Practice Essentials
Le Fort fractures account for 10-20% of all facial fractures. They result from exposure to a considerable amount of force. Motor vehicle accidents (MVAs) are the predominant cause; other causes include assaults and falls. With seatbelt laws and the increased use of airbags by auto manufacturers, the overall incidence of midface fractures has decreased.
(See the images of Le Fort fractures below. )
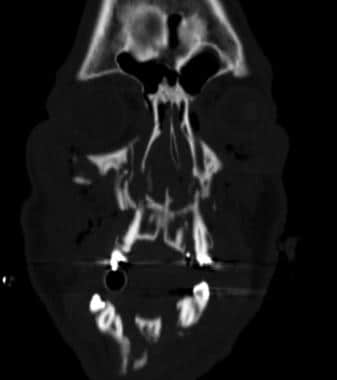 Coronal CT of a patient with right Le Fort III fracture and left Le Fort II fracture.
Coronal CT of a patient with right Le Fort III fracture and left Le Fort II fracture.
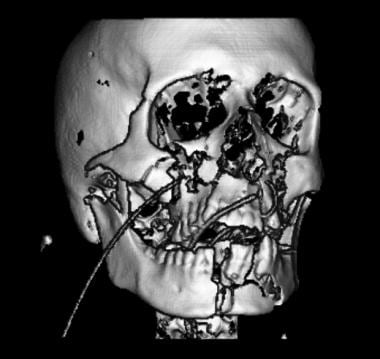
 Three-dimensional reconstruction of a patient with right Le Fort I fracture and a left Le Fort II fracture.
Three-dimensional reconstruction of a patient with right Le Fort I fracture and a left Le Fort II fracture.
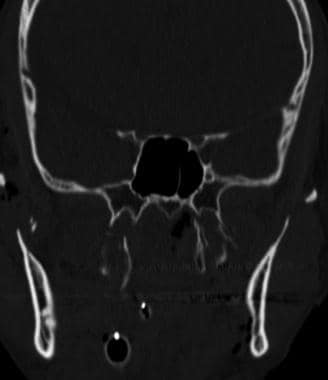
 Coronal CT demonstrating a right Le Fort I fracture and a left Le Fort II fracture.
Coronal CT demonstrating a right Le Fort I fracture and a left Le Fort II fracture.
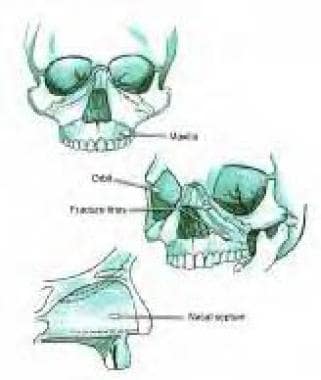
Le Fort classification system
Rene Le Fort described the classic patterns of fracture in his 1901 work. Le Fort's experiments consisted of dropping cadaver skulls from several stories or striking them with a wooden club. He found 3 distinct fracture patterns, which he termed the linea minoros resistentiae. Simply stated, in the Le Fort I fracture, the palate is separated from the maxilla; in the Le Fort II fracture, the maxilla separates from the face; and in the Le Fort III fracture, craniofacial dysjunction is present.
The Le Fort I fracture is a low transverse fracture that crosses the floor of the nose, pyriform aperture, canine fossa, and lateral wall from the maxilla, resulting in separation of the palate from the maxilla. These fractures are associated with malocclusion and dental fractures. [1]
The Le Fort II fracture crosses the nasal bones on the ascending process of the maxilla and lacrimal bone and crosses the orbital rim. The Le Fort II fracture extends posteriorly to the pterygoid plates at the base of the skull. A Le Fort I fracture is characterized by a low septal fracture, whereas a Le Fort II fracture results in a high septal fracture.
Only the Le Fort II fracture violates the orbital rim. Because of this proximity to the infraorbital foramen, type II fractures are associated with the highest incidence of infraorbital nerve hypesthesias. Involvement of the orbit may lead to the development of complications including extra-ocular muscle injury, orbital hematoma, globe rupture or impingement, and optic nerve damage. Furthermore, damage to the medial maxillary buttress has been associated with epistaxis, cerebral spinal fluid (CSF) rhinorrhea, lacrimal duct and sac injury, medial canthal tendon injury, and sinus drainage obstruction. [1]
Finally, the Le Fort III fracture traverses the frontal process of the maxilla, the lacrimal bone, the lamina papyracea, and the orbital floor. This fracture often involves the posterior plate of the ethmoid. Because of their location, Le Fort III fractures are associated with the highest rate of CSF leaks. [2, 3]
Shortcomings of the Le Fort classification system
Despite its shortcomings, the Le Fort fracture classification system is still the most accepted method of classifying fractures and the location of osteotomies of the midface. However, studies have demonstrated that this classification system may be imprecise. The initial classification was based on injury patterns caused by low-velocity and low-energy inciting events; however, now, LeFort fractures are predominantly caused by motor vehicle accidents or other high-energy collisions. They can be unilateral or bilateral, symmetrical or asymmetrical, and are often concomitant with other facial fractures. Often, fractures extend through the maxillary sinus, as well as the medial and lateral buttresses. [4]
In addition, most midface fractures have some degree of comminution and are complicated by fractures and displacement not addressed in the Le Fort system. These midface fractures include palate, medial maxillary arch, dentoalveolar, and anterior maxillary fractures.
Other classification systems
Palatal injuries continue to be found primarily in conjunction with midfacial or panfacial fractures and rarely occur in isolation. They are not classified in typical Le Fort fracture terminology. However, Le Fort did describe traumatic injuries to the palate in his paper on maxillary fractures. The incidence of palatal fracture in patients with Le Fort fractures ranges in reports from 8-13%. [5]
Palatal fractures were classified by Hendrickson et al, who described 6 types of palatal fractures, including the following: I, anterior and posterolateral alveolar; II, sagittal; III, parasagittal; IV, para-alveolar; V, complex; and VI, transverse. Palatal fractures are associated with Le Fort I fractures 100% of the time and with either Le Fort II/III or mandible fractures 50% of the time.
There are many other classification systems for describing midface fractures. In the system of Donat et al, the face is divided into a matrix of vertical and horizontal beams, creating a lattice of 11 unilateral and 22 bilateral sites; this lattice is used to describe midface fractures. [6] According to their preliminary data in 87 patients with midface fractures, this scheme enabled accurate transcription and communication among physicians 98% of the time.
Another classification system is the Wassmund system. This system classifies fractures into grades I-V. A Wassmund I fracture is equivalent to a Le Fort II fracture. A Wassmund IV fracture is equivalent to a Le Fort III fracture. A Wassmund III fracture is characterized as a Le Fort III fracture without inclusion of the nasal bones.
Manson described a facial fracture classification system on the basis of CT findings. [7] He divided fractures into low- and high-impact fractures.
Preferred examination
Radiologic features that should trigger further evaluation for Le Fort fractures include the presence of a pterygoid fracture, which is found in all Le Fort fractures types. Other signs include fractures of the lateral nasal wall, inferior orbital rim, lateral orbital wall, and the zygomatic arch. [1]
The preferred radiologic examination is CT scanning of the facial bones, with coronal and axial sections in bone windows for maximal detail. Midface fractures are best evaluated with CT imaging. [8, 9] Plain radiography and MRI play more limited roles in the evaluation of midfacial fractures. CT is not as suitable as MRI for assessing soft tissue changes and acute intracranial changes. Hardware and dental fillings can cause a scatter effect, making interpretation of fracture difficult in certain circumstances.
Previously, an adequate examination of the cribriform plate, orbital roof, and orbital floor required images in the coronal plane, necessitating a direct coronal CT scan. However, to acquire a direct coronal CT scan, the cervical spine had to be cleared, and this could wast valuable time. Obtaining a direct coronal CT scan also increased costs, increased patient exposure to ionizing radiation, and required transport of a potentially unstable patient to the scanner itself.
Patients with facial fractures should be evaluated for potential cervical spine and head injuries. Le Fort fractures have been associated with spinal fracture or dislocation (1.4%) and cervical cord injury (1%). Higher-grade Le Fort fractures (types II and III) have been associated with a 2.88-fold and 2.54-fold increased risk of concomitant intracranial injuries, respectively. [1]
Blunt facial trauma has been found to be associated with internal carotid artery injuries in 1.2% of cases; specifically, internal carotid artery injuries have been found in 6.9%, 5.6%, and 3.0% of patients with Le Fort I, II, and III fractures, respectively. [10]
Angiography may be needed if there is concern about an associated injury to the carotid artery or internal maxillary artery (eg, to identify the site of arterial bleeding before embolization).
For additional information about Le Fort fractures, see Maxillary and Le Fort Fractures.
Radiography
Plain radiographs are usually not ordered in complex trauma cases. The applicable plain images include facial bone series, which typically includes Waters, Stevens, and Townsend views.
Plain radiographs have largely been replaced by CT scans for examining the midface. If there is concern about the possibility of a midface fracture, a CT scan is warranted.
Panorex views are the best images for showing the orthognathic relationship and occlusion. A Panorex view is especially helpful when associated mandible fractures are present.
Computed Tomography
When diagnosing Le Fort fractures, 2-D CT imaging is preferable to 3-D CT because it provides increased detail of fracture lines and associated soft tissue injuries. 3-D CT is capable of identifying Le Fort fractures that are not obvious on single 2-D cuts and may be helpful for surgical planning. Multidetector CT (MDCT) is considered the imaging modality of choice because it produces high-resolution images and also allows for 3-D rendering. This facilitates identification of small fracture lines and differentiation of soft tissue and bone injury. [1]
When imaging for Le Fort fractures, it is important to analyze the whole face for fractures, including the entire mandible, because of the high rate of fracture of the upper and lower face when midface fractures occur. The CT scan is analyzed in bone windows; 2- to 3-mm sections are preferred. A single-plane CT scan does not provide as much information as a 2-plane CT scan. It is crucial to use a systematic analysis in analyzing midface fracture CT scans.
Axial sections are best for analyzing the posterior wall of the antrum, the pterygoid plates, the hard palate, dentoalveolar segments, the zygomatic arch and body, and the lateral wall of the orbit. Coronal sections provide the best images for analyzing the anterior wall of the maxilla, the inferior orbital rim, the palate, and the orbital floor.
Reformatted CT images are also of high quality and have been shown to be reliable and accurate in surgical reconstructive efforts.
With the introduction of helical CT, which acquires data in a continuous fashion, it is now possible to produce computer-reformatted images, either coronal or sagittal, from the standard axial images. Coronal images reformatted from helically acquired thin-section axial CT data have been shown to have high sensitivity and specificity in the detection of fractures, as compared with direct coronal imaging.
(See the Le Fort images below.)
Coronal CT of a patient with right Le Fort III fracture and left Le Fort II fracture.
Coronal CT demonstrating a right Le Fort I fracture and a left Le Fort II fracture.
Three-dimensional (3D) reconstructions (see the images below) are usually not necessary in analyzing midface fractures. However, these reconstructions may be useful in highly complex fractures or secondary reconstructions and in facilitating communication between the radiologist and the surgeon. [11, 12] Cavalanti et al have shown that 3D construction is quantitatively accurate for surgical planning and evaluation.
 Three-dimensional reconstruction of a patient with a right Le Fort III fracture and left Le Fort II fracture.
Three-dimensional reconstruction of a patient with right Le Fort I fracture and a left Le Fort II fracture.
Three-dimensional reconstruction of a patient with a right Le Fort III fracture and left Le Fort II fracture.
Three-dimensional reconstruction of a patient with right Le Fort I fracture and a left Le Fort II fracture.
Interpretation
Manson described a classification system in which fractures were classified as resulting from low-, middle-, or high-energy mechanisms; the determination of whether a fracture was the result of a log-, middle-, or high-energy mechanism was made on the basis of the degree of segmentation and displacement seen on CT scans. [13]
In Manson's system, fractures are classified according to the displacement and the degree of comminution. In type I fractures, there is minimal displacement and no comminution. In type II fractures, there is moderate displacement and a small amount of comminution. In type III fractures, there is severe displacement, with the major buttresses comminuted in multiple locations. This system may serve as a dependable guide for determining the prognosis and proper intervention.
In making the radiologic report, it is important that damage to adjacent structures, such as the nasolacrimal duct, mandible, zygoma, and orbit, be commented upon. The degree of displacement and the degree of comminution may affect the surgical approach. The presence of any hardware may signify previous traumatic injury and repair. [14, 15, 16]
Accuracy
CT scanning is the criterion standard for detecting facial fractures. It is superior to clinical examination, and it is more than 95% accurate.
Sagittal reformatted helical CT scans are comparable in quality to direct sagittal scans.
CT scanning of a facial bone results in few false-positive or false-negative results.
Koltai et al applied Manson's energy classification with CT scanning in children and found that CT is an effective way of determining the severity of fracture. The more severe the fracture, the more likely a repair is necessary.
Misinterpretation of facial suture lines can cause an inexperienced examiner to diagnose facial fractures when none is present.
Magnetic Resonance Imaging
MRI is typically performed 48 hours after trauma. The signal intensity of blood on T1-weighted images varies, depending on the age and location of the blood.
With regard to imaging the midface, the incidence of false-negative results are high with MRI, as compared with CT. Generally, a radiologist has a low degree of confidence in MRI findings when assessing a facial fracture; MRI plays an adjunctive role in the examination.
MRIs are typically not helpful in cases involving acute bony trauma to the face, but if there is a question of soft-tissue injury to nervous structures, MRI may be helpful.
MRI does have a role in cases involving intracranial injury or in cases in which unusual soft-tissue injury may be present.
MRI is superior in the evaluation of brain and dural-space injury.
-
Le Fort fractures.
-
Three-dimensional reconstruction of a patient with a right Le Fort III fracture and left Le Fort II fracture.
-
Coronal CT of a patient with right Le Fort III fracture and left Le Fort II fracture.
-
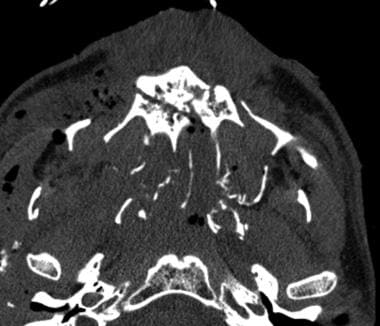
Bilateral pterygoid fractures.
-
Axial picture. Note bilateral pterygoid plate fractures.
-
Three-dimensional reconstruction of a patient with right Le Fort I fracture and a left Le Fort II fracture.
-
Coronal CT demonstrating a right Le Fort I fracture and a left Le Fort II fracture.









