Practice Essentials
Legg-Calvé-Perthes (LCPD) disease is a childhood hip disorder that results in infraction of the bony epiphysis of the femoral head. LCPD represents idiopathic avascular necrosis of the femoral head. The disease is bilateral in 10-20% of patients and usually affects children aged 4-8 years. When both hips are involved, they are usually affected successively, not simultaneously. A family history is present in 5-6% of patients. [1] In adults, the corresponding condition is termed Chandler disease. [2, 3]
Although the etiology is unclear, certain risk factors have been identified in children, including sex, socioeconomic group, and the presence of an inguinal hernia and genitourinary tract anomalies. More specifically, boys are affected 3 to 5 times more often than girls, and the incidence increases in low socioeconomic groups and in children with low birth weight. [4] Determining the prognosis is important at the time of presentation, because more than 50% of patients with LCPD do not require treatment. [5] A systematic review and meta-analysis by Adulkasem et al identified that In cases of severe LCPD requiring treatment, combined osteotomy was the most effective surgical procedure. [6]
Imaging modalities
Plain radiography remains the major modality for the evaluation of LCPD. Staging of the disease is based on plain radiographic findings. [7, 8] Scintigraphy is a useful technique in early disease, when plain radiographic findings may be normal; with scintigraphy, abnormalities become apparent earlier in the course of disease than they do with plain radiography. Computed tomography (CT) scans allow early diagnosis of bone collapse and curvilinear zones of sclerosis early in the disease process, when plain radiography is less sensitive. CT scans can also demonstrate subtle changes in the bone trabecular pattern. Ultrasonography is useful in the preliminary diagnosis of transient synovitis of the hip and the onset of LCPD. [9] Hip effusion with capsular distention is well depicted on sonographic images. [10, 11, 12, 13, 14] Magnetic resonance imaging (MRI) is as sensitive as isotopic bone scanning and allows more precise localization of involvement than conventional radiography. [3, 15, 16, 17, 18, 19, 20]
Plain radiographic findings may be entirely normal in early symptomatic disease. Although abnormalities become apparent with scintigraphy earlier in the course of disease than they do with radiography, abnormal scintigraphic findings are nonspecific; findings may be positive in patients with trauma, synovitis, and infections.
The use of CT scanning is limited by the comparatively higher radiation dose. Ultrasonographic diagnosis of LCPD is based on a demonstration of hip effusion, which is a nonspecific finding. On MRI scans, the changes seen as bone marrow edema and joint effusions are nonspecific. Angiography, venography, and arthrography are invasive procedures and do not provide significantly better clinical information for guiding therapeutic options.
(The radiologic features of LCPD are demonstrated in the images below.)
 Legg-Calvé-Perthes disease. Stage II disease. Note the slight widening of the left hip joint, representing a small joint effusion. Joint widening can also be secondary to hypertrophy of the cartilage.
Legg-Calvé-Perthes disease. Stage II disease. Note the slight widening of the left hip joint, representing a small joint effusion. Joint widening can also be secondary to hypertrophy of the cartilage.
 Legg-Calvé-Perthes disease. Plain radiograph in an adult patient with residual coxa magna and plana deformity with superimposed joint changes.
Legg-Calvé-Perthes disease. Plain radiograph in an adult patient with residual coxa magna and plana deformity with superimposed joint changes.
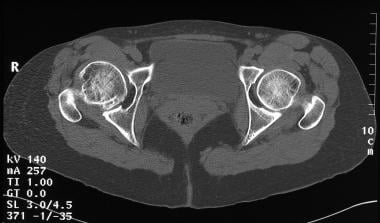 Legg-Calvé-Perthes disease. Axial nonenhanced CT scan through the hip joints in the same patient as in the previous image more clearly shows the loss of structural integrity of the right femoral head.
Legg-Calvé-Perthes disease. Axial nonenhanced CT scan through the hip joints in the same patient as in the previous image more clearly shows the loss of structural integrity of the right femoral head.
 Legg-Calvé-Perthes disease. Nonenhanced axial CT section through the hip joints obtained at a different level in the same patient as in the previous 2 images. Once again, the scan shows the loss of structural integrity of the right femoral head. Note the acetabular subchondral sclerosis.
Legg-Calvé-Perthes disease. Nonenhanced axial CT section through the hip joints obtained at a different level in the same patient as in the previous 2 images. Once again, the scan shows the loss of structural integrity of the right femoral head. Note the acetabular subchondral sclerosis.
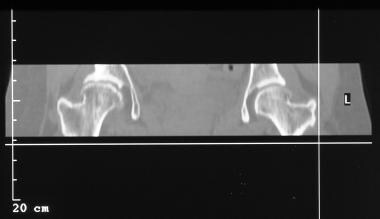 Legg-Calvé-Perthes disease. Coronal reconstruction shows flattening, sclerosis, and early fragmentation of the right femoral head (same patient as in the previous 3 images).
Legg-Calvé-Perthes disease. Coronal reconstruction shows flattening, sclerosis, and early fragmentation of the right femoral head (same patient as in the previous 3 images).
Staging
LCPD has 4 phases, as follows [2] :
-
Initial or necrosis phase: Interruption of vascular supply and bone necrosis. At this stage, the Waldenström sign is visible, which is characterized by increased joint space, secondary to a subchondral fracture.
-
Fragmentation phase: Initiated by a process of resorption of necrotic bone. Radiologically, dense bone islets appear; the central ones are condensed, and the lateral ones undergo osteolysis producing an image with multiple lines.
-
Reossification phase: Density is displaced in the opposite direction, the epiphysis is invaded by vessels, the dense islets are reabsorbed, and irregular bone tissue is formed, which then trabeculates. Repair begins with disappearance of the metaphyseal osteolysis.
-
Final phase, of healing or residual deformity: Necrotic bone is completely replaced by newly formed bone. The newly formed bone has a lower rigidity, so it can be remodeled in such a way that the morphology of the femoral head adapts to the shape of the insertion hole.
Several staging schema are used to determine severity of disease and prognosis; these include the Catterall, Salter-Thomson, and Herring systems. [21]
The Catterall classification is based on radiographic appearances and specifies 4 groups during the period of greatest bone loss. Catterall staging is as follows [22] :
-
Stage I — Histologic and clinical diagnosis without radiographic findings
-
Stage II — Sclerosis with or without cystic changes with preservation of the contour and surface of femoral head
-
Stage III — Loss of structural integrity of the femoral head
-
Stage IV — Loss of structural integrity of the acetabulum
The Catterall classification was developed to be applied in the fragmentation phase, which results in difficult and inaccurate initial assessment in early phases. Grouping tended to change if the classification was applied too early. Another criticism has been the lack of sufficiently high levels of interobserver agreement. [22]
The Salter-Thomson classification simplifies the Catterall classifications by reducing the groups to 2. The first, called group A, includes Catterall groups I and II; for patients in this group, less than 50% of the head is involved. The second, called group B, includes Catterall groups III and IV; for patients in this group, more than 50% of the head is involved. For both classifications, if less than 50% of the ball is involved, the prognosis is better, whereas if more than 50% is involved, the prognosis is potentially poor. [22]
The Herring classification addresses the integrity of the lateral pillar of the head. In lateral pillar group A, there is no loss of height in the lateral one third of the head, and there is little density change. In lateral pillar group B, there is a lucency and less than 50% loss of lateral height. Sometimes, the head is beginning to extrude from the socket. In lateral pillar group C, there is a more than 50% loss of lateral height. [21, 22]
Reported limitations of the Herring classification include difficulties in reliably classifying hips in the initial stage and the difficulty of classification in bilateral cases, since there is a lack of reference height with which to compare. [22]
In a subsequent review of the original study, Herring et al identified a group of hips with radiographic findings that were more severe than those typical of group B but less severe than those seen in group C. A new group, termed B/C borderline, was added to the classification system. However, the introduction of the borderline B/C group has not been found to increase the interobserver agreement or prognostic value of the original Herring classification. [22]
Radiography
Plain radiographs have a sensitivity of 97% and a specificity of 78% in the detection of LCPD. Severe osteoarthritis and infective arthritis may mimic the disease.
Early radiographic signs of LCPD include the following [23] :
-
Small femoral epiphysis (96%)
-
Sclerosis of the femoral head with sequestration and collapse (82%)
-
Slight widening of the joint space caused by thickening of the cartilage, failure of epiphyseal growth, the presence of joint fluid, or joint laxity (60%) (see the images below)
 Legg-Calvé-Perthes disease. Stage II disease. Note the slight widening of the left hip joint, representing a small joint effusion. Joint widening can also be secondary to hypertrophy of the cartilage.
Legg-Calvé-Perthes disease. Stage II disease. Note the slight widening of the left hip joint, representing a small joint effusion. Joint widening can also be secondary to hypertrophy of the cartilage.
 Legg-Calvé-Perthes disease. Stage II disease. Note the slight widening of the left hip joint representing a small joint effusion. Joint widening can also be secondary to hypertrophy of the cartilage.
Legg-Calvé-Perthes disease. Stage II disease. Note the slight widening of the left hip joint representing a small joint effusion. Joint widening can also be secondary to hypertrophy of the cartilage.
 Legg-Calvé-Perthes disease. The left joint effusion is apparent. The femoral head is smaller on the left than the right. The femoral head is also considerably denser on the left side. Joint widening can also be secondary to hypertrophy of the cartilage.
Legg-Calvé-Perthes disease. The left joint effusion is apparent. The femoral head is smaller on the left than the right. The femoral head is also considerably denser on the left side. Joint widening can also be secondary to hypertrophy of the cartilage.
 Legg-Calvé-Perthes disease. The left joint effusion is apparent. The femoral head is smaller on the left than on the right. The femoral head is also considerably denser on the left side. Joint widening can also be secondary to hypertrophy of the cartilage.
Legg-Calvé-Perthes disease. The left joint effusion is apparent. The femoral head is smaller on the left than on the right. The femoral head is also considerably denser on the left side. Joint widening can also be secondary to hypertrophy of the cartilage.
-
An absence of destruction of the articular cortex, as occurs in bacterial arthritis (destruction of articular cartilage never occurs in LCPD)



Late signs of LCPD on radiographs include the following:
-
Delayed osseous maturation of a mild degree, a radiolucent crescent line representing a subchondral fracture
-
Femoral head fragmentation and femoral neck cysts from intramedullary hemorrhage or extension of physeal cartilage into metaphysis, loose bodies, and coxa plana (see the images below)
 Legg-Calvé-Perthes disease. Image shows flattening and early fragmentation of the left femoral head with the presence of femoral neck cysts. The femoral head is obviously smaller on the left than on the right.
Legg-Calvé-Perthes disease. Image shows flattening and early fragmentation of the left femoral head with the presence of femoral neck cysts. The femoral head is obviously smaller on the left than on the right.
 Legg-Calvé-Perthes disease. Image shows flattening and early fragmentation of the left femoral head with the presence of femoral neck cysts. The femoral head is obviously smaller on the left than on the right.
Legg-Calvé-Perthes disease. Image shows flattening and early fragmentation of the left femoral head with the presence of femoral neck cysts. The femoral head is obviously smaller on the left than on the right.
 Legg-Calvé-Perthes disease. Image shows flattening and early fragmentation of the left femoral head with the presence of femoral neck cysts. The femoral head is obviously smaller on the left than on the right.
Legg-Calvé-Perthes disease. Image shows flattening and early fragmentation of the left femoral head with the presence of femoral neck cysts. The femoral head is obviously smaller on the left than on the right.
-
Coxa magna, or remodeling of the femoral head, which becomes wider and flatter, similar in appearance to a mushroom (see the image below)
 Legg-Calvé-Perthes disease. Plain radiograph in an adult patient with residual coxa magna and plana deformity with superimposed joint changes.
Legg-Calvé-Perthes disease. Plain radiograph in an adult patient with residual coxa magna and plana deformity with superimposed joint changes.



An uncommon radiologic finding of sclerosis and severe collapse of the entire femoral epiphysis resembling a discus has been reported in 32 children. [24]
Computed Tomography
Early signs of LCPD on CT scans include the following:
-
Bone collapse
-
Curvilinear zones of sclerosis
-
Subtle changes in bone trabecular pattern
-
Disruption of an area of condensation of bone formed by a compressive group of trabeculae (abnormal asterisk sign)
Late signs of the disease on CT scans include the following:
-
Central or peripheral areas of decreased attenuation
-
Intraosseous cysts
Coronal reconstructions can show subchondral fractures, subtle buckling, or collapse of the articular surface.
When CT scanning is employed, the staging of LCPD determined on the basis of plain radiographic findings is upgraded in 30% of patients. CT scanning is not as sensitive as nuclear medicine or MRI, but it may be used for follow-up imaging in patients with LCPD. CT scan findings of osteoarthritis and infective arthritis may mimic those of LCPD.
Magnetic Resonance Imaging
Early in the course of Legg-Calve-Perthes disease, irregular foci of low signal intensity or linear segments replace the normal high signal intensity of bone marrow in the femoral epiphysis on T1- and T2-weighted images. Other findings include an intra-articular effusion and a small, laterally displaced ossification nucleus, labral inversion, and femoral head deformity. The differential diagnosis includes severe osteoarthritis, infective arthritis, and other causes of bone marrow edema and joint effusions. MRI is as sensitive as isotopic bone scanning, and it allows more precise localization of involvement than does conventional radiography. MRI is preferred for evaluating the position, form, and size of the femoral head and surrounding soft tissues. [18, 19, 20, 23, 25, 26, 27]
A preliminary study of diffusion MRI of the neck of the femur in 27 children found that the estimation of apparent diffusion coefficient (ADC) of the neck of the femur in Legg-Calve-Perthes disease is a useful parameter and could be useful in the treatment of LCPD. [28] The study revealed an early and significant increase in the ADC on the pathologic side. This increase could have prognostic value, as it is correlated with the Catterall classification.
(The MRI characteristics of Legg-Calve-Perthes disease are demonstrated in the images below.)
 Legg-Calvé-Perthes disease. Coronal T2-weighted MRIs show irregularity and flattening of cortical margins of the left femoral epiphysis. Also note a mild joint effusion and subluxation and hinge deformity of the left femoral head.
Legg-Calvé-Perthes disease. Coronal T2-weighted MRIs show irregularity and flattening of cortical margins of the left femoral epiphysis. Also note a mild joint effusion and subluxation and hinge deformity of the left femoral head.
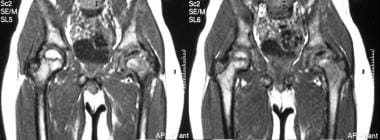 Legg-Calvé-Perthes disease. Coronal T1-weighted MRIs show the loss of normal high signal intensity in the left femoral epiphysis, which now has low signal intensity.
Legg-Calvé-Perthes disease. Coronal T1-weighted MRIs show the loss of normal high signal intensity in the left femoral epiphysis, which now has low signal intensity.
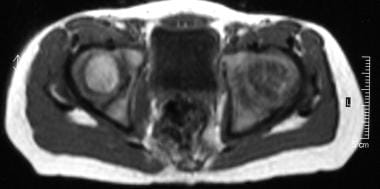 Legg-Calvé-Perthes disease. Axial T1-weighted MRIs through the femoral heads show low signal intensity in the left femoral head.
Legg-Calvé-Perthes disease. Axial T1-weighted MRIs through the femoral heads show low signal intensity in the left femoral head.
Fat-suppressed or short-tau inversion recovery (STIR) sequences are more accurate than plain radiographs in showing degenerative changes of the articular cartilage. These MRIs demonstrate the influx of fluid into areas of articular cartilage irregularity.
The asterisk sign is defined as findings of areas of low signal intensity on T1-weighted images and high signal intensity on T2-weighted images in marrow. The double-line sign occurs in as many as 80% of patients and represents the sclerotic rim, which appears as a signal void. This sign is demonstrated as a line between necrotic and viable bone edges, with a hyperintense rim of granulation tissue.
Jaramillo et al found in a study that multipositional MRI with an open magnet was comparable to arthrography for demonstrating containment of the congruency of the articular surfaces of the hip. [15] However, in the evaluation of deformity or loss of the spherical nature of the femoral head, open MRI performed less well.
Sebag et al showed dynamic gadolinium-enhanced subtraction MRI to be a simple and promising means of early recognition of ischemia in LCPD. [16]
Gadolinium-based contrast agents have been linked to the development of nephrogenic systemic fibrosis (NSF) or nephrogenic fibrosing dermopathy (NFD). The disease has occurred in patients with moderate to end-stage renal disease after being given a gadolinium-based contrast agent to enhance MRI or MRA scans. NSF/NFD is a debilitating and sometimes fatal disease. Characteristics include red or dark patches on the skin; burning, itching, swelling, hardening, and tightening of the skin; yellow spots on the whites of the eyes; joint stiffness with trouble moving or straightening the arms, hands, legs, or feet; pain deep in the hip bones or ribs; and muscle weakness.
In addition, the FDA is requiring a class warning and other safety measures for all gadolinium-based contrast agents (GBCAs) concerning gadolinium remaining in patients’ bodies, including the brain, for months to years after receiving these drugs. [29]
Ultrasonography
Although not performed routinely, ultrasonographic evaluation of patients with Legg-Calve-Perthes disease is a simple and standardized procedure that can be useful for staging the disease and monitoring its course. It can also spare the patient from radiation exposure and lower treatment costs. Lateral extrusion and the onset of healing in patients with LCPD can be shown earlier with sonograms than with radiographs.
Ultrasonography is useful in establishing the diagnosis of transient synovitis of the hip and the onset of LCPD. Hip effusion, which results in capsular distention, is accurately documented on sonograms. (Capsular distention lasting longer than 6 weeks is associated with LCPD.) Ultrasonography allows aspiration of joint fluid for laboratory examination. Together, the results of clinical evaluation, radiography, and sonography determine the need for sonography-guided aspiration. Ultrasonography-guided aspiration allows the selection of only those patients with septic arthritis for surgical drainage and shortens the procedure. Negative sonographic findings allow the exclusion of septic arthritis but not osteomyelitis.
A chronologic, 4-part staging of LCPD has been proposed on the basis of the ultrasonographic findings. The stages reflect the degree of flattening and fragmentation and the reconstitution of the femoral head. Thickening of articular cartilage, associated synovitis, and lateral extrusion of the femoral head can be documented. Joint effusion is present in 74% of patients in stages I-II. Lateral extrusion increases from stage II onward until the healing stage. [10, 11, 12, 13, 14, 30]
Hip ultrasonography seems to be a reliable method for monitoring the containment of the femoral head in LCPD. [31] Changes similar to those of LCPD can be found in transient synovitis and other conditions that cause hip joint effusions. Moreover, joint effusion is not always present in patients with LCPD.
Nuclear Imaging
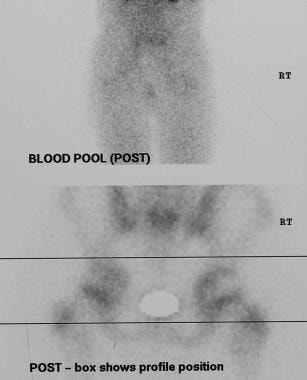
Technetium-99m diphosphonate uptake depends on the stage of the disease, but it does play a role in the diagnosis. Characteristic features include a photopenic void in proximal femoral epiphyses (seen in the first 2 images below), as compared to the contralateral side, which usually can be seen by using a pinhole camera with the hip in maximal medial rotation, obviating the need of single-photon emission CT (SPECT).
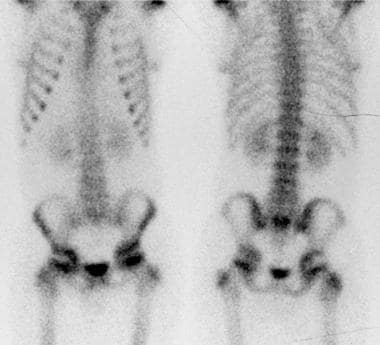 Legg-Calvé-Perthes disease. Technetium-99m diphosphonate bone scan shows a photon-deficient defect in the right femoral head.
Legg-Calvé-Perthes disease. Technetium-99m diphosphonate bone scan shows a photon-deficient defect in the right femoral head.
 Legg-Calvé-Perthes disease. Zoomed images of the same patient as in the previous image show the photopenic defect more clearly.
Legg-Calvé-Perthes disease. Zoomed images of the same patient as in the previous image show the photopenic defect more clearly.
 Legg-Calvé-Perthes disease. Radiograph obtained at the same time as the radionuclide scans in the previous 2 images illustrates the usefulness of isotope bone scans. The radiographic changes of subchondral lucency are subtle.
Legg-Calvé-Perthes disease. Radiograph obtained at the same time as the radionuclide scans in the previous 2 images illustrates the usefulness of isotope bone scans. The radiographic changes of subchondral lucency are subtle.
Scintigraphy may be helpful in early diagnosis. Initially, uptake is decreased in the femoral head because of an interruption in the blood supply. Later, uptake is increased in the femoral head as a result of revascularization, bone repair, and degenerative osteoarthritis. In addition, acetabular activity can be increased with associated joint disease.
The sensitivity of radionuclide scanning in the diagnosis of LCPD is 98%, and the specificity is 95%. Similar activity patterns may occur with osteoarthritis or infective or inflammatory arthritis. The presence of a large joint effusion can simulate diminished perfusion caused by osteonecrosis.
Angiography
Angiography is performed only in rare cases. Early in the disease process, opacification of the joint with contrast material can reveal subtle flattening of the chondral surface of the femoral head and widening of the joint space.
Angiographic findings may demonstrate an interruption in the superior capsular arteries and a generalized decrease of blood flow in the affected hip. Later in the disease process, the size and position of sequestered fragments can be identified by the distribution of revascularized osseous segments despite the demonstration of a smooth cartilaginous surface. However, vascular changes in LCPD are nonspecific on angiograms.
-
Legg-Calvé-Perthes disease. Stage II disease. Note the slight widening of the left hip joint, representing a small joint effusion. Joint widening can also be secondary to hypertrophy of the cartilage.
-
Legg-Calvé-Perthes disease. Stage II disease. Note the slight widening of the left hip joint representing a small joint effusion. Joint widening can also be secondary to hypertrophy of the cartilage.
-
Legg-Calvé-Perthes disease. The left joint effusion is apparent. The femoral head is smaller on the left than the right. The femoral head is also considerably denser on the left side. Joint widening can also be secondary to hypertrophy of the cartilage.
-
Legg-Calvé-Perthes disease. The left joint effusion is apparent. The femoral head is smaller on the left than on the right. The femoral head is also considerably denser on the left side. Joint widening can also be secondary to hypertrophy of the cartilage.
-
Legg-Calvé-Perthes disease. Image shows subchondral sclerosis and radiolucency in the left femoral head (stage II disease). The femoral head is slightly smaller on the left than the right.
-
Legg-Calvé-Perthes disease. The left subchondral radiolucency is more readily demonstrated on a frog-leg view and represents subchondral fracture.
-
Legg-Calvé-Perthes disease. Image shows left femoral subchondral sclerosis and radiolucency.
-
Legg-Calvé-Perthes disease. Image shows left femoral subchondral sclerosis and radiolucency.
-
Legg-Calvé-Perthes disease. Image shows flattening and early fragmentation of the left femoral head with the presence of femoral neck cysts. The femoral head is obviously smaller on the left than on the right.
-
Legg-Calvé-Perthes disease. Image shows flattening and early fragmentation of the left femoral head with the presence of femoral neck cysts. The femoral head is obviously smaller on the left than on the right.
-
Legg-Calvé-Perthes disease. Image shows flattening and early fragmentation of the left femoral head with the presence of femoral neck cysts. The femoral head is obviously smaller on the left than on the right.
-
Legg-Calvé-Perthes disease. Image shows fragmentation of the left femoral head. Also note widening and shortening of the left femoral neck.
-
Legg-Calvé-Perthes disease. Image shows loss of structural integrity of the right femoral head. Also note lateral extrusion of the right femoral head.
-
Legg-Calvé-Perthes disease. Image shows loss of structural integrity of the left femoral head. Also note the widening and shortening of the femoral neck, and more importantly, the severe subluxation.
-
Legg-Calvé-Perthes disease. Plain radiograph in an adult patient with residual coxa magna and plana deformity with superimposed joint changes.
-
Legg-Calvé-Perthes disease. Axial nonenhanced CT scan through the hip joints in the same patient as in the previous image more clearly shows the loss of structural integrity of the right femoral head.
-
Legg-Calvé-Perthes disease. Nonenhanced axial CT section through the hip joints obtained at a different level in the same patient as in the previous 2 images. Once again, the scan shows the loss of structural integrity of the right femoral head. Note the acetabular subchondral sclerosis.
-
Legg-Calvé-Perthes disease. Coronal reconstruction shows flattening, sclerosis, and early fragmentation of the right femoral head (same patient as in the previous 3 images).
-
Legg-Calvé-Perthes disease. Coronal T2-weighted MRIs show irregularity and flattening of cortical margins of the left femoral epiphysis. Also note a mild joint effusion and subluxation and hinge deformity of the left femoral head.
-
Legg-Calvé-Perthes disease. Coronal T1-weighted MRIs show the loss of normal high signal intensity in the left femoral epiphysis, which now has low signal intensity.
-
Legg-Calvé-Perthes disease. Axial T1-weighted MRIs through the femoral heads show low signal intensity in the left femoral head.
-
Legg-Calvé-Perthes disease. Technetium-99m diphosphonate bone scan shows a photon-deficient defect in the right femoral head.
-
Legg-Calvé-Perthes disease. Zoomed images of the same patient as in the previous image show the photopenic defect more clearly.
-
Legg-Calvé-Perthes disease. Radiograph obtained at the same time as the radionuclide scans in the previous 2 images illustrates the usefulness of isotope bone scans. The radiographic changes of subchondral lucency are subtle.
-
Legg-Calvé-Perthes disease. Coronal T2-weighted MRI shows irregularity and flattening of cortical margins of the right femoral epiphysis and the loss of normal signal intensity. Also, note a mild effusion in the joint (same patient as in the previous 3 images).






