Practice Essentials
In general, the imaging appearances of liver metastases are nonspecific, and biopsy specimens are required for histologic diagnosis. CT is the imaging modality of choice for evaluating liver metastases. This preference is largely attributable to the effects of the dual blood supply on the enhancement characteristics of metastases, as compared with normal liver parenchyma. For detection and characterization of small lesions and to evaluate the liver with background fatty liver changes, MRI may be superior to multidector CT and positron emission tomography (PET). [1, 2, 3, 4, 5]
(See the CT images of liver metastases below.)
 Liver, metastases. Characteristic appearance of carcinoid liver metastases on a contrast-enhanced axial CT scan through the upper abdomen. Portal venous phase image shows the metastases as negative defects against the normally enhancing liver
Liver, metastases. Characteristic appearance of carcinoid liver metastases on a contrast-enhanced axial CT scan through the upper abdomen. Portal venous phase image shows the metastases as negative defects against the normally enhancing liver
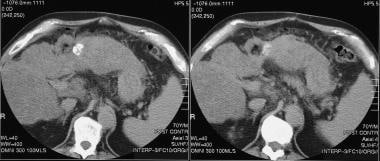
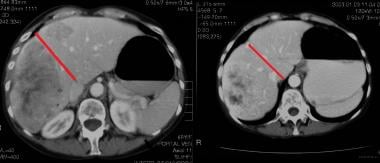 Liver, metastases. Contrast-enhanced transaxial CT images in the portal venous phase through the liver of a 48-year-old man with colonic metastases. The left image shows metastases in both lobes of the liver and, thus, inoperable. The right image was taken 2 months after oxaliplatin therapy. The metastases were downstaged. The patient underwent a successful right hepatectomy.
Liver, metastases. Contrast-enhanced transaxial CT images in the portal venous phase through the liver of a 48-year-old man with colonic metastases. The left image shows metastases in both lobes of the liver and, thus, inoperable. The right image was taken 2 months after oxaliplatin therapy. The metastases were downstaged. The patient underwent a successful right hepatectomy.
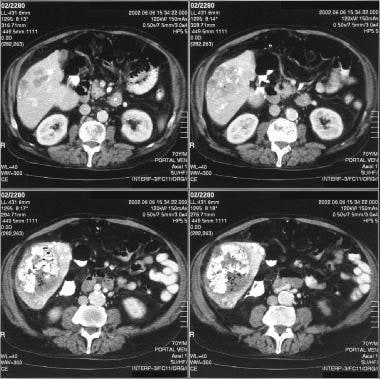
 Contrast-enhanced CT scans taken in the portal venous phase show a hypervascular metastatic deposit from a renal cell carcinoma. The patient had a previous right hepatectomy for an earlier renal cell solitary metastatic deposit.
Contrast-enhanced CT scans taken in the portal venous phase show a hypervascular metastatic deposit from a renal cell carcinoma. The patient had a previous right hepatectomy for an earlier renal cell solitary metastatic deposit.
Preferred examination
Plain chest radiographs are routinely obtained in patients who are suspected of having cancer and are also used in the staging of cancer, but plain abdominal radiography has a limited role in the investigation of liver metastases. Ultrasonography (US) is widely used in the investigation of suspected liver metastases.
Intraoperative US (IOUS) of the liver has the highest sensitivity for the detection of focal liver abnormalities, with 96% accuracy; by contrast, the accuracy of transabdominal US is 84%. Duplex and color-flow imaging provide additional aids in the localization of lesions; the differentiation between ducts and blood vessels; the documentation of vascular invasion, occlusion, or both; the assessment of the presence of collateral circulation; and the degree of vascularity of liver metastases.
Late-phase pulse-inversion harmonic imaging is a useful technique for characterizing hepatic lesions and for demonstrating both greater numbers of liver metastases and smaller liver metastases. Contrast-enhanced US in the liver-specific phase of contrast enhancement improves the detection of hepatic metastases, relative to nonenhanced conventional US.
MRI is usually reserved for problem solving because of the cost of the procedure. However, evidence supporting the use of MRI in the evaluation of liver metastases is accumulating because MRI allows the effective localization of hepatic and vascular invasion. However, CT remains the preferred option over both MRI and US. CT permits better evaluation of the involvement of extrahepatic tissues, including the bones, bowel, lymph nodes, and mesentery.
In their meta-analysis, Kinkel et al compared US, CT, MRI, and fluorodeoxyglucose (FDG) imaging in the detection of liver metastases from colorectal, gastric, and esophageal cancers and concluded that, with an equivalent specificity, FDG positron emission tomography (PET) is the most sensitive noninvasive imaging modality for the diagnosis of liver metastases. [6]
Selective hepatic angiography may demonstrate hypervascular liver metastases by showing capillary blush in involved areas, highlighting the potential response of tumors to embolization. Angiography is essential when hepatic vascular intervention is planned.
The liver provides a fertile soil in which metastases may become established, not only because of its rich, dual blood supply but also because of humoral factors that promote cell growth. (The blood supply of the liver is exceeded only by that of the lung, in terms of blood flow per minute.) The fenestrations in the sinusoidal endothelium allow a foothold into the space of Disse for tumor emboli arriving via the blood stream. [7, 8, 9]
Most liver metastases are multiple. In 77% of patients with liver metastases, both lobes are involved; in only 10% of cases is metastasis solitary. Multiple tumors often vary in size; this fact suggests that tumor seeding occurs in episodes. Growing metastases compress adjacent liver parenchyma, causing atrophy and forming a connective tissue rim. Large metastases often outgrow their blood supply, causing hypoxia and necrosis at the center of the lesion.
Approximately 50% of the patients with liver metastases have clinical signs of hepatomegaly or ascites; liver function tests tend to be insensitive and nonspecific.
Several factors influence the incidence and pattern of liver metastases. These include the patient's age and sex, the primary site, the histologic type, and the duration of the tumor. In a few tumor types, such as colonic carcinoma, carcinoid, and hepatocellular carcinoma (HCC), metastasis is confined to the liver. Most tumors that metastasize to the liver, such as breast and lung cancers, spread to other sites at the same time (see the images below).
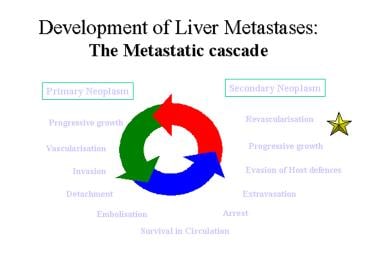 Liver, metastases. The metastatic cascade in the development of liver metastases.
Liver, metastases. The metastatic cascade in the development of liver metastases.
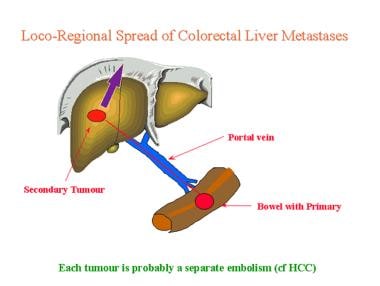 Liver, metastases. Diagram showing the mechanism of the local-regional spread of colorectal liver metastases.
Liver, metastases. Diagram showing the mechanism of the local-regional spread of colorectal liver metastases.
Some focal lesions may be surgically resectable or treated by means of ablation techniques. Imaging plays a vital role in the diagnosis of liver metastases and in the assessment of the response to treatment. The recognition of a liver lesion as a metastatic focus may significantly influence the patient's treatment and prognosis.
Limitations of techniques
One major drawback of all imaging examinations is that they seldom enable a tissue diagnosis. The differentiation of granulomatous lesions of the liver from primary benign or malignant liver lesions may be difficult. Diagnostic difficulties may be encountered in the characterization of atypical hemangiomas and focal nodular hyperplasia (FNH). Hemangiomas may coexist with metastases.
In endemic regions of the world, hydatid liver disease may be a great mimic of liver metastases. Hydatid cysts may be unilocular, multilocular, complex, and solid or calcified. Occasionally, defects present after liver cryosurgery may mimic liver metastases. Certain pseudolesions, such as focal fatty infiltration or focal fatty sparing, may also pose problems.
Radiography
Plain radiographs have only a minor role in the diagnosis of liver metastases, and most radiographic abnormalities are an incidental finding. The chest radiograph may show an elevated right hemidiaphragm as a result of hepatomegaly or ascites. A primary lung parenchymal tumor may be demonstrated. Metastases may be present in the lung and mediastinum (see the image below).
 Liver, metastases. Plain radiograph of the upper abdomen shows gross hepatomegaly and multiple conglomerates of punctate calcification in the right hypochondrium encroaching on the left hypochondrium. The final diagnosis was a medullary carcinoma of the thyroid (calcified) with calcified hepatic metastases.
Liver, metastases. Plain radiograph of the upper abdomen shows gross hepatomegaly and multiple conglomerates of punctate calcification in the right hypochondrium encroaching on the left hypochondrium. The final diagnosis was a medullary carcinoma of the thyroid (calcified) with calcified hepatic metastases.
A plain radiograph of the abdomen may confirm hepatomegaly and show changes suggestive of ascites. Calcified metastases have been reported from a variety of primary sites but particularly from a mucin-secreting colorectal cancer.
Calcification within metastases tends to be amorphous, unlike solid calcification in granuloma. The spleen may be enlarged with or without portal hypertension. Plain radiography may also demonstrate other nonspecific features, extrinsic impression of the left lobe of liver on a gastric gas shadow, ascites, and splenomegaly, among other findings. Calcification is a more specific sign, seen in 2-3% of lesions, but it is insensitive except in children with neuroblastoma, in whom the sensitivity approaches 25%. The pattern of calcification seldom indicates whether the tumor is primary or secondary. The pattern may be variable, and it may have a stippled, flaky, amorphous, nodular, or granular appearance.
Causes of calcified liver metastases include the following:
-
Ovarian serous lesion
-
Mucinous adenocarcinoma of the stomach, pancreas, colon, and rectum
-
Leiomyosarcoma (usually of the stomach)
-
Endocrine pancreatic carcinoma
-
Osteogenic sarcoma
-
Treated breast cancer
-
Pleural mesothelioma
-
Ovarian teratocarcinoma
Chest radiographs are routinely obtained in all patients with cancer, as well as in those suspected of having cancer. Lung cancer is a frequent cause of liver metastases, and metastases to the lung from other primary sites alter the management of cancer considerably. Chest radiography remains the primary imaging modality for the detection of lung cancer. A plain abdominal radiograph plays only a minor role in the investigation of liver metastases.
Chest radiography lacks specificity; a benign lung parenchymal lesion may have an appearance similar to that of cancer. Calcified liver lesions have been reported in association with a variety of conditions, including granulomatous disease, hydatid cysts, old healed liver abscesses, old liver infarcts, primary benign and malignant liver tumors, porcelain gallbladder, vascular calcification, and intrahepatic biliary calculi, to name a few.
Computed Tomography
CT is the examination of choice for evaluating liver metastases. This preference is largely attributable to the effects of the dual blood supply on the enhancement characteristics of metastases, as compared to normal liver parenchyma. Helical (spiral) CT techniques and multisection CT have revolutionized the use of CT in hepatic imaging. The accuracy of CT in the detection of metastases varies with the technique used, the underlying primary lesion, and the degree of vascularity (see the images below). [10, 11, 12, 13, 14, 15]
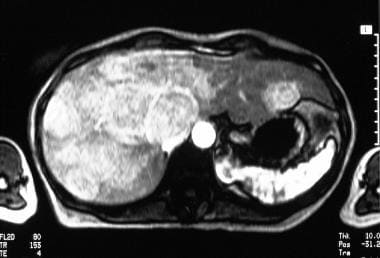
Liver, metastases. Characteristic appearance of carcinoid liver metastases on a contrast-enhanced axial CT scan through the upper abdomen. Portal venous phase image shows the metastases as negative defects against the normally enhancing liver
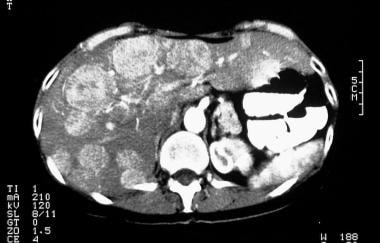 Liver, metastases. Characteristic appearance of carcinoid liver metastases on contrast-enhanced axial CT scan through the upper abdomen, which shows early arterial enhancement of the liver metastases.
Liver, metastases. Characteristic appearance of carcinoid liver metastases on contrast-enhanced axial CT scan through the upper abdomen, which shows early arterial enhancement of the liver metastases.
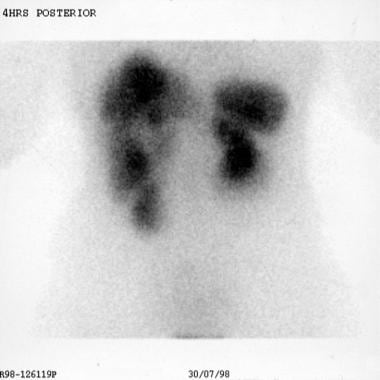
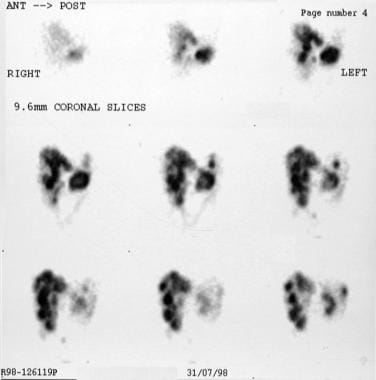 Liver, metastases. Characteristic appearance of carcinoid liver metastases on single-photon emission CT scans obtained with indium-111 octreotide. Images show liver lesions in detail.
Liver, metastases. Contrast-enhanced transaxial CT images in the portal venous phase through the liver of a 48-year-old man with colonic metastases. The left image shows metastases in both lobes of the liver and, thus, inoperable. The right image was taken 2 months after oxaliplatin therapy. The metastases were downstaged. The patient underwent a successful right hepatectomy.
Contrast-enhanced CT scans taken in the portal venous phase show a hypervascular metastatic deposit from a renal cell carcinoma. The patient had a previous right hepatectomy for an earlier renal cell solitary metastatic deposit.
Liver, metastases. Characteristic appearance of carcinoid liver metastases on single-photon emission CT scans obtained with indium-111 octreotide. Images show liver lesions in detail.
Liver, metastases. Contrast-enhanced transaxial CT images in the portal venous phase through the liver of a 48-year-old man with colonic metastases. The left image shows metastases in both lobes of the liver and, thus, inoperable. The right image was taken 2 months after oxaliplatin therapy. The metastases were downstaged. The patient underwent a successful right hepatectomy.
Contrast-enhanced CT scans taken in the portal venous phase show a hypervascular metastatic deposit from a renal cell carcinoma. The patient had a previous right hepatectomy for an earlier renal cell solitary metastatic deposit.
 CT scan in the same patient as in the previous image following immunotherapy. Note the considerable reduction in the size of the liver lesion.
CT scan in the same patient as in the previous image following immunotherapy. Note the considerable reduction in the size of the liver lesion.
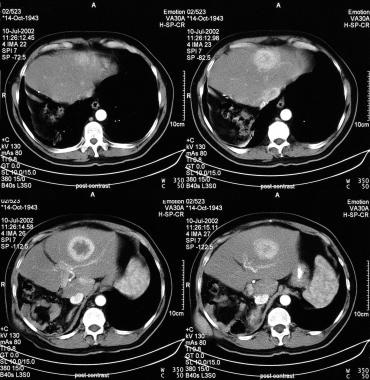
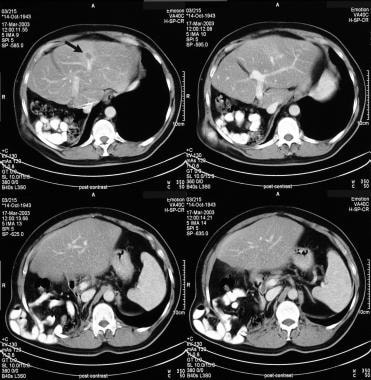
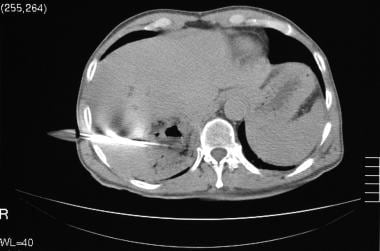
 Contrast-enhanced CT scan in a patient who had undergone a left hepatectomy for a hepatocellular carcinoma. The patient has developed a small metastatic deposit within the liver remnant (arrow in the upper 2 frames). The lower 2 frames were taken after alcohol ablation.
Contrast-enhanced CT scan in a patient who had undergone a left hepatectomy for a hepatocellular carcinoma. The patient has developed a small metastatic deposit within the liver remnant (arrow in the upper 2 frames). The lower 2 frames were taken after alcohol ablation.
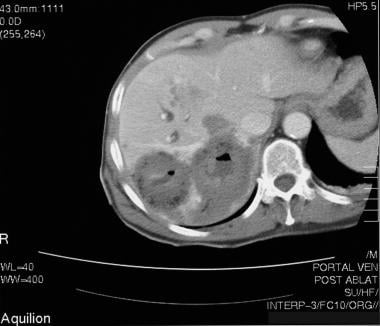
 Recurrent/metastatic hepatocellular carcinoma following chemoembolization. Note the intense iodized oil uptake, tumor necrosis, and air within the necrotic tumor. Also note the iodized oil uptake in the smaller, satellite tumors.
Recurrent/metastatic hepatocellular carcinoma following chemoembolization. Note the intense iodized oil uptake, tumor necrosis, and air within the necrotic tumor. Also note the iodized oil uptake in the smaller, satellite tumors.
 CT scan of a 52-year old man with a previous chemoembolization for hepatocellular carcinoma who had a recurrent tumor adjacent to the previously embolized tumor. This scan was taken following alcohol ablation.
CT scan of a 52-year old man with a previous chemoembolization for hepatocellular carcinoma who had a recurrent tumor adjacent to the previously embolized tumor. This scan was taken following alcohol ablation.

 CT scan in the same patient as in the previous image shows the placement of radiofrequency probes.
CT scan in the same patient as in the previous image shows the placement of radiofrequency probes.
 Contrast-enhanced CT scan in the same patient as in the previous 2 images with colorectal liver metastases.
Contrast-enhanced CT scan in the same patient as in the previous 2 images with colorectal liver metastases.
Metastases may appear in a multitude of ways on CT scans. The majority of liver metastases are hypovascular (hypoattenuating) in comparison to surrounding parenchyma; therefore, on nonenhanced CT scans, most lesions appear either hypoattenuating or isoattenuating relative to the surrounding parenchyma. Though nonenhanced scans are no longer routinely obtained in the evaluation of liver metastases, they are useful for the detection of calcified metastases, which often occur with mucinous primary tumors such as those of the colon, ovary, and breast. Nonenhanced images may also be helpful in the detection of hemorrhage. [16, 17, 18, 19, 20, 21, 22]
Both calcification and hemorrhage may become obscured on contrast-enhanced scans. Hypovascular lesions are routinely detected by use of contrast-enhanced techniques. The accuracy of the technique depends on the timing of the acquisition relative to the administration of contrast material. The optimal scanning time is in the portal venous phase (approximately 60 s). [23, 24, 25]
Conventional CT scanners have been superseded by helical scanners and multisection scanners that allow the rapid acquisition of images and the use of smart preparation, which triggers scanning at a predetermined Hounsfield unit value in a region of interest. [26, 27, 28, 29, 30, 31, 32]
During portal venous scanning, the attenuation of the normal liver parenchyma increases, revealing the relatively hypoattenuating metastases, sometimes with vague peripheral enhancement. The enhancement that occurs represents viable tumor peripherally, which appears against a necrotic center. The hypoattenuating center can be the result of cystic changes, such as those in primary tumors of the ovary and pancreas. Though the margins of the lesions may vary considerably from well defined to ill defined and infiltrating, the defining characteristic of a hypoattenuating center is the most common CT presentation.
Hyperattenuation of lesions, occurring as a result of increased tumor vascularity, is uncommon. On nonenhanced scans, some metastases of vascular primary tumors, such as renal cell carcinomas, pancreatic islet cell tumors, pheochromocytomas, melanomas, and breast carcinomas, may appear as hypoattenuating lesions.
When vascular metastases are suspected, a nonenhanced scan is recommended. On arterial phase (20-30 s) enhanced scans, these vascular metastases show homogeneous enhancement as compared to the surrounding liver; sometimes, a hypoattenuating rim is observed. Most of these lesions become isoattenuating to normal liver in the portal phase of dual-phase CT. Dual-phase CT requires fast scanning sequences, available only with helical and multisection scanners. Triple-phase CT is routinely performed in some centers; it involves multisection scanners and is particularly useful in evaluating suspected hyperattenuating metastases.
CT techniques
Delayed high-dose contrast-enhanced CT is rarely used; however, it is of value in the evaluation of equivocal lesions. This examination is performed 4-6 hours after the administration of contrast material. The iodinated contrast agent concentrates in the normal liver hepatocytes but not in focal lesions. Therefore, focal lesions appear as regions of low attenuation. The dual-phase CT scan obtained earlier serves as a roadmap for the normal vessels of the liver. [33, 34, 35]
The most sensitive technique for detecting liver metastases is CT arteriography (CTA) and CT arterioportography (CTAP). Although these are invasive procedures, they are invaluable in accurately assessing the number and position of the lesions before hepatic resection. In CTA, a percutaneous catheter is placed into the hepatic artery, and a CT scan is obtained through the liver. Though the technique demonstrates the most minimal of peripheral vascular enhancement in hypoattenuating lesions, CTA is most useful in evaluating hyperattenuating lesions because hepatic neoplasms receive most of their blood supply from the hepatic artery.
In CTAP, a catheter is placed percutaneously into the superior mesenteric or splenic artery so that CT can be performed during the portal venous phase of contrast enhancement. The normal liver is homogeneously enhancing, and the metastases appear as nonenhancing masses. Therefore, CTAP is the preferred technique for evaluating hypovascular metastases.
A further scanning technique that is rarely used in the evaluation of metastases is iodolipid CT. A hyperattenuating iodolipid such as lipiodol is injected directly into the hepatic artery, and CT scanning is performed through the liver in 5-7 days. The iodolipid is rapidly cleared from the normal parenchyma, but it is retained within neoplastic tissue; this feature aids in the detection of very small space-occupying lesions.
Dual-energy CT has been cited as a promising tool for assessment of colorectal cancer liver metastases. [36]
Degree of confidence
CT is the most sensitive technique for the detection of liver metastases. Contrast-enhanced scans offer a high degree of sensitivity—as high as 80-90%. The specificity is 99%. Helical and multisection techniques have eliminated respiration-related misregistration, allowing far better detection of smaller metastases. [6]
CTA and CTAP have similar sensitivities, though whether CTAP is more sensitive in detecting small subcentimeter metastatic lesions is arguable. CTAP is less specific than CTA.
Metastases may look like almost any lesion that occurs in the liver. Hemangiomas may be easily mistaken for metastases when they are multiple. On nonenhanced CT, they often form well-defined hypoattenuating lesions that mimic vascular metastases. On contrast-enhanced scans, they show peripheral enhancement. However, unlike vascular metastases, hemangiomas take at least several minutes to become completely filled. The area of central low attenuation typified by hypoattenuating metastases may simulate cysts in the liver. However, with the administration of contrast material, little doubt remains because cysts show no enhancement.
Focal nodular hyperplasia (FNH) rarely poses a major diagnostic problem, except in cases in which the lesions do not possess a prominent central scar; in these cases, they may look like vascular metastases. A fatty liver may obscure metastases on both nonenhanced and enhanced scans. Focal fatty sparing in a diffusely fatty liver or foci of focal fatty infiltration may simulate metastases. However, on nonenhanced scans, these regions of fat variation tend to be nonspherical and geographic, with no mass effect or distortion of the local vessels.
Small, 0.5-cm lesions may be missed on helical and multisection CT scans. With helical CT, partial-volume artifact may compound this problem if the pitch is greater than 1.5. The rate of contrast administration and the timing of the acquisition must be precise to avoid false-negative results. It is essential that a dynamic bolus technique be used. On delayed scans, hepatic vessels appear hypoattenuating, as do focal lesions; therefore, the vessels may be confused with small lesions. As long as a dynamic bolus examination has been performed earlier to identify vessels, this confusion should be limited.
Problems may arise with the invasive techniques of CTA and CTAP. CTA highlights subtle differences in the perfusion of the liver resulting from, for example, variations in hepatic arterial anatomy. The detection of small metastases may be difficult, and portal branches may mimic masses. Perfusion abnormalities may interfere with CTAP (eg, in the presence of portal hypertension or lobar hyperperfusion secondary to accessory or replaced hepatic arteries). The specificity of CTAP is not as good as that of CTA, because virtually all lesions appear hypoattenuating. Anomalous peripheral venous drainage, local variations in portal perfusion, and mixing from nonenhancing splenic venous blood may enable the detection of pseudolesions and may be useful for recognizing false-negative results.
In a study by Nakai et al of imaging characteristics of liver metastases overlooked on contrast-enhanced CT, liver metastases without sufficient contrast enhancement, those in patients with hepatic steatosis, those in subcapsular locations, and those found at examinations for indications other than assessment for tumors were significantly more likely to be overlooked. [37]
Magnetic Resonance Imaging
MRI is seldom used as a primary tool in the diagnosis of liver metastases, but it is regarded as a problem-solving technique. It is also used when alternative imaging is contraindicated. MRI has the advantages of providing high inherent contrast resolution, providing biochemical and morphologic information, offering a multiplanar capability, and possessing an intrinsic sensitivity to blood flow and blood breakdown products.
As with CT and US, liver metastases have a variety of appearances on MRI. Most liver tumors, whether benign or malignant, appear as hypointense lesions on T1-weighted images and as hyperintense lesions on T2-weighted images. There are a few exceptions to this rule (eg, metastatic melanoma, which exhibits high signal intensity on T1-weighted MRIs relative to the liver) (see the images below). [38, 39, 40, 41, 42, 43, 44, 45]
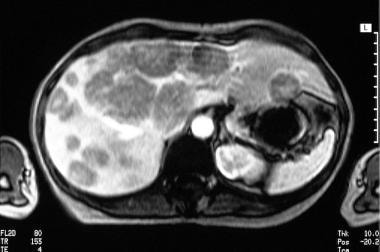 Liver, metastases. Characteristic appearance of carcinoid liver metastases on a gadolinium-enhanced axial MRI through the liver. Image shows early arterial enhancement of multiple liver tumors.
Liver, metastases. Characteristic appearance of carcinoid liver metastases on a gadolinium-enhanced axial MRI through the liver. Image shows early arterial enhancement of multiple liver tumors.
 Liver, metastases. Characteristic appearance of carcinoid liver metastases on a gadolinium-enhanced axial MRI through the liver. Image shows portal venous phase enhancement of multiple liver tumors.
Contrast-enhanced CT scan in a patient who had undergone a left hepatectomy for a hepatocellular carcinoma. The patient has developed a small metastatic deposit within the liver remnant (arrow in the upper 2 frames). The lower 2 frames were taken after alcohol ablation.
Liver, metastases. Characteristic appearance of carcinoid liver metastases on a gadolinium-enhanced axial MRI through the liver. Image shows portal venous phase enhancement of multiple liver tumors.
Contrast-enhanced CT scan in a patient who had undergone a left hepatectomy for a hepatocellular carcinoma. The patient has developed a small metastatic deposit within the liver remnant (arrow in the upper 2 frames). The lower 2 frames were taken after alcohol ablation.
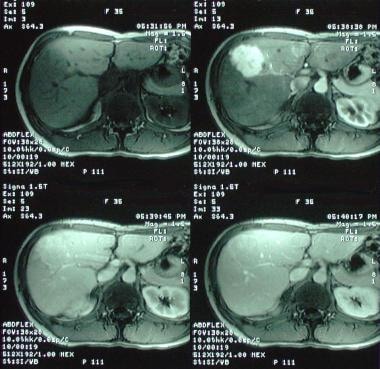 Liver metastases. Mimics. Dynamic MRIs in a 36-year-old woman referred for a gallbladder ultrasonography. The patient was found to have a vague, ill-defined, hypoechoic mass within the right lobe of the liver. Gadolinium-enhanced T1-weighted MRI (top left) demonstrates an ill-defined hypointense mass, which is intensely enhancing in the arterial phase after the administration of contrast (top right). Minor enhancement persists in the portal venous phase (bottom left). On delayed images, the lesion becomes isointense relative to the liver (bottom right). The appearances are characteristic of focal nodular hyperplasia.
Liver metastases. Mimics. Dynamic MRIs in a 36-year-old woman referred for a gallbladder ultrasonography. The patient was found to have a vague, ill-defined, hypoechoic mass within the right lobe of the liver. Gadolinium-enhanced T1-weighted MRI (top left) demonstrates an ill-defined hypointense mass, which is intensely enhancing in the arterial phase after the administration of contrast (top right). Minor enhancement persists in the portal venous phase (bottom left). On delayed images, the lesion becomes isointense relative to the liver (bottom right). The appearances are characteristic of focal nodular hyperplasia.
Heavily T2-weighted images are useful in differentiating hemangiomas and cysts because the signal intensity is higher in these benign lesions than in liver metastases. However, differentiating benign lesions from malignant lesions on the basis of signal intensity characteristics on heavily T2-weighted images may not be conclusive; combining the signal intensity changes with the morphologic changes in the lesion is more useful.
Morphologic characteristics on T2-weighted images that suggest metastatic liver disease include the following: (1) heterogeneous signal intensity with irregular and indistinct outer margins and (2) a smooth or irregular central area of high signal intensity with a surrounding ring of signal intensity lower than that of the central focus but higher than that of the adjacent normal liver. Intravenous contrast agents improve the detection of liver mass lesions.
MRI contrast agents and contrast-enhanced techniques
The contrast agents available for use in liver imaging may be classified into 4 groups according to their biologic distribution:
-
Gadolinium chelates, which have an extracellular distribution
-
Macrophage-monocytic agents targeted to the phagocytic system
-
Hepatobiliary agents
-
Blood pool agents
This classification is not strictly accurate because these agents are distributed successively or simultaneously to more than one site.
Use of dynamic gadolinium-enhanced MRI not only improves the detection of focal liver masses but also permits the differentiation of benign lesions and malignant lesions. In some instances, contrast-enhanced imaging may enable the specific diagnosis of a focal liver lesion. Metastases enhance heterogeneously and occasionally show central nonenhancing areas as a result of tumor necrosis. Hypervascular metastases enhance more than the surrounding liver in the arterial phase of a dynamic study, whereas hypovascular metastases enhance less than the surrounding liver.
Studies have shown that target tumor enhancement of colorectal cancer liver metastases on 10-minute delayed-phase gadolinium-enhanced MRI is associated with overall survival after hepatectomy. A recent study has shown that the same may be true for 5-minute post-contrast injection with gadolinium (36-month survival with strongly enhancing tumors was 74.4%, as compared to 44.6% with weakly enhancing tumors). [46, 47, 48, 49, 50, 51, 52]
Extracellular contrast agents, such as gadolinium-based agents, have a narrow time window during which the liver may be imaged. This limitation may be overcome by the use of contrast agents targeted to the liver.
An octadenatate gadolinium chelate, gadolinium benzylopropionictetraacetate (Gd-BOPTA), has been developed as an extracellular hepatobiliary contrast agent for use with MRI. This agent produces more selective and more prolonged liver enhancement. Gd-BOPTA may therefore overcome the timing restrictions encountered with gadolinium diethylenetriamine pentaacetic acid (Gd-DTPA).
Compared with Gd-DTPA, mangafodipir trisodium (Mn-DPDP) provides a fivefold increase in the signal-to-noise ratio and also prolonged enhancement of normal liver, whereas liver metastases show no significant enhancement. After the intravenous injection of Mn-DPDP, maximal liver enhancement is sustained for approximately 30 minutes. Therefore, Mn-DPDP may overcome the restrictive imaging window encountered with Gd-DTPA.
In a meta-analysis of 10 articles (256 patients, 562 metastases) by Zhang et al to determine the sensitivity and positive predictive value (PPV) of gadobenate-enhanced MR imaging for detection of liver metastases, overall sensitivity was 95.1% and PPV was 90.9%. Individual sensitivity estimates for precontrast (unenhanced) imaging, gadobenate-enhanced dynamic imaging, and combined unenhanced, dynamic, and delayed hepatobiliary phase imaging were 77.8%, 88.1%, and 95.1%, respectively. Addition of hepatobiliary phase images was found to significantly improve detection of liver metastases. [53]
In a meta-analysis of diffusion-weighted MRI versus gadoxetic acid-enhanced MRI, sensitivity estimates for DW-MRI alone, gadoxetic acid-enhanced MRI alone, and the combined sequence for detecting liver metastases were 87.1%, 90.6% and 95.5%, respectively. [54]
Iron oxides are cleared by the reticuloendothelial system. Two types of iron oxides are available: superparamagnetic iron oxide particles (SPIOs) and ultrasmall superparamagnetic iron oxide particles (USPIOs). Iron oxides decrease the signal intensity of the normal liver by shortening T2 as a result of magnetic susceptibility. Delayed-enhanced images obtained 60 minutes after the injection outline the phagocytic activity of the liver. However, because metastases do not usually contain Kupffer cells, they do not take up iron oxide particles. Thus, liver metastases stand out against a dark background.
Sensitivity and specificity of MRI
Technically, MRI is as sensitive as CT in the detection of liver metastases. The use of ultrafast techniques has certainly increased the sensitivity of MRI, although it is still inferior to CTAP. In a number of settings, MRI is superior to other imaging techniques. Hemangiomas are reliably diagnosed with MRI, and more importantly, they are more easily differentiated from metastases with MRI than with other imaging modalities.
MRI is said to be the best modality in the diagnosis of focal nodular hyperplasia (FNH); it has a sensitivity of 70% and a specificity of 98%. The central scar is more often detected by MRI than by CT. One limiting factor of gadolinium-enhanced MRIs of the liver is that the liver must be imaged repetitively with T1-weighted gradient-echo sequences during hepatic arterial, portal venous, and delayed phase of contrast enhancement.
Gadolinium-enhanced study is always performed in the phase that shows the greatest differences in the distribution of contrast agent between normal tissues and abnormal tissues. For all practical purposes, this means such studies are performed during the portal venous phase. Therefore, a time limit exists during which imaging may be performed with gadolinium-based and other extracellular contrast agents. The time-limiting factor may be overcome through the use of tissue-specific contrast agents.
The use of Mn-DPDP avoids the problems of restrictions in timing that arise with the use of Gd-DTPA; in addition, with the use of Mn-DPDP, nonenhancing hepatocellular lesions (eg, metastases) can be distinguished from benign and malignant hepatocellular lesions. Mn-DPDP imaging has a sensitivity of 100%, a specificity of 92%, and an accuracy of 93.6%.
SPIO and USPIO images depict more liver focal lesions than do nonenhanced MRIs obtained at all field strengths. With SPIO techniques, lesions as small as 3 mm can be detected; by contrast, with conventional techniques, the smallest lesions that can be detected are 10 mm. Compared with conventional techniques, SPIO enhancement appears to be more sensitive than contrast-enhanced CT.
MRI was found to be significantly superior to 18F-FDG PET/CT in the detection and classification of liver metastases in patients with adenocarcinomas of the GI tract, especially regarding detection of small metastases. [55]
Limiting factors with MRI
Two major factors limit the widespread use of MRI in liver imaging: technical factors and cost. The technical factors include motion artifacts, including respiratory, cardiac, and bowel movements, as well as aortic pulsation, which tend to degrade the images. These problems are not insurmountable and may be overcome with the use of ultrafast imaging, phased-array surface coils, and intraluminal and organ-specific contrast agents. Regarding the cost factor, with escalating health care expenses, cost-effectiveness and the use of a single imaging modality capable of answering the clinical question are being emphasized.
Gadolinium-based contrast agents have been linked to the development of nephrogenic systemic fibrosis (NSF) or nephrogenic fibrosing dermopathy (NFD). NSF/NFD has occurred in patients with moderate to end-stage renal disease after being given a gadolinium-based contrast agent to enhance MRI or MRA scans. NSF/NFD is a debilitating and sometimes fatal disease. Characteristics include red or dark patches on the skin; burning, itching, swelling, hardening, and tightening of the skin; yellow spots on the whites of the eyes; joint stiffness with trouble moving or straightening the arms, hands, legs, or feet; pain deep in the hip bones or ribs; and muscle weakness.
Diseases that may be confused with liver metastases include the following: hemangioma, FNH, HCC, hepatocellular adenoma, liver cyst, biliary hamartoma, biliary cystadenoma, intrahepatic cholangiocarcinoma, angiosarcoma, epithelioid hemangioendothelioma, primary hepatic lymphoma, focal fatty infiltration and focal fatty sparing, lipoma, and inflammatory pseudotumor. These diseases are described below.
In addition, Mn-DPDP enhancement has been reported in HCC, regenerative nodules, and foci of FNH. The appearances on SPIO and USPIO images are nonspecific, and metastases, primary benign tumors, malignant tumors, and cysts may have similar appearances.
Hemangioma
Hemangiomas and liver metastases are often confused. Hemangiomas show low signal intensity on T1-weighted images and high signal intensity on T2-weighted images. Heavily T2-weighted images are useful in differentiating hemangiomas from other solid tumors because the signal intensity is higher in hemangiomas.
Breath-hold and fast spin-echo techniques are particularly useful for distinguishing hemangiomas from metastases. Hemangiomas may also be characterized by their typical enhancement pattern after the administration of a gadolinium chelate. Typically, discrete, nodular peripheral enhancement is observed. In distinction, metastases often show transient rim enhancement. A peripheral rim of hypointensity relative to the center of the tumor on delayed-contrast images is said to be a specific sign of malignancy.
Focal nodular hyperplasia
FNH often contains a central scar. Because hepatocytes are the major components of FNH, its signal intensity on MRI parallels that of the normal liver. Small areas may be difficult to detect on MRIs. FNH usually has homogeneous signal intensity except for the central scar. FNH is slightly hypointense to the liver on T1-weighted images and slightly hyperintense on T2-weighted images. The central scar appears hypointense on T1-weighted images and hyperintense on T2-weighted images. Flow-sensitive MRI may demonstrate arteries in the central scar if the arteries are large enough. These features of FNH on nonenhanced images are not encountered in all cases; hence, contrast-enhanced MRI studies may be required for a confident diagnosis.
Hepatocellular carcinoma
Hepatocellular carcinoma may be solitary or multicentric, and it may mimic liver metastases. HCC has low, intermediate, or high intensity on T1-weighted images. High signal intensity may be related to the fat content, intracellular glycogen, hemorrhage, or copper deposition. The finding of high intensity on T1-weighted images is useful because few other liver lesions have high signal intensity on these images; these lesions include fat-containing benign tumors and hemorrhagic tumors, such as hepatic adenomas.
HCC is hyperintense on T2-weighted images; larger tumors may show a mosaic pattern. A tumor capsule, if seen, may have low signal intensity on T1-weighted images and a double-layered appearance on T2-weighted images. The outer layer is hyperintense, and the inner layer is hypointense. Associated venous thrombosis that is well depicted on MRIs suggests HCC. Regenerative nodules in a cirrhotic liver classically have low signal intensity on T1-weighted images because of the accumulation of iron.
Hepatocellular adenoma
Hepatocellular adenomas are usually solitary; most affect young females taking oral contraceptives. However, in rare cases, the tumors may be multiple and mimic metastases. On MRI, the tumor appears hyperintense or isointense on T1-weighted images and mildly hyperintense on T2-weighted images. These tumors often have a fatty component (50%), which may be assessed by means of fat-suppressed or inversion recovery sequences. The appearance of hemorrhage within the liver, which is common, depends on the age of the hematoma. Signal heterogeneity within these tumors is common because of the wide range of pathologic changes that may occur in hepatic adenomas.
Patterns of gadolinium enhancement are variable. Unlike FNH lesions, which are usually hypervascular, adenomas may appear as avascular lesions. However, most hepatocellular adenomas are hypervascular in the arterial phase of a dynamic contrast dynamic study. In about a third of the cases, a peripheral rim is observed; this is hypointense on T1-weighted images and of variable intensity on T2-weighted sequences. This rim shows gadolinium enhancement, which represents compressed normal liver around the tumor. Some MRI features are shared by both hepatocellular adenomas and HCCs; therefore, a tissue diagnosis may be required.
Liver cyst
Complex and complicated liver cysts may be confused with metastases. MRI is particularly good for depicting hemorrhagic hepatic cysts. Intracystic hemorrhage remains hyperintense on T2-weighted images, but with T1-weighted images, the signal intensity is homogeneously high or heterogeneous. A hyperintense fluid-fluid level may be observed in the dependent part of the cyst, and low or intermediate signal intensity may be present in the upper part of the cyst. Infected cysts enhance with the use of a gadolinium-based contrast agent. Multiloculated or coalescent cysts may also mimic cystic tumors with intramural nodules. The walls and septa do not enhance. MRI is not usually indicated in the workup of cysts detected with US or CT. MRI is useful in differentiating complicated cysts from metastases.
Biliary hamartoma
Biliary hamartomas (Meyenberg complexes) are benign lesions that consist of a focal collection of bile ducts. They are usually multiple and are located predominantly in the subcapsular region. US and CT findings are nonspecific and may mimic those of metastases. The lesions have low signal intensity on T1-weighted MRIs and homogeneously high signal intensity on T2-weighted MRIs. The homogeneous hyperintensity on T2-weighted images is crucial and indicates benign lesions.
Biliary cystadenoma
Biliary cystadenoma and cystadenocarcinoma may mimic cystic liver metastases. These tumors are similar to mucinous cystic tumors of the pancreas and ovary. Most tumors contain closely bound spindle cells below the epithelium that resemble ovarian stroma found only in women. A small number of tumors do not contain ovarian stroma; these may be found in men and women. Grossly, the tumors are multiloculated with varying degrees of septation and nodularity. The locules contain fluid of variable consistency; this fluid may be serous, mucinous, bilious, hemorrhagic, or a combination of these. Radiologically, features such as septa and nodularity are associated with cystadenocarcinoma when they are seen together. MRI depicts the multilocular mass with septa and nodularity; the signal intensity varies with the consistency of the intralocular fluid.
Intrahepatic cholangiocarcinoma
Intrahepatic cholangiocarcinomas account for 10% of all primary malignant liver tumors. MRI depicts a nonencapsulated tumor that is hypointense on T1-weighted images and hyperintense on T2-weighted images. A central hypointensity corresponding to a central scar may be seen on T2-weighted images. The depiction of a central scar on MRIs is a reliable feature for differentiating a metastatic tumor from a primary liver tumor.
Gadolinium enhancement patterns depend on the size of the tumor. Small tumors may be homogeneously enhancing, mimicking HCC. Larger tumors show minimal to moderate peripheral enhancement with progressive central filling. Incomplete central filling is noted on delayed images. The central scar may enhance, but it becomes isointense on delayed images, unlike FNH, which becomes hyperintense. There is controversy regarding portal and hepatic vein invasion. Some authors believe that vascular involvement is more a feature of HCC and that such involvement is exceptional with intrahepatic cholangiocarcinoma. However, most authors now believe that vascular infiltration is common with intrahepatic cholangiocarcinoma. Gradient-echo MRI is valuable in depicting vascular invasion.
Angiosarcoma
Angiosarcoma is a rare aggressive tumor of the liver that has been linked to industrial and environmental exposure to toxins. The MRI features are similar to those described in hemangiomas. Because both tumors contain abundant vascular spaces, they are usually hyperintense on T2-weighted images. However, angiosarcomas usually exhibit heterogeneous signal intensity with T2-weighted sequences. Peripheral gadolinium enhancement is often seen, but the enhancement is not as intense or globular as that in hemangiomas; it is usually discontinuous.
Epithelioid hemangioendothelioma
Epithelioid hemangioendothelioma is a rare, vascular, primary tumor of the liver that may mimic metastases on imaging. The tumor predominantly affects women in their 40s. MRI features have been described in only one case. T2-weighted images depict subcapsular nodules with increased signal intensity, similar to most liver malignancies, but the signal intensity is not as intense as that of a hemangioma. The tumor shows faint peripheral enhancement with a gadolinium-based contrast agent. MRI features of malignant mesenchymal tumors (plasmacytoma, leiomyosarcoma, undifferentiated sarcoma, epithelioid hemangioendothelioma, and angiosarcoma) may be difficult to differentiate from those of other benign or malignant liver tumors.
Primary hepatic lymphoma
Primary hepatic lymphoma is a rare disease. Hepatic lymphoma deposits are usually seen in association with systemic disease. On T1-weighted images, primary hepatic lymphoma is usually well defined and isointense to homogeneously hypointense or slightly hyperintense. On T2-weighted images, they are slightly heterogeneous and hyperintense. Lobulation is better seen with T2-weighted sequences. In one case, the margins were ill defined, and portal vein branches were identified within the tumor—an unusual finding in liver neoplasms. One lesion was studied after the injection of gadopentetate dimeglumine; it showed marked and heterogeneous enhancement.
Focal fatty infiltration and focal fatty sparing
Both focal fatty infiltration and focal fatty sparing may mimic malignant disease of the liver on images. The geographic configuration and typical periligamentous and periportal location should suggest the diagnosis. These lesions do not appear as a mass, and they have no mass effect. Blood vessels that traverse these lesions appear undistorted. Chemical shift imaging may be used to determine whether a suspicious area or the surrounding liver parenchyma contains microscopic fat. On T2-weighted MRIs, particularly fat-suppressed images, the lesion has the signal intensity of normal liver and not the spleen.
Lipoma
Fatty liver tumors are rare. Lipomas are well-defined tumors that are hyperintense on T1-weighted images. The signal intensity is usually similar to that of subcutaneous and retroperitoneal fat. On fat-suppressed images, the tumor appears hypointense; it may be differentiated from other hyperintense lesions on T1-weighted images. These lesions may be caused by copper deposition, hemorrhage, or peliosis, for example. Hepatic angiomyolipomas are usually hyperintense and heterogeneous on T1-weighted images. The hyperintensity is usually related to the fat content of the tumor and is usually suppressed with fat-suppression sequences. The hypervascularity and the aneurysmal component of the tumor may also cause hyperintensity on T1-weighted MRIs.
On T2-weighted images, the lesion again appears hyperintense and heterogeneous. The atypical angiomyolipoma is more likely to be confused with other liver tumors because they are hypointense on T1-weighted images and hyperintense on T2-weighted images. Rarely, angiomyolipomas do contain fat. These tumors are difficult to differentiate from other tumors on the basis of the imaging results. After the administration of a gadolinium-based contrast agent, these tumors enhance heterogeneously.
Inflammatory pseudotumor
Inflammatory pseudotumor of the liver is a rare disorder that usually affects infants and young men. The process is an inflammatory response to an unknown agent. The majority of patients present with signs and laboratory evidence of an active inflammatory process. Most of these lesions are located in segment 4. [56]
Only a few case reports describe the MRI features of hepatic pseudoinflammatory tumors. These lesions are usually solitary. They may have nonspecific increased signal intensity on T1- and T2-weighted images. Some reports describe a hypointense lesion on T1-weighted images and isointensity with a hyperintense ring on T2-weighted images. One case report describes irregular and intensely enhancing lesions on immediate postgadolinium spoiled gradient-echo images. Rapid washout was noted. Periportal involvement was also shown on T2-weighted fat-suppressed images. On the whole, the diagnosis may be difficult by use of imaging, and biopsy may be required.
Ultrasonography
Generally, metastases cause hepatomegaly, though this may not be evident until the disease is advanced. Intrahepatic masses may alter the shape of the liver, and its surface may appear nodular or lobular. This latter sign is nonspecific and also occurs in cystic fibrosis and liver infiltration. In general, the US appearance of liver metastases is nonspecific, and biopsy may be required for a tissue diagnosis. However, the presence of multiple hepatic nodules of different sizes within the liver is nearly always the result of metastases. Percutaneous biopsy should not be undertaken if curative hepatic resection may be possible. (See the images below.) [57, 58, 59]
 Liver, metastases. Characteristic appearance of carcinoid liver metastases with different imaging modalities. Axial sonogram through the liver shows multiple fairly well-defined echogenic liver metastases of varying sizes.
Liver, metastases. Characteristic appearance of carcinoid liver metastases with different imaging modalities. Axial sonogram through the liver shows multiple fairly well-defined echogenic liver metastases of varying sizes.
 Liver metastases. Mimics. A 2.5-cm echogenic nodule in the left lobe of the liver was confirmed to be a hemangioma on further imaging.
Liver metastases. Mimics. A 2.5-cm echogenic nodule in the left lobe of the liver was confirmed to be a hemangioma on further imaging.
Liver metastases may cause focal or diffuse parenchymal changes. [60] The US appearance and the histologic findings are poorly correlated, though cauliflower masses are often from the colon, and evaluation of the abdomen may reveal a bowel mass. The echogenicity is dependent on tumor vascularity; the cellular composition; the degree of tissue invasion; and the presence or absence of necrosis, fibrosis, and fatty change. Metastases complicated by hemorrhage, necrosis, or infection may result in bizarre changes in their configuration and echo pattern.
Isoechoic metastases
Isoechoic and infiltrating metastases are ill defined and difficult to identify. They occasionally have a mass effect, which is shown as a contour anomaly and a surface irregularity of the liver, as displacement or compression of the intrahepatic vasculature, or as segmental bile duct obstruction. Other signs of malignancy may be apparent; such signs include lymphadenopathy, ascites, and peritoneal metastases. Also, the primary site may be recognized; for example, a mass may be found in the pancreas.
Rarely, a sonolucent ring sign is seen. A mass in the liver adjacent to the gallbladder may demonstrate a hump sign (ie, edge sign) or a gallbladder compression sign. A hump, or edge, sign may indicate the presence of a superficial mass near the surface. These findings are nonspecific signs of space-occupying lesions in the liver; they may be caused by benign or malignant lesions. The gallbladder compression sign has also been described as a normal variant, although this condition is exceptionally rare.
Echogenic metastases
Metastases containing multiple tortuous vessels tend to be hypervascular; their echogenicity is most probably related to the number of blood-tissue interfaces rather than the blood vessel walls themselves. Metastases from the following tumors tend to be echogenic: GI cancer, renal cell carcinoma, carcinoid, choriocarcinoma, pancreatic islet cell tumors, chloromas (leukemic), and AIDS-related Kaposi sarcoma. In children, metastases from neuroblastoma, hepatoblastoma, leukemia, hepatoma, and Wilms tumor may be densely echogenic. Tumors responding to therapy may show increased echogenicity, but more often, they show a reduction in size.
Causes of echogenic metastases include the following:
-
Mucinous adenocarcinoma of the colon
-
Pancreatic carcinoma (usually hypoechoic but possibly becoming echogenic as calcification occurs)
-
Gastric carcinoma (usually hypoechoic)
-
Hepatocellular carcinoma (HCC)
-
Neuroblastoma
-
Cholangiocarcinoma
-
Treated breast carcinoma
-
Renal cell carcinoma
-
Carcinoid
-
Choriocarcinoma
-
Pancreatic islet cell tumors
-
Wilms tumor (usual spread is to lung)
-
Kaposi sarcoma
-
Myeloma deposit
-
Hepatic chloroma
Hypoechoic metastases
Hypoechoic metastases are generally hypovascular; they comprise uniform tissue, cellularity, or both. Any primary tumor can cause this pattern of metastases, but those particularly likely to have this pattern are lymphomas; melanomas; and carcinomas of the pancreas, lung, or cervix.
Causes of hypoechoic metastases include the following:
-
Lymphoma (especially AIDS related)
-
HCC
-
Pancreatic carcinoma
-
Lung (particularly adenocarcinoma)
-
Cervical carcinoma
-
Melanoma
-
Nasopharyngeal carcinoma
-
Kaposi sarcoma (rare; most are hyperechoic)
-
Myeloma deposits
-
Cystic liver metastases
-
Mucinous cystadenocarcinoma colon
-
Cystadenocarcinoma ovary
-
Cystadenocarcinoma pancreas
-
Leiomyosarcoma
-
Squamous cell carcinoma
-
Testicular carcinoma
-
Carcinoid
-
Granulosa cell ovarian tumor
Cystic metastases
Metastases that are cystic may mimic abscesses, hemorrhagic infarcts, hematomas, simple cysts, and hydatid cysts. Cystic metastases display a degree of complexity in the form of mural nodules, thickened walls and septa, and fluid/debris levels. These features are not present in simple hepatic cysts. A detailed clinical history may help exclude hematomas, hydatid cysts, and abscesses from consideration.
Two groups of patients tend to get cystic metastases: (1) those who have a primary neoplasm with a cystic component, such as a mucinous cystadenocarcinoma of the colon, stomach, pancreas, or ovary, and (2) those with metastases that are undergoing central necrosis. In cases of the latter, low-level echoes and wall irregularity are seen. Squamous cell carcinoma, leiomyosarcoma, melanoma, and testicular carcinoma have a propensity to undergo extensive central necrosis.
Bull's eye, or target, metastases
In bull's eye, or target, metastases, the halo is most probably related to a combination of compressed normal hepatic parenchyma around the mass and a zone of cancer cell proliferation. The presence of a halo usually suggests aggressive behavior. Bronchogenic carcinoma characteristically causes target-type metastases. However, this pattern is nonspecific and may be found with metastases from the breast and colon, as well as primary malignant liver neoplasms (eg, HCC) and benign liver neoplasms (eg, adenoma in glycogen storage disease). A similar appearance has been described with liver abscesses.
Calcified metastases
If calcified metastases are densely echogenic, they may shadow. The calcification and echogenicity result from intratumoral mucin, necrosis, or phosphatase activity. This pattern of metastases may occur from many primary sites, but it is particularly common with carcinoma of the colon of the mucin secreting type, pseudomucinous cystadenocarcinoma of the stomach, and (rarely) adenocarcinoma of the breast or melanoma. In children, neuroblastoma is the most common metastasis; it is usually hypoechoic; however, it may show calcification, and it may be echogenic.
Diffuse or infiltrative metastases
Diffuse disease may be the result of the confluence of areas of focal disease, infiltrating tumors, or miliary metastatic deposits. Diffuse disease is seen less frequently than focal disease. The liver may appear moth eaten or diffusely heterogeneous; in rare cases, the infiltrates are isoechoic.
Diffuse metastases may be difficult to detect with US, particularly on the background of fatty infiltration, which may occur as result of cirrhosis or chemotherapy. Lymphoma and leukemia are particularly prone to diffuse disease, which may appear hypoechoic, though these changes do not always reflect the presence of metastases. Reactive lymphocytic infiltration secondary to disease elsewhere may give rise to the same appearance. A diffuse pattern is commonly seen with carcinoma of the breast, lung, or melanoma.
When the liver is extensively replaced by metastases, jaundice may occur because of inadequate liver function; this sign may be result from the lack of normal liver tissue or from distortion of the hepatic architecture, particularly the bile ducts and vessels. Alternatively, Hodgkin disease may cause intrahepatic biliary obstruction at the canalicular level, and lymphadenopathy may compress the extrahepatic biliary system. Even in the absence of jaundice, liver function tests show some abnormality in the presence of diffuse intrahepatic malignancy.
Leukemia
Hepatomegaly is common in both lymphatic leukemia and myeloid leukemia. Chloromas are composed of granulocyte precursor cells. These are rare solid extramedullary tumors that usually have a mass effect. They may occur in intracranial, intrathoracic, and intra-abdominal sites. Most chloromas are seen in children. Chloromas within the liver are extremely rare. They may appear as hypoechoic or hyperechoic masses. The hyperechoic mass may mimic hemangiomas. Chloromas may rarely show central necrosis, which appears as echogenic centers mimicking Candida abscesses.
Lymphoma
Diffuse infiltration of liver and spleen is common in lymphoma; focal involvement is less common. The diffusely infiltrating type of liver lymphoma is difficult to image with US, because it may cause subtle architectural distortion or no US abnormality at all.
Primary lymphoma of the liver is an unusual entity, but its incidence appears to be rising. This change may reflect its appearance in the increasing numbers of immunocompromised patients, such as patients with AIDS or those undergoing organ transplantation. Primary lymphoma (confined to solitary organs) is more common with non-Hodgkin lymphoma than with other diseases. Focal hepatic lymphoma is usually hypoechoic; however, target and hyperechoic patterns have been described in cases of non-Hodgkin lymphoma but not in cases of Hodgkin lymphoma. Burkitt lymphoma may also cause hypoechoic liver masses. These masses are usually large at the time of diagnosis.
AIDS-related liver tumors
Non-Hodgkin lymphoma and Kaposi sarcoma are common complications of HIV infection. The incidence of Kaposi sarcoma in AIDS patients is 0.5-0.9% among those 1-19 years of age; the incidence increases with age, and the rate is higher in males than in females. In black children and in male adolescents who report having homosexual intercourse, the incidence of Kaposi sarcoma is 3 times higher. In children, non-Hodgkin lymphoma is more common than Kaposi sarcoma.
Primary non-Hodgkin lymphoma and Kaposi sarcoma affecting the liver are uncommon. However, in autopsy series in patients with Kaposi sarcoma and AIDS, 34% have liver involvement, but the incidence during imaging is lower.
Non-Hodgkin lymphoma usually appears with multiple hypoechoic masses in the liver; it is not different from that of a primary hepatic lymphoma in patients without AIDS. However, liver abnormalities are common in patients with AIDS and may be related to the following: (1) coincidentally acquired hepatotropic viruses, (2) complications of therapy, (3) changes associated with a chronic debilitating disease, or (4) complications related to immune compromise (eg, infections, neoplasms, iatrogenic complications).
In the liver, Kaposi sarcoma manifests itself as 5- to 12-mm hyperechoic nodules, although hypoechoic masses have also been reported. Three quarters of patients with AIDS-related Kaposi sarcoma have abdominal lymphadenopathy, which cannot be differentiated from non-Hodgkin lymphoma, inflammation, or infection on imaging. Biopsy is usually required to distinguish these entities.
Hepatic myeloma
Extramedullary myeloma deposits are extremely rare; a few cases of liver involvement have been reported. US shows hepatomegaly with single or multiple hypoechoic solid masses, but target lesions and hyperechoic masses have also been reported. A fine-needle aspirate may demonstrate numerous mononuclear cells, which are characteristic of myeloma.
Doppler techniques
Some researchers have attempted to use color and duplex Doppler arterial flow patterns around liver masses to improve the specificity of US examination. Unfortunately, Doppler results cannot always be used to differentiate metastases from other masses (eg, hemangioma) because the former are mostly hypovascular.
There has been some success in differentiating HCC from metastases, as Doppler shifts of greater than 5 kHz are reported to be specific for HCC. Moreover a basket-type pattern has been described for hepatomas on color-flow Doppler images. A Doppler shift of up to 4 kHz has been described in vascular metastases. On color-flow Doppler images, a hypovascular mass with venous or arterial flow meandering around the mass (detour sign) is occasionally seen around metastases; this finding reflects their mass effect in displacing such vessels.
Although color-flow Doppler is of limited value in adding specificity to a US diagnosis, it may be invaluable in localizing areas of vascularity to optimize the site for biopsy.
Intraoperative US and laparoscopic US
IOUS is an important diagnostic tool in patients undergoing hepatic resection for colorectal metastases. IOUS allows careful evaluation of the normal liver segments to exclude occult metastases in the segments that will be left in situ. The high accuracy of IOUS is a result of the contact scanning possible with a high-frequency transducer and color-flow Doppler imaging; with this technique, the complete organ may be covered without artifact. IOUS depicts 25-35% more lesions than does preoperative US. Most significantly, 40% of the lesions detected by means of IOUS are neither visible nor palpable and would presumably have been missed with other means. [57, 61]
IOUS has also been shown to be a sensitive means of detecting HCC, particularly if US contrast agents are used to improve Doppler images. IOUS has been used as an aid to liver resection since the end of the 1970s. This approach has been particularly useful in the resection of tumors from a cirrhotic liver; in such cases, conventional resection methods would result in high mortality and morbidity rates. IOUS combines the needs for adequate tumor resection with sparing of the liver parenchyma.
Operative US is used routinely during cryotherapy, or intraoperative freezing of metastases. The tip of the cryotherapy probe is placed in the center of the metastasis, which is then frozen with liquid nitrogen. As the metastasis freezes, it becomes echogenic and is seen as an echogenic sphere forming around the tip of the probe. Cryotherapy is applied until the echogenic sphere has replaced all of the visible metastasis with a margin, which fully includes the edges of the tumor to prevent recurrence. On follow-up, the metastasis forms a lollipop-shaped defect with a cystlike hypoechoic area representing the site of the treated tumor, which becomes necrotic with a tubular stem with the attenuation of fluid; this stem represents freezing around the probe shaft.
Good background knowledge of the liver surgical anatomy and of US is vital before one embarks on IOUS for surgical resection. At laparotomy, liver mobilization, effected by dividing the round, falciform, and triangular ligaments, is an essential prerequisite before liver exploration with IOUS. When the round ligament is pulled, the liver surface is widely exposed, and by following the portal venous branches and hepatic veins, the liver may be fully examined. The use of IOUS in liver resection may be schematically divided in 2 principal phases: liver exploration for staging the disease, and guidance of the surgical maneuvers.
IOUS also permits an accurate 3-dimensional reconstruction of the relationships between the tumor, the hepatic veins, and the portal branches. Moreover, the portal venous branches are used as landmarks in defining the resection line. This finding is fundamental for planning the surgical strategy.
In cirrhotic livers, the hard and irregular surface makes the detection of small nodules difficult by means of palpation. In 30-65% of patients, liver tumors smaller than 4-5 cm in diameter are not palpable. IOUS allows accurate localization of these tumors in 96-98% of patients. In the evaluation for HCC, IOUS allows the identification of 30% new hypoechoic, malignant nodules in a cirrhotic liver; this finding alters the surgical strategy. [57]
Moreover, laparoscopic US may help prevent unnecessary laparotomy in 63% of cases with nonresectable malignancies. [57] Tumor thrombi in the portal and hepatic veins and invasion of the biliary tree in the setting of HCC and other metastases are regarded as signs of advanced-stage disease, particularly with HCC. The tumor extension is readily seen on IOUS as hypoechoic masses occupying the vessel lumen. Liver resection for HCC may be performed in the presence of tumor thrombi in the portal vein trunk, and in this instance, IOUS allows an evaluation of the extent of the tumor thrombus, which determines the extent of liver resection. Though not completely satisfactory, IOUS remains the most accurate tool available for defining vascular tumor invasion.
Operative US may be used to guide segmental resection by allowing visualization of portal vein branches, which may then be injected with dye. This injection leads to staining of the liver segment, which accurately demarcates its vascular boundaries on the liver surface. This technique may be further refined with the insertion of a 6F balloon catheter into the supplying portal vein under IOUS guidance. Inflation of the placed balloon creates a relatively bloodless field for surgery.
Laparoscopic US is also valuable. It has an advantage over abdominal US in that the probe may be used to palpate the surface of the liver. This aids in the diagnosis of hemangiomas, which may be compressed, unlike solid tumors, which cannot.
Synchronous liver metastases are frequently encountered at surgery for GI malignancy; of these, as many as 40% are not palpable. IOUS is considered the standard for identifying liver metastases, and it enables the detection of 93% of liver metastases, as compared to 51% detection with preoperative CT and US; 66% are palpable at surgery. [57] The addition of contrast-enhanced IOUS using lipid-stabilized perfluorobutane microbubbles has been shown to provide additional information that can alter the surgical plans for patients with liver colorectal metastases. [62]
By better defining the hepatic venous vasculature, IOUS allows many more surgical resections for colorectal metastases than would otherwise be possible, on the basis of preoperative scanning. IOUS may cause the upstaging of colorectal metastases, preventing unnecessary surgery.
Degree of confidence
There is considerable debate regarding the choice of the ideal noninvasive imaging modality for the detection of liver metastases. The use of multiple modalities is both time-consuming and costly. One must therefore place US in the correct order within the diagnostic pathway. US is valuable, inexpensive, quick, and portable, and it may depict lesions as small as 1 cm.
The addition of Duplex, color Doppler, and tissue harmonic imaging and the use of US contrast enhancement have improved the sensitivity and specificity of US in the detection of focal liver lesions. US may also be used to guide access to focal liver lesions for biopsy.
IOUS is extremely sensitive for metastases not detected on preoperative scanning. The 90% sensitivity of IOUS approaches that of CT with the bolus injection of contrast material, and IOUS is the most sensitive test available for detecting liver focal lesions. IOUS of the liver has the highest sensitivity for the detection of focal liver abnormalities, with 96% accuracy, versus 84% accuracy for transabdominal US. At present, IOUS is more accurate than any other imaging modality and is used in the authors' unit for cases not adequately diagnosed and staged by US, CT, and MRI.
Hemangiomas, multicentric HCCs, multiple liver adenomas, complicated simple cysts, hydatid cysts, FNH, regenerative nodules, focal fatty sparing, and focal fatty infiltration may all mimic liver metastases.
With IOUS, a false-positive diagnosis occurs in 2-4% of cases; IOUS-guided biopsy that allows the examination of frozen sections may address this problem.
Nuclear Imaging
The standard sulfur colloid scans for the detection of liver metastases are no longer performed. The value of nuclear medicine studies lies in the fact that they may be used to characterize several of the benign liver lesions, which may mimic solitary or multiple metastases. The distinction of these lesions is a particular problem when one is staging a known primary cancer in a patient in whom benign focal liver masses are incidentally discovered. The colloid scan may be of great help in distinguishing a number of benign conditions that may mimic metastases and include fatty infiltration, focal nodular hyperplasia (FNH), and macroregenerative nodules (see the image below). [63, 64, 65, 66]
 Liver, metastases. Characteristic appearance of carcinoid liver metastases on planar indium-111 octreotide scan shows the primary lesion, mesenteric metastases, and multiple liver metastases.
Liver, metastases. Characteristic appearance of carcinoid liver metastases on planar indium-111 octreotide scan shows the primary lesion, mesenteric metastases, and multiple liver metastases.
The role of nuclear medicine in liver imaging has been undergoing great changes; for example, CT has replaced radionuclide imaging as the criterion standard screening tool for metastatic liver disease. Although conventional CT has a sensitivity of 85% for detecting any metastases, it is only 60% sensitive for individual lesions. The specificity for solitary lesions is also low with CT.
In a patient with a known primary malignancy, the presence of multiple liver lesions is highly suggestive of metastases. A solitary liver lesion in a patient with a known primary malignancy almost always requires further characterization. In such cases, imaging modalities such as MRI and radionuclide imaging are often necessary to make a specific diagnosis. Many of these lesions may be further characterized by performing scintigraphy; a specific diagnosis may be made with focal fatty infiltration, focal fatty sparing, FNH, liver abscesses, and hemangiomas.
Hepatic arterial perfusion scintigraphy
In cases of limited metastatic liver disease in patients with colorectal cancer, resection of metastases is associated with a 5-year survival rate of 25-30%. However, 30% of patients undergoing hepatic resection for colorectal metastases are known to have occult metastases that are not detected with CT, US, or sulfur colloid scanning. These patients may benefit from CT arterioportography (CTAP). CTAP works on principles similar to those of hepatic artery perfusion scintigraphy (HAPS). The study involves the infusion of technetium-99m (99mTc) macroaggregated albumin into a hepatic artery catheter. Metastases appear as areas of increased focal radionuclide uptake.
In combination with a triple-headed single-photon emission CT (SPECT) sulfur colloid scan, HAPS may show metastatic lesions as small as 0.5-1 cm. In a prospective study, Vogel and associates compared preoperative HAPS with CTAP and found sensitivities of 92% and 86% and positive predictive values of 73% and 60%, respectively. [67] HAPS showed more metastases; some of the lesions were not apparent at surgery, and blind biopsy was needed for confirmation.
More than 90% of GI carcinoids and their metastases are identified by use of somatostatin receptor scintigraphy. Accumulation often is seen in clinically unsuspected sites not recognized by other imaging techniques.
HAPS has a false-positive rate of 25%. How many of these lesions are truly false-positive is not known because patients with lesions deemed inoperable seldom undergo follow-up imaging. Describing the experience at 1 center, Drane showed that almost 50% of the lesions classified as false-positive were later proved to be liver metastases. [68]
Hepatic perfusion index
The hepatic perfusion index has been used to evaluate occult or subclinical liver metastases. The technique involves dynamic hepatic scintigraphy, which provides an estimate of the ratio of the total arterial blood flow to the total liver blood flow; this ratio is known as the hepatic perfusion index. Some believe that an increased hepatic perfusion index is associated with occult liver metastases, whereas others maintain that a low index is more important. A low index suggests that the patient is at a low risk for metachronous tumors, and therefore, they may be spared from adjuvant chemotherapy.
Tc sulfur colloid scintigraphy
Sulfur colloid scintigraphy has largely been abandoned as an imaging test for liver metastases despite its reasonably high sensitivity for the detection of metastatic disease (80-85%). The lesions appear as photon-deficient defects, which are nonspecific. Also, the sensitivity of planar imaging decreases dramatically for surface lesions smaller than 2 cm and deeper lesions smaller than 3-4 cm in diameter. A genuine liver lesion within a fatty liver may be missed or mischaracterized on other imaging studies. In such instances, sulfur colloid scanning may be useful in confirming or excluding a mass lesion in the liver.
Sulfur colloid scans may still be indicated when the CT findings are nondiagnostic because of a fatty liver. SPECT imaging has improved the overall sensitivity but at the expense of reduced specificity because of problems with distinguishing small lesions near the heart or intrahepatic vessels. Because the Kupffer cells are unaffected by fatty infiltration, sulfur colloid scans are typically normal. Sulfur colloid scintigraphy is highly sensitive and specific for focal fatty infiltration.
The imaging modalities that best characterize focal nodular hyperplasia (FNH) are those that can delineate the central scar or that can show Kupffer cell activity. CT and MRI demonstrate the central scar best, whereas radionuclide scans best demonstrate Kupffer cell activity. The introduction of MRI with superparamagnetic contrast agents may challenge the role of radionuclide scanning in the future.
Hepatocellular neoplasms such as a hepatocellular adenoma and hepatocellular carcinoma (HCC) may also have Kupffer cells, and they may demonstrate sulfur colloid uptake. Typically, hepatic adenomas appear photopenic on sulfur colloid scans, but colloid uptake in a liver lesion does not exclude a hepatic adenoma.
Hepatic adenoma, hemangioma, hepatoblastoma, liver herniation, and HCC may have similar appearances on 99mTc sulfur colloid scans.
Somatostatin receptor analogue scintigraphy
Somatostatin receptor scintigraphy is not specific for carcinoids. Uptake occurs in other lesions with a high density of somatostatin receptors; these include gastrinomas, glucagonomas, somatostatinomas, vasoactive intestinal polypeptide tumors, neural crest tumors (paragangliomas, medullary thyroid carcinomas, neuroblastomas, pheochromocytomas), oat cell lung carcinomas, and lymphoproliferative disease (Hodgkin and non-Hodgkin lymphoma). In addition, the possibility of uptake in areas of lymphocyte concentration in inflammatory states must be kept in mind. Approximately 20% of gastrinomas are missed during somatostatin receptor analogue scintigraphy.
Somatostatin receptor analogue scintigraphy has had the greatest impact on the diagnosis of gastrinomas; it has a sensitivity and a specificity of 80-90% for the detection of both primary and metastatic sites. Somatostatin receptor analogue scintigraphy may depict subcentimeter liver metastases with a high signal-to-noise ratio. Somatostatin receptor analogue scintigraphy has been reported to show uptake in insulinomas, glucagonomas, small-cell lung cancer, thyroid cancer, and carcinoids.
Somatostatin receptor analogue scintigraphy may prove useful in the treatment of patients with hypergastrinemic states who have increased incidence of gastric carcinoids. In patients with multiple endocrine neoplasia type 1 (MEN-1), localization in the upper abdomen may not be associated with a pancreatic endocrine tumor; instead, it may be caused by a gastric carcinoid.
With pancreatic carcinoid, somatostatin analogue scintigraphy has been proven to be sensitive, although findings are nonspecific because the scan also may yield positive findings for islet cell tumors. Regarding small-bowel carcinoid, somatostatin receptor scintigraphy performed with indium-111 (111In) octreotide and 111In pentetreotide is used to image many neuroendocrine tumors, including carcinoids that possess somatostatin-binding sites. Several studies have shown that this method is sensitive and noninvasive for imaging primary carcinoid tumors and carcinoid metastatic spread. The addition of single-photon emission CT (SPECT) further refines the technique, increasing sensitivity.
Scintigraphy performed with iodine-123 (123I) metaiodobenzylguanidine (MIBG) demonstrates 44-63% uptake in GI carcinoids. A higher frequency of uptake is found in midgut carcinoids and in tumors with elevated serotonin levels.
Somatostatin receptor analogue scintigraphy is regarded as the imaging modality of first choice in the diagnosis of the primary site for a gastrinoma (Zollinger-Ellison syndrome) and its metastases. The overall sensitivity of somatostatin receptor analogue scintigraphy is 70% for carcinoids, 40% for insulinomas, and 30% for glucagonomas.
With medullary thyroid carcinoma metastases, dimercapto-succinic acid (V) [DMSA(V)] and 201Tl are used as complementary agents to detect more than 95% of tumor sites. The advantage of scintigraphy over anatomic cross-sectional imaging is that the former shows the viability of tumors that have been treated with ablative procedures.
FDG-PET
High rates of tumor recurrence after liver resection for colorectal metastases suggest that current imaging strategies are failing to detect occult liver and extrahepatic metastases. Although FDG-PET cannot match the anatomic resolution of cross-sectional imaging, it is particularly useful in the detection and characterization of extrahepatic disease that may not be identified on cross-sectional imaging. [14, 15, 18, 21, 69, 70, 71]
Fluorodopa F-18-PET has been used to image primary GI carcinoid tumors and lymph node and organ metastases, with promising results. FDG PET imaging is now more available and more widely used. In general, FD- PET is useful in cases of poorly differentiated carcinoids and other neuroendocrine tumors, but it should not be used as a first-line imaging agent. FDG-PET is primarily useful when somatostatin receptor scintigraphy results are negative. Fluorodopa F-18-PET is a useful supplement to morphologic imaging methods. FDG-PET imaging is useful in poorly differentiated carcinoids when somatostatin receptor scintigraphy results are negative.
Rohren and associates have shown that in patients being evaluated for potential curative resection of hepatic metastases from colorectal cancer, FDG-PET is accurate for identifying metastatic disease to the liver. [72] The sensitivity and specificity of FDG-PET are 95% and 100%, respectively. However, the detection of individual metastases depends on their size, and anatomic imaging methods such as IOUS more accurately depict their distribution and size. FDG-PET is also more accurate than CT and carcinoembryonic antigen (CEA) studies for detection of recurrent colorectal cancer.
The detection rate for liver metastases is generally better for CT than for FDG-PET (80% vs 65%). This rate is related to tumor size; therefore, the false-negative rate is significant. Several sources of benign and physiologic increases in activity may yield false-positive results.
(See the images below.)
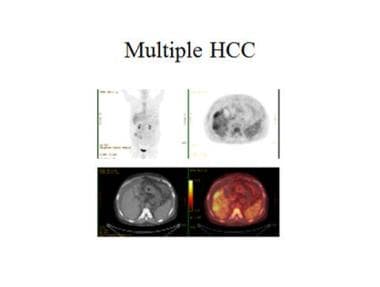 Fluorine-18 fluorodeoxyglucose (FDG) positron emission tomography (PET) has a proven record as a valuable tool in the initial diagnosis, staging, and restaging of many cancers. The sensitivity of FDG-PET in detecting hepatocellular carcinoma 5 cm or smaller in size is low. However, for larger tumors, there is a strong correlation of sensitivity and uptake intensity with tumor size and elevated alpha-fetoprotein levels. FDG-PET sensitivity and uptake intensity does not correlate with histologic grade. Whether FDG PET offers any benefit over traditional imaging has yet to be determined. Nevertheless, extrahepatic disease is depicted well on FDG PET. Courtesy of Dr Ghulam Mustafa Shah Syed.
Fluorine-18 fluorodeoxyglucose (FDG) positron emission tomography (PET) has a proven record as a valuable tool in the initial diagnosis, staging, and restaging of many cancers. The sensitivity of FDG-PET in detecting hepatocellular carcinoma 5 cm or smaller in size is low. However, for larger tumors, there is a strong correlation of sensitivity and uptake intensity with tumor size and elevated alpha-fetoprotein levels. FDG-PET sensitivity and uptake intensity does not correlate with histologic grade. Whether FDG PET offers any benefit over traditional imaging has yet to be determined. Nevertheless, extrahepatic disease is depicted well on FDG PET. Courtesy of Dr Ghulam Mustafa Shah Syed.
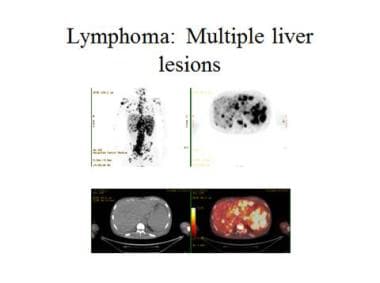 Fluorine-18 fluorodeoxyglucose (FDG) positron emission tomography (PET) showing multiple lymphoma deposits in the liver, spleen, and bone. Courtesy of Dr Ghulam Mustafa Shah Syed.
Fluorine-18 fluorodeoxyglucose (FDG) positron emission tomography (PET) showing multiple lymphoma deposits in the liver, spleen, and bone. Courtesy of Dr Ghulam Mustafa Shah Syed.
CEA immunoscintigraphy
CEA is a tumor-associated antigen arising from the endodermally derived epithelium of the GI tract. It is expressed in a variety of adenocarcinomas, such as colorectal cancer. CEA is a self-antigen not recognized by the immune system as a foreign substance; therefore, it does not provoke an immune response. CEA occurs on the cell membrane of colorectal carcinomas. An anti-CEA antibody derived from a murine monoclonal Fab' fragment when labeled with 99mTc enables the imaging of CEA-expressing tumors. The technique may be refined by combining CEA immunoscintigraphy with CT.
The combined CT and CEA method has a sensitivity of 78%, a specificity of 87%, an accuracy of 79%, and a positive predictive value of 99%. The technique is twice as accurate as CT imaging alone in patients with occult disease, with a rate of 61%, as compared with 33%. The method may depict normal-sized lymph nodes affected with metastatic disease. The anti-CEA antibody is antigenic and may cause anaphylaxis, although reactions to the drug are rare.
CEA is expressed in inflammatory conditions such as Crohn disease; therefore, there is a potential for false-positive diagnoses. Activity in a normal liver, kidney, heart, and aorta also may lead to a false-positive diagnosis. The liver is the major site of normal uptake; therefore, detecting metastatic sites in the liver may be difficult. Colloid subtraction has been incorporated, but the results offer no great promise.
Tc-pertechnetate–labeled RBC scintigraphy
The sensitivity of labeled-RBC scanning with planar images is 69-82% for tumors larger than 1.9 cm. The specificity and positive predictive value approach 100%. With the addition of SPECT, sensitivities rise sharply to almost 100% for tumors larger than 2 cm and to 93% for tumors measuring 1.1-2 cm. SPECT also defines tumors near the kidney and spleen with greater sensitivity. With a 3-headed gamma camera and SPECT, lesions as small as 0.5 cm can be detected.
Fibrotic or thrombotic hepatic cavernous hemangiomas may yield a false-negative result with a labeled-RBC technique because the mass may remain photo deficient, and increased blood pool activity is not seen. A false-positive perfusion–blood pool mismatch is rarely seen; it has been reported in 4 cases of HCC, 2 cases of angiosarcoma, and 2 cases of colonic metastases.
Xe radionuclide scanning
The sensitivity of Xenon-133 (133Xe) radionuclide scanning is only 60-70%; therefore, the test is best reserved for cases in which the index of clinical suspicion for focal fatty change is high and the results of sulfur colloid scanning are equivocal.
Ga scintigraphy
In 88% of cases of HCC, gallium-67 (67Ga) uptake is equal to or greater than the liver background activity and corresponds to the photon-deficient defects on the sulfur colloid scan. When no gallium uptake occurs in a defect identified on a sulfur colloid scan, HCC may be excluded.
Hepatoiminodiacetic acid (HIDA) uptake has been described in 50.6% of HCCs. HIDA uptake has been linked to a better prognosis for patients with HCC. Using Tc-99m disofenin (DISIDA [diisopropyl iminodiacetic acid]), Calvet and associates found 70% uptake in well-differentiated HCC, 30% uptake in moderately well differentiated HCC, and no uptake in poorly differentiated HCC. [73]
Differentiation from focal fat
Results of sulfur colloid scans are usually normal, with focal fatty infiltration and focal fatty sparing, because Kupffer cells are not affected by steatosis.
Xenon-133 (133Xe) is highly fat-soluble. After its inhalation, it characteristically concentrates in areas of focal fatty infiltration. The intensity of the radionuclide concentration is related to the fat content.
Differentiation from FNH
Sulfur colloid uptake in patients with FNH depends on the concentration of Kupffer cells in the FNH lesion. The detection of the Kupffer cells in FNH lesions has historically been the role of scanning with 99mTc sulfur colloid. In approximately 60-70% patients with FNH, scans show homogeneous uptake of 99mTc sulfur colloid. In the remaining 30-40%, the Kupffer cells in the FNH lesion are not sufficiently concentrated to demonstrate activity, and the lesion may in fact be photon deficient. Tc-99m hepatoiminodiacetic acid (HIDA) may show normal to increased uptake in 40-70% of patients; the lesion may be photon deficient in as many as 60% of patients. With 99mTc-tagged RBCs, uptake is increased during the early phase; thereafter, diminished uptake is seen in the lesion relative to the liver.
The imaging modalities that can best characterize FNH are those that can delineate the central scar or that can show Kupffer cell activity. CT and MRI demonstrate the central scar best, whereas radionuclide scans demonstrate Kupffer cell activity.
Differentiation from hemangioma
Hepatic cavernous hemangiomas are the most common benign tumors of liver. They are typically found incidentally on imaging studies, laparotomy, or autopsy. Although they are usually solitary, as many as 30% are multiple. Scintigraphy labeled with 99mTc-pertechnetate–labeled RBC provides a specific and noninvasive method for diagnosing cavernous hemangioma. The typical appearance is that of an initial photon-deficient mass, followed by gradual filling in of the mass with the labeled RBCs from the periphery to the center. Eventually, the entire mass is completely filled. This finding has been called perfusion–blood pool mismatch. The addition of SPECT improves the detection of smaller lesions.
Differentiation from liver abscess
With gallium-67 (67Ga) scintigraphy, gallium is concentrated in pyogenic liver abscesses; hot spots are seen in more than 80% patients with liver abscesses. Gallium is concentrated in amebic abscesses only at the periphery of the lesions.
Differentiation from HCC
On 99mTc sulfur colloid scan, HCC appears as a nonspecific photon-deficient mass, whereas a 67Ga scan confirms activity in the area of photon deficiency seen with colloid scintigraphy. Radionuclide scanning may be particularly useful when a questionable lesion is seen with US, CT, or MRI.
Thallium-201 (201Tl) also accumulates in HCC, and 201Tl imaging may be substituted for gallium scanning and used in combination with phytate colloid scintigraphy and a subtraction technique to eliminate background liver activity.
Tc-99m HIDA and other iminodiacetic acid (IDA) compounds also accumulate in HCC. The intensity of uptake of IDA compounds is a predictor of prognosis; increased uptake may reflect better tumor differentiation and hence result in a better prognosis. Using disofenin (DISIDA), Calvet and associates found 70% uptake in well-differentiated HCC, 30% uptake in moderately well differentiated HCC, and no uptake in poorly differentiated HCC. [73]
Medullary thyroid carcinoma metastases
A variety of radionuclides may be used to detect medullary thyroid carcinoma and its metastases. These metastases may be imaged with iodine-131 (131I) MIBG, 111In octreotide, 99mTc dimercapto-succinic acid (V) (DMSA[V]), 201Tl, 99mTc sestamibi, and FDG. Because sufficient experience has not been gained with any one agent and no comparative trial is possible, the choice of the agent to be used is determined on the basis of local expertise, availability, and cost. DMSA(V) and 201Tl, or a combination of the 2 agents, is the least expensive agent and used in some centers.
Angiography
The following videos demonstrate traditional angiography, CTA, and rotational angiography in a patient with liver metastases.
The blood flow to liver metastases is almost invariably increased relative to that of the liver. However, the degree of vascularity, as demonstrated on angiograms, bears no relationship to the blood flow in the tumor, as measured physiologically. The vascularity varies with the primary site. Liver metastases from GI and pancreatic primary sites may be mildly hypervascular to moderately hypovascular (see the images below).
 Liver, metastases. Celiac-axis angiograms show the characteristic appearance of carcinoid liver metastases, with early enhancement of the metastases in the arterial phase.
Liver, metastases. Celiac-axis angiograms show the characteristic appearance of carcinoid liver metastases, with early enhancement of the metastases in the arterial phase.
 Liver, metastases. Celiac-axis angiogram shows the characteristic appearance of carcinoid liver metastases, with persistent enhancement of the metastases in the capillary phase.
Liver, metastases. Celiac-axis angiogram shows the characteristic appearance of carcinoid liver metastases, with persistent enhancement of the metastases in the capillary phase.
A number of primary tumors may generate hypervascular liver metastases. These include neuroendocrine tumors; renal cell carcinomas; thyroid carcinoma; and choriocarcinoma, which are occasionally confused with hepatic hemangiomas. Metastases from a bronchogenic carcinoma and cancers of the esophagus are usually hypovascular. Liver metastases from breast cancer, ocular melanoma, cholangiocarcinoma, and sarcomas may be hypervascular or hypovascular.
Hypervascular metastases stand out as rounded areas of increased accumulation of contrast material against the homogeneously enhancing liver in the capillary phase. They are usually rounded, and most are peripheral. Most liver metastases are multiple. In larger tumors, abnormal vessels may be seen within the tumor. Larger metastases may stretch or displace the hepatic arteries.
Choriocarcinoma metastases are one the most vascular hepatic tumors that may bleed spontaneously and undergo central necrosis when the tumor outgrows its blood supply. Liver metastases from a renal cell carcinoma may have florid vascularity, and they may show arteriovenous shunting indistinguishable from that of hepatocellular carcinoma (HCC). Carcinoid, islet cell metastases, and metastases from a leiomyosarcoma are also hypervascular, but to a lesser degree.
When liver metastases are hypovascular relative to the liver, the tumors stand out as avascular defects in the capillary phase of the hepatic angiogram (hepatogram phase). If the hypovascular metastases are multiple, the hepatogram phase of the liver resembles Swiss cheese. Liver metastases with vascularity similar to that of the liver parenchyma are usually difficult to detect. The diagnosis of these tumors depends on the finding of invasion and/or displacement or compression of the main hepatic artery or its branches. Rarely, compressed hepatic arteries show delayed drainage of contrast material.
Angiography for CT with ethiodol or lipiodol
Lipiodol (Ethiodol; ethiodized oil) is an iodized ester of the fatty acid of poppy seed oil. After 5-20 mL of the iodized oil is injected into the hepatic artery via an angiographically placed catheter, prolonged retention of the agent is observed within hypervascular liver tumors, particularly those of HCC. However, how the liver handles the iodized oil is still not clear. The greater permeability of the tumor vessels is thought to result in increased delivery of the oil into foci of HCC. Previously, it was widely believed that droplets of iodized oil occluded small hepatic arteries within the tumor. However, the fact that the iodized oil opacifies the portal vein in a dose-dependent fashion indicates that the oil first seals the hepatic sinusoids, and when sufficient oil has been administered, the oil refluxes back into the portal venous system via arterioportal communication. Additionally, the clearance of iodized oil from HCC is slow, probably because of the absence of Kupffer cells and lymphatics in HCC and other malignant tumors, which are believed to clear the oil from the normal liver parenchyma.
CT performed a week after iodized oil embolization shows the retention of the iodized oil within the tumor as high-attenuating foci. The technique is frequently used in the diagnosis and infusion therapy of HCC. The technique is highly sensitive in the diagnosis of small HCC, as well as additional small satellite intrahepatic metastatic nodules of HCC.
Four patterns of iodized oil uptake have been described in hepatic tumors:
-
Type 1: homogeneous diffuse uptake, typically seen in primary liver tumors
-
Type 2: no uptake, as seen in non-HCC metastases
-
Type 3: peripheral thin rim of uptake, also associated with metastases
-
Type 4: thick rim of uptake, seen only in hemangiomas
Angiography for CTAP
CT arterioportography (CTAP) is based on the intense enhancement of normal liver parenchyma that can be achieved when radio-iodinated contrast material is injected via a catheter placed in the superior mesenteric or splenic artery. The liver is imaged in the portal venous phase when maximum liver-to-lesion attenuation difference occurs. Because the portal vein does not normally supply liver tumors, lesions in the liver stand out as low-attenuating areas. Complete hepatic angiography in conjunction with CTAP is useful because vascular invasion or vascular encasement that may affect tumor resectability is better depicted with angiography than with other means.
Angiography for planning regional therapy
Chemoembolization improves survival rates in select patients with unresectable HCC; those with other tumors (eg, metastatic hepatic carcinoids) may benefit from embolization alone. These therapies are delivered via safely placed arterial catheters. Accurate depiction of arterial anatomy is an essential prerequisite for the safe delivery of these therapies.
Angiography not only depicts variation in the arterial blood supply and collaterals to the GI tract but also permits an assessment of portal vein patency. Hypervascular tumors such as HCC develop a parasitic blood supply from the phrenic, intercostal, internal mammary, lumbar, gastroduodenal, and superior mesenteric arteries. When tumors with parasitic blood supply are being treated, some of the tumor may escape treatment. These parasitic blood vessels themselves may be superselectively catheterized and the tumor carefully embolized.
Vessels arising from the hepatic arteries and supplying the gut have been recognized to prevent nontarget embolization. The right gastric artery may originate near the proper hepatic artery bifurcation or, more commonly, from the proximal left hepatic artery. The left hepatic artery may originate from a common left gastric–left hepatic arterial trunk. The identification of these variations is critical for safe chemoembolization.
Degree of confidence
Angiography has no direct role in the diagnosis of liver metastases. However, angiography has high sensitivity in the detection of hypervascular metastases as small as 0.5-1 cm in diameter. Hypovascular metastases must be approximately 2-3 cm or larger in diameter to be identified by means of angiography.
The sensitivity and specificity of iodized oil CT in the diagnosis of HCC has been described as being as high as 97.1% and 76.9%, respectively; the reported accuracy is 88.3%. The positive predictive value of iodized oil CT for the diagnosis of HCC liver metastases is 90.5%. The differentiation between adenomatous hyperplastic nodules and HCC may sometimes be difficult. However, iodized oil is not normally accumulated in adenomatous hyperplastic nodules, because the nodules derive their blood supply from the portal venous system. Therefore, the risk of confusing adenomatous hyperplastic nodules with HCC is insignificant with iodized oil CT.
CTAP has a sensitivity of 90% in the detection of liver metastases that are 5 mm or smaller, because of the greater differences in liver and lesion attenuation. The specificity of CTAP is low because both benign and malignant lesions appear as hypoattenuating perfusion defects. Problems may arise if scanning begins too early, because suboptimal enhancement of hepatic veins may be misinterpreted as focal liver lesions. Nontumorous perfusion defects have been described in situations involving the following: faulty technique; laminar flow in the portal vein produced by rapid venous return; focal fatty infiltration; and aberrant blood supply to the liver. Delayed scanning is usually advocated to distinguish pseudolesions from genuine liver masses.
With diffuse malignant infiltration of the liver, determining whether hypervascular areas in the liver represent metastases may be difficult. Diffuse malignant infiltration may also mimic cirrhosis, obstructive jaundice, or cholangitis on angiography. If these areas are rounded, they are more likely to represent metastases.
The detection of metastases to the left lobe is more problematic because the left lobe may be partially obscured by the stomach parenchyma and spleen, and it lies over the spine. Hence, if left-lobe metastases are suspected, selective left-lobe angiography is indicated.
Angiographic results may be falsely negative if liver metastases have vascularity similar to that of the liver parenchyma. Most liver metastases are multiple; however, if a solitary metastatic deposit occurs, it may be difficult to differentiate from a primary benign or malignant liver neoplasm. Moreover, HCC, adenomas, and hemangiomas may be multiple. Hemangiomas may coexist with FNH.
The diagnosis of pancreatic liver metastases may also be problematic because biliary tree dilatation is often present. This finding may be gross and appear as hypovascular tumors. Biliary dilatation caused by an ampullary carcinoma may have a similar appearance; it may have a Swiss cheese appearance of liver metastases.
Iodized oil CT has some limitations. Because the uptake of iodized oil depends on increased tumor vascularity, small HCCs that are avascular and necrotic, as well as small fibrotic subtypes of HCC, may be missed. Uptake may also be limited in cases in which HCC was previously ablated with alcohol, presumably as a result of alcohol-related vascular damage.
A false-positive diagnosis with iodized oil CT may occur because uptake may occur in benign lesions and within the normal parenchyma in the presence of focal inflammation and arteriovenous shunting. HCC lesions usually show homogeneous uptake, but patchy uptake has been described in large necrotic HCCs, hemangiomas, metastases, and focal nodular hyperplasia (FNH); this feature may pose diagnostic difficulties.
-
Liver, metastases. The metastatic cascade in the development of liver metastases.
-
Liver, metastases. Diagram showing the mechanism of the local-regional spread of colorectal liver metastases.
-
Liver, metastases. Graph showing results from resection of a colorectal liver metastasis.
-
Liver, metastases. Photograph of the various types of cryosurgery probes available.
-
Liver, metastases. Photograph of a cryosurgery probe and ultrasonography in use.
-
Liver, metastases. Ultrasonographic monitoring of the freezing created by cryosurgery probe.
-
Liver, metastases. A case against liver biopsy. This 68-year-old woman was referred for resection of an isolated liver metastases found at the time of colectomy. The patient underwent laparoscopy and laparoscopically guided liver biopsy. A surface lesion was examined at biopsy. At 6 weeks, the patient underwent laparotomy. At laparotomy, several surface metastatic deposits were identified in the liver around the biopsy site, and numerous small peritoneal metastases were present.
-
Liver, metastases. Plain radiograph of the upper abdomen shows gross hepatomegaly and multiple conglomerates of punctate calcification in the right hypochondrium encroaching on the left hypochondrium. The final diagnosis was a medullary carcinoma of the thyroid (calcified) with calcified hepatic metastases.
-
Liver, metastases. Characteristic appearance of carcinoid liver metastases with different imaging modalities. Axial sonogram through the liver shows multiple fairly well-defined echogenic liver metastases of varying sizes.
-
Liver, metastases. Characteristic appearance of carcinoid liver metastases on a contrast-enhanced axial CT scan through the upper abdomen. Portal venous phase image shows the metastases as negative defects against the normally enhancing liver
-
Liver, metastases. Characteristic appearance of carcinoid liver metastases on contrast-enhanced axial CT scan through the upper abdomen, which shows early arterial enhancement of the liver metastases.
-
Liver, metastases. Characteristic appearance of carcinoid liver metastases on a gadolinium-enhanced axial MRI through the liver. Image shows early arterial enhancement of multiple liver tumors.
-
Liver, metastases. Characteristic appearance of carcinoid liver metastases on a gadolinium-enhanced axial MRI through the liver. Image shows portal venous phase enhancement of multiple liver tumors.
-
Liver, metastases. Characteristic appearance of carcinoid liver metastases on planar indium-111 octreotide scan shows the primary lesion, mesenteric metastases, and multiple liver metastases.
-
Liver, metastases. Characteristic appearance of carcinoid liver metastases on single-photon emission CT scans obtained with indium-111 octreotide. Images show liver lesions in detail.
-
Liver, metastases. Celiac-axis angiograms show the characteristic appearance of carcinoid liver metastases, with early enhancement of the metastases in the arterial phase.
-
Liver, metastases. Celiac-axis angiogram shows the characteristic appearance of carcinoid liver metastases, with persistent enhancement of the metastases in the capillary phase.
-
Liver, metastases. Contrast-enhanced transaxial CT images in the portal venous phase through the liver of a 48-year-old man with colonic metastases. The left image shows metastases in both lobes of the liver and, thus, inoperable. The right image was taken 2 months after oxaliplatin therapy. The metastases were downstaged. The patient underwent a successful right hepatectomy.
-
Contrast-enhanced CT scans taken in the portal venous phase show a hypervascular metastatic deposit from a renal cell carcinoma. The patient had a previous right hepatectomy for an earlier renal cell solitary metastatic deposit.
-
CT scan in the same patient as in the previous image following immunotherapy. Note the considerable reduction in the size of the liver lesion.
-
Contrast-enhanced CT scan in a patient who had undergone a left hepatectomy for a hepatocellular carcinoma. The patient has developed a small metastatic deposit within the liver remnant (arrow in the upper 2 frames). The lower 2 frames were taken after alcohol ablation.
-
Recurrent/metastatic hepatocellular carcinoma following chemoembolization. Note the intense iodized oil uptake, tumor necrosis, and air within the necrotic tumor. Also note the iodized oil uptake in the smaller, satellite tumors.
-
CT scan of a 52-year old man with a previous chemoembolization for hepatocellular carcinoma who had a recurrent tumor adjacent to the previously embolized tumor. This scan was taken following alcohol ablation.
-
Contrast-enhanced CT scan in a patient with colorectal liver metastases.
-
CT scan in the same patient as in the previous image shows the placement of radiofrequency probes.
-
Contrast-enhanced CT scan in the same patient as in the previous 2 images with colorectal liver metastases.
-
Liver metastases. Mimics. A 2.5-cm echogenic nodule in the left lobe of the liver was confirmed to be a hemangioma on further imaging.
-
Liver metastases. Mimics. Dynamic MRIs in a 36-year-old woman referred for a gallbladder ultrasonography. The patient was found to have a vague, ill-defined, hypoechoic mass within the right lobe of the liver. Gadolinium-enhanced T1-weighted MRI (top left) demonstrates an ill-defined hypointense mass, which is intensely enhancing in the arterial phase after the administration of contrast (top right). Minor enhancement persists in the portal venous phase (bottom left). On delayed images, the lesion becomes isointense relative to the liver (bottom right). The appearances are characteristic of focal nodular hyperplasia.
-
Traditional angiography in a patient with liver metastases. Courtesy of Memorial Sloan-Kettering Cancer Center, featuring Constantinos T. Sofocleous, MD, PhD.
-
Computed tomography angiography in a patient with liver metastases. Courtesy of Memorial Sloan-Kettering Cancer Center, featuring Constantinos T. Sofocleous, MD, PhD.
-
Rotational angiography in a patient with liver metastases. Courtesy of Memorial Sloan-Kettering Cancer Center, featuring Constantinos T. Sofocleous, MD, PhD.
-
Fluorine-18 fluorodeoxyglucose (FDG) positron emission tomography (PET) has a proven record as a valuable tool in the initial diagnosis, staging, and restaging of many cancers. The sensitivity of FDG-PET in detecting hepatocellular carcinoma 5 cm or smaller in size is low. However, for larger tumors, there is a strong correlation of sensitivity and uptake intensity with tumor size and elevated alpha-fetoprotein levels. FDG-PET sensitivity and uptake intensity does not correlate with histologic grade. Whether FDG PET offers any benefit over traditional imaging has yet to be determined. Nevertheless, extrahepatic disease is depicted well on FDG PET. Courtesy of Dr Ghulam Mustafa Shah Syed.
-
Fluorine-18 fluorodeoxyglucose (FDG) positron emission tomography (PET) showing multiple lymphoma deposits in the liver, spleen, and bone. Courtesy of Dr Ghulam Mustafa Shah Syed.







