images in a 40-year-old patient with complex partial seizures. The right hippocampus is atrophic and has increased signal intensity that is compatible with mesial temporal sclerosis. Other associated findings of mesial temporal sclerosis are present and are better demonstrated on coronal T2-weighted magnetic resonance images than they are on these images.
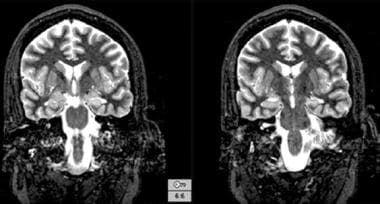
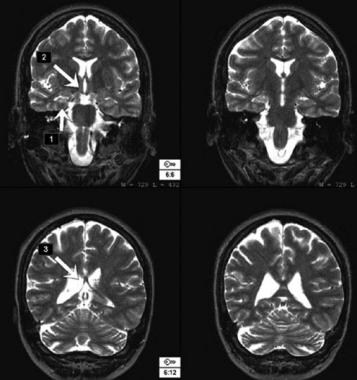 Coronal T2-weighted magnetic resonance images demonstrate mesial temporal sclerosis on the right, as well as associated findings of a small right mammillary body and a small right fornix.
Coronal T2-weighted magnetic resonance images demonstrate mesial temporal sclerosis on the right, as well as associated findings of a small right mammillary body and a small right fornix.
On coronal T2 spin-echo views (see the image below), the hippocampus is surrounded by hyperintensity from cerebrospinal fluid (CSF) in the temporal horn of the lateral ventricle, choroid fissure, and choroid plexus. This surrounding high T2 signal somewhat limits detection of T2 signal abnormality in the hippocampus.
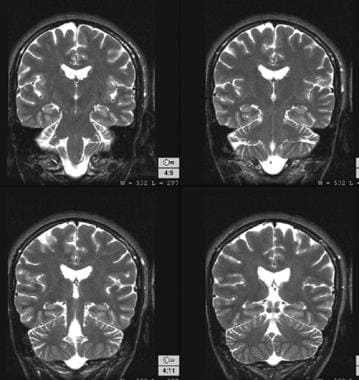 Normal findings on T2-weighted magnetic resonance images obtained through the hippocampi.
Normal findings on T2-weighted magnetic resonance images obtained through the hippocampi.
Because fluid-attenuated inversion recovery (FLAIR) imaging nulls the CSF signal, abnormal signal intensity in the hippocampus is relatively more apparent. [19] A pitfall of coronal FLAIR imaging is the slight hyperintensity of all limbic structures relative to the neocortex; therefore, experienced neuroradiologists who have knowledge of the normal signal intensity of the hippocampus are needed. A FLAIR image is demonstrated below.
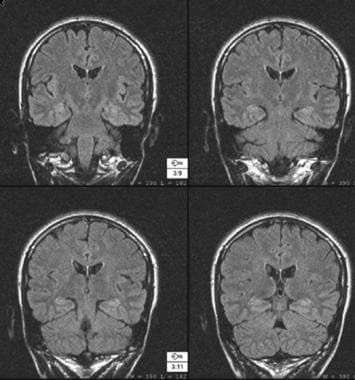 Normal findings on fluid-attenuated inversion recovery (FLAIR) magnetic resonance images obtained through the hippocampi. Note the normal, slightly increased signal intensity in the hippocampi.
Normal findings on fluid-attenuated inversion recovery (FLAIR) magnetic resonance images obtained through the hippocampi. Note the normal, slightly increased signal intensity in the hippocampi.
Thin-section volumetric T1-weighted imaging is occasionally used to calculate hippocampal volume; however, because it does not depict abnormal signal intensity, it is less useful than FLAIR and T2-weighted spin-echo imaging for visual detection of mesial temporal sclerosis.
Magnetic resonance spectroscopy (MRS) can help in lateralizing temporal lobe epilepsy. Lateralization is useful in a patient with clinical temporal lobe epilepsy but no localizing findings on MRI. As many as 20% of patients with clinical temporal lobe epilepsy have no such MRI findings.
Hydrogen-1 MRS demonstrates the anatomic distribution of metabolite signals. The metabolites frequently studied include N- acetylaspartate (a neuronal marker), creatine (a relatively stable marker found in the brain that is often used as a reference to compare with other metabolites), and choline (a marker related to cell membrane synthesis). Studies have shown that interictal N- acetylaspartate is reduced in the ipsilateral temporal lobe compared with the uninvolved temporal lobe. [20]
Degree of confidence
Routine MRI is typically insensitive to findings of mesial temporal sclerosis. McBride and colleagues compared findings of standard MRI performed outside an epilepsy center with the findings of special temporal lobe seizure protocols performed at major epilepsy centers. [21] Although routine MRI readily depicted low-grade tumors and vascular malformations, it was inadequate for diagnosing hippocampal sclerosis. This difference occurred because the hippocampal structures are relatively flat and lie predominantly in the axial plane (in which most routine sequences are performed); therefore, subtle lesions of the hippocampus may be missed.
(See the images below.)
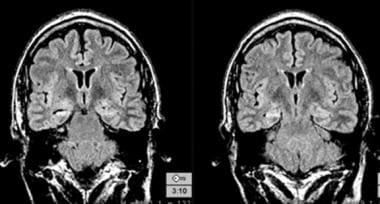 A 59-year-old patient with a history of temporal lobe epilepsy. The right hippocampus has increased signal intensity and volume loss.
A 59-year-old patient with a history of temporal lobe epilepsy. The right hippocampus has increased signal intensity and volume loss.
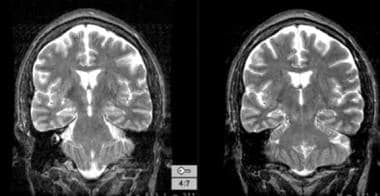 Coronal T2-weighted magnetic resonance image in a 59-year-old patient (same patient as in the above image) shows increased signal intensity and volume loss.
Coronal T2-weighted magnetic resonance image in a 59-year-old patient (same patient as in the above image) shows increased signal intensity and volume loss.
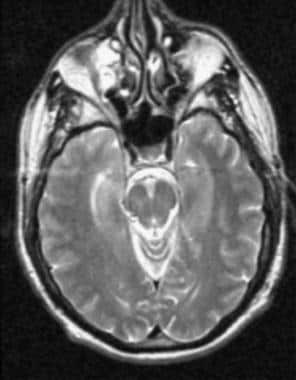 Axial magnetic resonance image in a 59-year-old patient (same patient as in the above 2 images). The right hippocampus has increased signal intensity; however, the signal intensity is less obvious in the axial plane than it is in the oblique coronal plane.
Axial magnetic resonance image in a 59-year-old patient (same patient as in the above 2 images). The right hippocampus has increased signal intensity; however, the signal intensity is less obvious in the axial plane than it is in the oblique coronal plane.
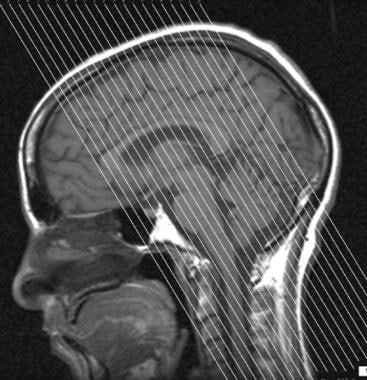
Optimized high-resolution MRI of the temporal lobes is required for reliable detection of mesial temporal sclerosis. [22] Special oblique coronal thin sections perpendicular to the plane of the hippocampus have high sensitivity and specificity for mesial temporal sclerosis. The proper plane and orientation for MRI is demonstrated in the images below.
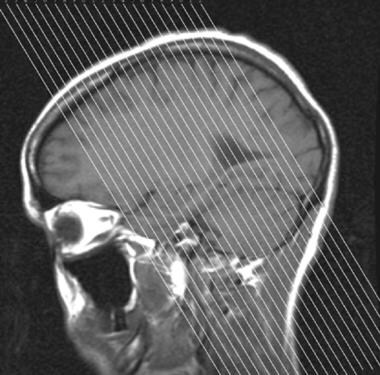 Proper magnetic resonance imaging (MRI) plane for evaluation of the hippocampus is perpendicular to its long axis.
Proper magnetic resonance imaging (MRI) plane for evaluation of the hippocampus is perpendicular to its long axis.
T2-weighted spin-echo imaging is somewhat better than FLAIR imaging for demonstrating the internal architecture of the hippocampus; however, the degree of signal abnormality is somewhat more obvious on FLAIR imaging. The advantage of FLAIR imaging is derived from the decreased background signal intensity that originates in extrahippocampal structures.
In a study performed by Berkovic and colleagues, sensitivity of MRI for mesial temporal sclerosis was as high as 97%, and specificity was 83%. [23] (Other studies have determined values of 80-90% sensitivity.) The authors reported on patients who underwent MRI and who later received anterior temporal lobectomy. Radiologic findings were correlated with pathologic findings.
Studies have been performed to assess whether an image-processing algorithm (Correlative Image Enhancement, CIE) could facilitate recognition of hippocampal signal abnormality in the presence of mesial temporal sclerosis (MTS) by increasing contrast-to-noise ratio (CNR) between affected hippocampus and normal gray matter.
In a study of baseline coronal FLAIR images from brain MRIs of 27 children with epilepsy who underwent hippocampal resection processed using CIE, processing resulted in a significant increase in mean CNR (from 3.9 ± 5.3 to 25.3 ± 25.8; P< 0.01) for hippocampi with MTS, with a substantial (>100%) increase from baseline seen in 15/19 (78.9%) cases. Baseline CNR of 1.7 ± 5.3 for normal hippocampi did not change significantly after processing (1.8 ± 5.3; P=1.00). The researchers concluded that by enhancing CNR for diseased hippocampi while leaving normal hippocampi relatively unaffected, CIE may improve the diagnostic accuracies of radiologists in detecting MTS-related signal alteration within the affected hippocampus. [24]
In a retrospective case-control study comparing pediatric MTS cases to children with no seizure history, CIE selectively increased the CNR of hippocampi affected by MTS and improved reader performance in detecting MTS-related hippocampal signal abnormality. [25]
MRI findings of mesial temporal sclerosis have also been correlated with surgical outcome. Patients with mesial temporal sclerosis that was visible on magnetic resonance images (and that was subsequently confirmed on pathology) were found to have improved postsurgical outcomes, with high seizure-free rates or substantial improvement in seizures in comparison with patients who had normal MRI findings. [23]
Nuclear Imaging
SPECT scanning and PET scanning with 18-fluorodeoxyglucose (FDG) provide functional information about the temporal lobe. PET scans show glucose metabolism in the brain by using a positron-emitting substance. Patients with temporal lobe epilepsy have decreased glucose metabolism in the affected lobe during the interictal period. SPECT scans show the distribution of blood flow in the brain at the time of the injection of a radiotracer, which is injected ictally or interictally. If the radiotracer is injected ictally, focally increased uptake is identified in the affected temporal lobe (hot focus). If the radiotracer is injected interictally, the effected temporal lobe demonstrates decreased uptake compared with that of the rest of the brain (cold focus).
Sensitivity for detection of interictal seizure foci is 65-75% for both SPECT scans and PET scans. When the source of seizures is lateralized on PET scans or SPECT scans, 94% of patients improve after surgical resection.
Two studies have shown that restricted rather than widespread hypometabolism on FDG-PET is correlated with Engel class Ia surgical outcome. [26, 27, 12]
-
Diagram of the hippocampal anatomy and adjacent structures in the mesial temporal lobe. The cornu ammonis, a part of the hippocampus, can be divided into four fields: CA1, CA2, CA3, and CA4.
-
Anatomic diagram depicts the relationship of the hippocampus to other structures in the limbic system. Note that the cingulate gyrus is continuous with the parahippocampal gyrus.
-
Proper magnetic resonance imaging (MRI) plane for evaluation of the hippocampus is perpendicular to its long axis.
-
Midline magnetic resonance image with proper section orientation.
-
Normal findings on fluid-attenuated inversion recovery (FLAIR) magnetic resonance images obtained through the hippocampi. Note the normal, slightly increased signal intensity in the hippocampi.
-
Normal findings on T2-weighted magnetic resonance images obtained through the hippocampi.
-
A 59-year-old patient with a history of temporal lobe epilepsy. The right hippocampus has increased signal intensity and volume loss.
-
Coronal T2-weighted magnetic resonance image in a 59-year-old patient (same patient as in the above image) shows increased signal intensity and volume loss.
-
Axial magnetic resonance image in a 59-year-old patient (same patient as in the above 2 images). The right hippocampus has increased signal intensity; however, the signal intensity is less obvious in the axial plane than it is in the oblique coronal plane.
-
A 22-year-old patient with refractory temporal lobe epilepsy. Fluid-attenuated inversion recovery (FLAIR) magnetic resonance images of the left hippocampus show increased signal intensity and volume loss.
-
T2-weighted magnetic resonance images reveal the increased signal and volume loss of the left hippocampus (same patient as in the image above).
-
Fluid-attenuated inversion recovery (FLAIR) magnetic resonance images in a 40-year-old patient with complex partial seizures. The right hippocampus is atrophic and has increased signal intensity that is compatible with mesial temporal sclerosis. Other associated findings of mesial temporal sclerosis are present and are better demonstrated on coronal T2-weighted magnetic resonance images than they are on these images.
-
Coronal T2-weighted magnetic resonance images demonstrate mesial temporal sclerosis on the right, as well as associated findings of a small right mammillary body and a small right fornix.






