Practice Essentials
Laryngeal cancer is the most common cancer of the upper aerodigestive tract. Squamous cell carcinoma (SCC) is the most common malignant tumor of the larynx and accounts for approximately 95% of all cases of laryngeal carcinoma. [1] According to the SEER (Surveillance, Epidemiology, and End Results Program) Cancer Statistics Review of the National Cancer Institute, an estimated 12,370 men and women in the United States will have been diagnosed with laryngeal squamous cell carcinoma in 2020. [2] Cervical lymph node metastasis is the main mechanism of spread of SCC. Knowledge of nodal drainage patterns helps in correctly characterizing enlarged nodes and accurately evaluating most likely sites of metastasis. The cervical nodes are divided into 6 levels on the basis of primary lymphatic drainage of each cervical tumor. The supraglottis drains primarily into the upper jugular lymph nodes, and the glottis and subglottis have sparse lymphatic drainage. [3]
The incidence of laryngeal tumors is closely correlated with smoking, as head and neck tumors occur 6 times more often in cigarette smokers than in nonsmokers. The age-standardized risk of mortality from laryngeal cancer appears to have a linear relationship with increasing cigarette consumption. Death from laryngeal cancer is 20 times more likely for the heaviest smokers than for nonsmokers. [4]
Furthermore, active smoking by patients with head and neck cancer is associated with significant increases in the annual rate of second primary tumor development compared to former smokers or nonsmokers. The use of unfiltered cigarettes or dark, air-cured tobacco is associated with further increases in risk.
Although alcohol is a less potent carcinogen than tobacco, alcohol consumption is a risk factor for laryngeal tumors. In individuals who use both tobacco and alcohol, these risk factors appear to be synergistic, and they result in a multiplicative increase in the risk of developing laryngeal cancer.
Host, tumor, and treatment factors all have an important impact on prognosis in patients who have laryngeal squamous cell carcinoma; staging systems only take into account tumor factors. [4]
Imaging modalities
Radiologic evaluation of the larynx usually starts with CT because of short scanning time, excellent anatomic resolution, and wide availability. MRI is reserved for cases in which CT is not conclusive. Because of excellent soft-tissue resolution, MRI is more accurate than CT in delineating deep tumor extension and cartilage involvement. [3]
Cross-sectional imaging with CT and/or MRI or of the head and neck is necessary to delineate the extent of primary disease, the presence of bone or cartilage invasion, and the presence of nodal disease. Imaging is particularly useful for submucosal regions such as the pre-epiglottic space and subglottis. Although some authors claim that MRI provides a more accurate depiction of tumor extent, most institutions continue to use CT as the primary cross-sectional modality. Advances in high-resolution multi-channel helical CT have kept CT competitive with MRI. MRI is more sensitive, but less specific, than CT for the diagnosis of cartilage invasion. [5, 6, 7, 8, 9, 10, 11, 12, 13, 14]
T1 tumors of the glottis may not require imaging, though CT is often used to exclude nodal metastases. Plain chest radiography or chest CT may be used to rule out pulmonary metastasis.
The information sought at imaging depends on the size and position of the primary tumor and the type of therapy planned. A small tumor without evidence of deep extension does not require imaging because all information needed for the therapeutic decision may be obvious at endoscopy.
Treatment options include cord stripping, laser excision, or radiation therapy. [15] Alternatively, the lesion may be so large that a total laryngectomy is the only option considered; thus, imaging of the primary lesion is of limited usefulness. [16, 17]
For intermediate-sized lesions, imaging can provide useful information. Radiation therapy remains an option. If surgery is considered, a decision must be made as to whether a patient is a candidate for a voice-sparing partial laryngectomy or whether total laryngectomy is required. [16, 17]
Supraglottic carcinomas are associated with a high incidence of nodal metastases at diagnosis; therefore, complete evaluation of the internal jugular lymph nodes with imaging studies is needed. The reported incidence of clinically positive lymph nodes is 55% at initial diagnosis, with a 16% incidence of bilateral involvement.
Petragalla et al evaluated 40 patients for thyroid, arytenoid, and cricoid cartilage invasion on CT imaging who had undergone total laryngectomy for both primary and recurrent laryngeal carcinoma. CT erosion showed 100% agreement for thyroid inner cortex and cricoid cartilage invasion and 87% for arytenoid cartilage invasion. For primary tumors, CT demonstrated good (inner cortex 75%; full-thickness 85%), substantial (67.5%), and perfect (100%) accuracy in thyroid, arytenoid, and cricoid cartilage invasion, respectively. [12]
Slevin et al confirmed that response-assessment FDG PET-CT after radiotherapy, with or without chemotherapy, for laryngeal and hypopharyngeal carcinomas has a high negative predictive value for both primary sites and lymph node sites and can therefore be used to guide treatment decisions. In 35 patients, sensitivity, specificity, positive predictive value, and negative predictive value for response-assessment FDG PET-CT for primary sites, respectively, were 100%, 73%, 46%, and 100%; and for nodal sites, 83%, 95%, 83%, and 95%. [18]
In a study by Hu et al, CEUS, compared with conventional ultrasound and contrast-enhanced CT, showed a reliable initial T-staging accuracy and diagnostic properties for detecting laryngeal cartilage invasion. Of 41 patients with laryngeal carcinoma who underwent conventional high-frequency ultrasound, contrast-enhanced US, and contrast-enhanced CT before surgery, CEUS showed hyperenhancement in 38 cases and isoenhancement in 3 cases. [19]
(See the images below.)

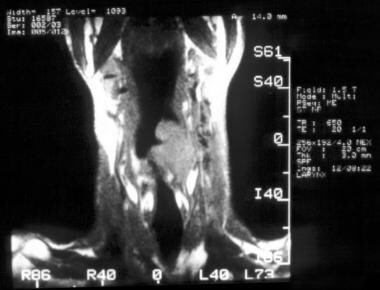 MR imaging, larynx. Sagittal T1-weighted MRI of the larynx in a patient with squamous cell carcinoma. Note extension into the supraglottis.
MR imaging, larynx. Sagittal T1-weighted MRI of the larynx in a patient with squamous cell carcinoma. Note extension into the supraglottis.
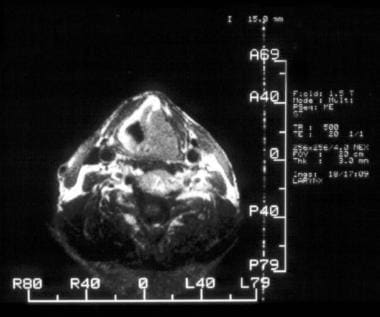 MR imaging, larynx. Axial T1-weighted MRI of a patient with squamous cell carcinoma of the larynx. The tumor has invaded the thyroid cartilage.
MR imaging, larynx. Axial T1-weighted MRI of a patient with squamous cell carcinoma of the larynx. The tumor has invaded the thyroid cartilage.
Anatomy
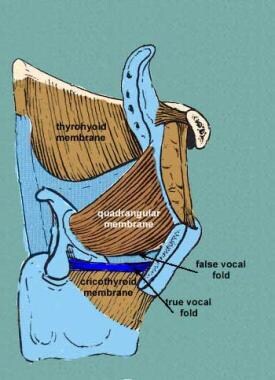
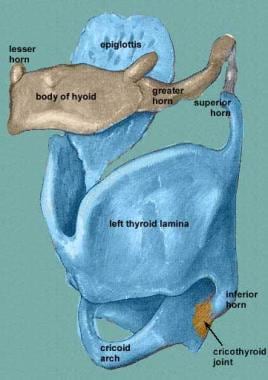
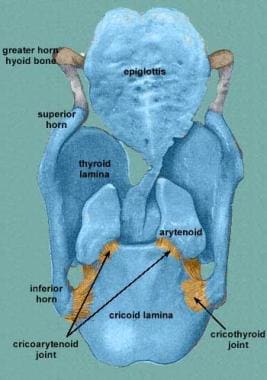
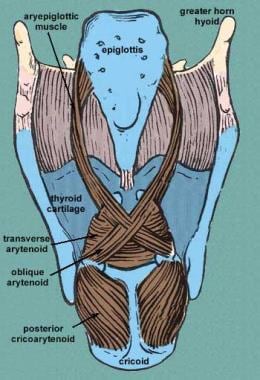
The larynx is divided into 3 anatomic regions: the supraglottic larynx, the glottis, and the subglottic region. The cartilaginous framework of the larynx includes the thyroid cartilage, cricoid cartilage, arytenoid cartilage, and corniculate cartilage, as shown in the images below.
 Lateral radiograph of the neck showing the different structures of the larynx: a, vallecula; b, hyoid bone; c, epiglottis; d, pre-epiglottic space; e, ventricle (air-space between false and true cords); f, arytenoid; g, cricoid; and h, thyroid cartilage.
Lateral radiograph of the neck showing the different structures of the larynx: a, vallecula; b, hyoid bone; c, epiglottis; d, pre-epiglottic space; e, ventricle (air-space between false and true cords); f, arytenoid; g, cricoid; and h, thyroid cartilage.
The pre-epiglottic fat is located in the anterior and lateral aspects of the larynx and is often invaded by advanced cancers. The anatomic borders are as follows: superior, hyoid bone and hyoepiglottic ligament; inferior, conus elasticus; anterior, thyrohyoid membrane; posterior, anterior wall of the pyriform sinus; and lateral, thyroid cartilage wall. Invasion of the pre-epiglottic fat has significant surgical implications, so evaluation of this space should be part of any radiologic analysis.
The recurrent laryngeal nerve innervates the intrinsic laryngeal muscles. Damage to this nerve causes hoarseness clinically and medialization of the arytenoid cartilage radiographically. Enlargement of the pyriform sinus is an important secondary sign of recurrent laryngeal nerve paralysis. The superior laryngeal nerve innervates the cricothyroid muscle, an extrinsic laryngeal muscle that tenses the true vocal cords. Damage to this nerve produces bowing of the vocal cord.
The anatomy of the cervical lymph nodes is relevant to the treatment of all laryngeal cancer. The American Joint Committee on Cancer (AJCC) and the American Academy of Otolaryngology–Head and Neck Surgery classification systems are widely used.
Radiologists use the hyoid bone as a marker for the carotid bifurcation, and the inferior cricoid cartilage as a marker for the omohyoid muscle, which may be difficult to discern radiographically. The Radiation Therapy Oncology Group, in collaboration with 2 European research groups, has established guidelines for delineation of nodal levels.
Staging system
The AJCC has designated staging by using the tumors, nodes, and metastases (TNM) classification. Definitions for the stages are described below. [20]
For primary tumors, TX indicates that the primary tumor cannot be assessed; T0 means there is no evidence of primary tumor; and Tis indicates carcinoma in situ.
In the supraglottis, the T stages are as follows:
-
T1, tumor limited to 1 subsite of the supraglottis with normal vocal cord mobility
-
T2, tumor invasion of the mucosa of more than 1 adjacent subsite of the supraglottis or glottis or of a region outside the supraglottis (eg, mucosa of base of tongue, vallecula, medial wall of pyriform sinus), without fixation of the larynx
-
T3, tumor limited to the larynx with vocal cord fixation and/or invasion of any of the postcricoid area or pre-epiglottic tissues
-
T4a, moderately advanced local disease; tumor invasion through the thyroid cartilage and/or other tissues beyond the larynx
-
T4b, very advanced local disease; tumor invades prevertebral space, encases carotid artery or invades mediastinal structures
In the glottis, the T stages are as follows:
-
T1, tumor limited to the vocal cord (may involve anterior or posterior commissure) with normal mobility
-
Stage T1 can be subdivided into T1a, in which the tumor is limited to 1 vocal cord and T1b, in which the tumor involves both vocal cords
-
T2, tumor extension to the supraglottis and/or subglottis and/or impaired vocal cord mobility
-
T3, tumor limited to the larynx with vocal cord fixation
-
T4a, moderately advanced local disease; tumor invasion through the thyroid cartilage and/or other tissues beyond the larynx
-
T4b, very advanced local disease; tumor invades prevertebral space, encases carotid artery or invades mediastinal structures
In the subglottis, the T stages are as follows:
-
T1, tumor limited to the subglottis
-
T2, tumor extension to a vocal cord with normal or impaired mobility
-
T3, tumor limited to the larynx with vocal cord fixation
-
T4a, moderately advanced local disease; tumor invasion through cricoid or thyroid cartilage and/or extension to other tissues beyond the larynx
-
T4b, very advanced local disease; tumor invades prevertebral space, encases carotid artery or invades mediastinal structures
The N stages are as follows:
-
NX, regional lymph nodes cannot be assessed
-
N0, no regional lymph node metastasis
-
N1, metastasis in a single ipsilateral lymph node, 3 cm or less in greatest dimension
-
N2, metastasis in a single ipsilateral lymph node more than 3 cm but not more than 6 cm in greatest dimension, metastases in multiple ipsilateral lymph nodes with none more than 6 cm in greatest dimension, or metastases in bilateral or contralateral lymph nodes none more than 6 cm in greatest dimension
-
Stage N2 may be further subdivided as follows: N2a, metastasis in a single ipsilateral lymph node more than 3 cm but not more than 6 cm in greatest dimension; N2b, metastasis in multiple ipsilateral lymph nodes, none more than 6 cm in greatest dimension; and N2c, metastasis in bilateral or contralateral lymph nodes, none more than 6 cm in greatest dimension.
-
N3, metastasis in a lymph node more than 6 cm in greatest dimension
-
Stage N3 may be further subdivided as follows: N3a, metastasis in a lymph node more than 6 cm in greatest dimension with no extranodal extension (ENE-); N3b, metastasis in a lymph node more than 6 cm in greatest dimension with extranodal extension (ENE+);
M stages are as follows:
-
MX indicates that distant metastasis cannot be assessed
-
M0, no distant metastasis
-
M1, distant metastasis
Radiography
Soft tissue radiographs of the neck are good survey studies (see the image below). [7] Air is used as a natural contrast agent to visualize the lumen of the larynx and trachea. Retropharyngeal tissue thickness can be appreciated. Epiglottis and the aryepiglottic folds are visualized. However, radiography has no role in the current management of laryngeal cancer. The barium swallow is used to evaluate the pharyngeal wall. The motility and pliability of the pharyngeal wall and the mucosal surfaces are assessed. Tumor infiltration causes lack of pliability or distensibility, as well as mucosal irregularity.
Lateral radiograph of the neck showing the different structures of the larynx: a, vallecula; b, hyoid bone; c, epiglottis; d, pre-epiglottic space; e, ventricle (air-space between false and true cords); f, arytenoid; g, cricoid; and h, thyroid cartilage.
Computed Tomography
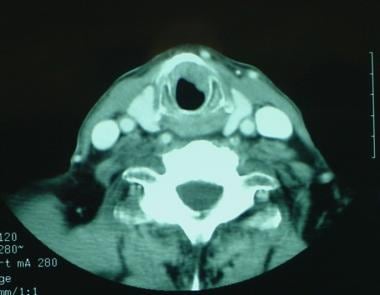
Imaging of laryngeal cancer includes contrast-enhanced helical CT scanning from the C1 vertebral body to the thoracic inlet, with the section plane parallel to the true vocal cords or the hyoid bone (see the images below). The section thickness should not exceed 3 mm. Patients should be instructed to breathe quietly. With new multidetector-row CT scanners, collimation can be 1 mm, and the larynx can be imaged in a few seconds, providing near-isometric Z -axis resolution with minimal motion artifacts. [8]
All laryngeal studies should be reconstructed using soft tissue algorithms. The area extending from the thyroid bone to the base of the cricoid cartilage is additionally reconstructed with a high-resolution bone algorithm to evaluate for cartilage invasion by tumor. Intravenous contrast enhancement helps distinguish vascular structures from lymph nodes.
CT has a high sensitivity and negative predictive value for detection of cartilage invasion using the following criteria: sclerosis, erosion, lysis, and extralaryngeal spread. By applying a combination of these criteria to all cartilages, a sensitivity as high as 91% and a negative predictive value of 95% can be obtained. [8]
Petragalla et al evaluated 40 patients for thyroid, arytenoid, and cricoid cartilage invasion on CT imaging who had undergone total laryngectomy for both primary and recurrent laryngeal carcinoma. CT erosion showed 100% agreement for thyroid inner cortex and cricoid cartilage invasion and 87% for arytenoid cartilage invasion. For primary tumors, CT demonstrated good (inner cortex 75%; full-thickness 85%), substantial (67.5%), and perfect (100%) accuracy in thyroid, arytenoid, and cricoid cartilage invasion, respectively. [12]
In a study, by Kuno et al, of 55 patients who underwent 3T MR imaging and 128-slice dual-energy CT for preoperative initial staging of laryngeal or hypopharyngeal squamous cell carcinomas, dual-energy CT showed higher specificity than MR imaging for diagnosing all cartilage together (84% for MR imaging versus 98% for dual-energy CT) and for thyroid cartilage (64% versus 100%). [14]
Magnetic Resonance Imaging
MRI of the larynx has several advantages over CT that may be helpful for presurgical planning. The multiplanar capabilities of MRI are superior to the reformations available with traditional CT. Coronal imaging is helpful for determining involvement of the laryngeal ventricle and transglottic spread. Midsagittal images are helpful for demonstrating the relationship between the tumor and the anterior commissure. MRI is also superior to CT for specific tissue characterization. However, the longer imaging time may contribute to image degradation by motion.
Hypointensity on T1-weighted images, hyperintensity on T2-weighted images, and gadolinium enhancement are suggestive of cartilage involvement. However, the only truly diagnostic finding is involvement of the strap muscles due to anterior extension of the tumor through the cartilage. MRI has been shown to have a sensitivity of 89-94%, a specificity of 74-88%, and a negative predictive value of 94-96% for the detection of neoplastic cartilage invasion [8] .
Studies have been done on the use of dextran-coated ultrasmall supramagnetic iron oxide (USPIO) to detect metastatic nodal disease. Patients are usually imaged 24-36 hours after the intravenous administration of USPIO. Compared with its noncontrast signal intensities, the signal intensity of a normally functioning lymph node after the administration of USPIO is markedly reduced on T1- and T2-weighted images as a result of both T2 relaxation and magnetic susceptibility effects due to the uptake of the iron particles by macrophages. A metastatic lymph node does not have a signal loss on contrast-enhanced images, because the macrophages of the node have been replaced. The sensitivity and specificity in detecting nodal metastases have been reported to be 87 and 90%, respectively.
The positive predictive value of MRI for neoplastic cartilage invasion (71%) is lower than the negative predictive value. [8, 9] In particular, the specificity of MRI for neoplastic invasion of thyroid cartilage is lower than that in the cricoid and arytenoid cartilages.
A diffusion-weighted MRI study found that apparent diffusion coefficient (ADC) is significantly and inversely correlated with cell density, nuclear area, and nuclear-cytoplasmic ratio in head and neck squamous cell carcinoma. ADC was significantly correlated with cellularity, stromal component, and nuclear-cytoplasmic ratio. In another study, ADC was found to be an independent predictor of prognosis in head and neck squamous cell carcinoma treated with radiotherapy. [10, 21]
In a prospective study that compared MRI to CT in preoperative staging of glottis cancer, MRI was shown to be more sensitive. MRI showed a diagnostic accuracy in 80% of cases, with a sensitivity of 100% and high specificity. CT accuracy was 70%, with low sensitivity but with high specific value. Statistical analysis showed that MRI has higher correlation with the pathology report than does CT. [11]
(See the images below.)
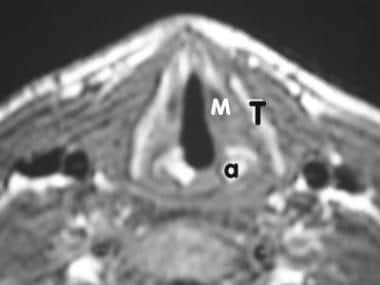 MR imaging, larynx. Image 1 of 3. Axial T1-weighted slice of the larynx showing the thyroid cartilage (T), arytenoid (a), and the thyroarytenoid muscle (M).
MR imaging, larynx. Image 1 of 3. Axial T1-weighted slice of the larynx showing the thyroid cartilage (T), arytenoid (a), and the thyroarytenoid muscle (M).
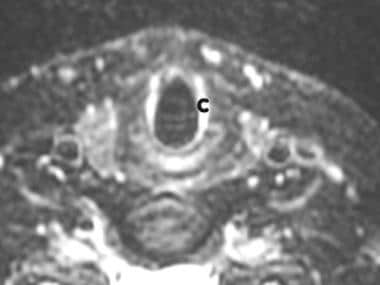 MR imaging, larynx. Image 2 of 3. Axial slice (slightly lower than Image 1) showing the cricoid cartilage.
MR imaging, larynx. Image 2 of 3. Axial slice (slightly lower than Image 1) showing the cricoid cartilage.
 MR imaging, larynx. Image 3 of 3. T1-weighted axial slice above Image 1 showing the epiglottis (arrow) and the vallecula, the hypointense area just anterior to the epiglottis.
MR imaging, larynx. Image 3 of 3. T1-weighted axial slice above Image 1 showing the epiglottis (arrow) and the vallecula, the hypointense area just anterior to the epiglottis.
 MR imaging, larynx. Sagittal localizer showing the epiglottis, valleculae, and base of the tongue.
MR imaging, larynx. Sagittal T1-weighted MRI of the larynx in a patient with squamous cell carcinoma. Note extension into the supraglottis.
MR imaging, larynx. Axial T1-weighted MRI of a patient with squamous cell carcinoma of the larynx. The tumor has invaded the thyroid cartilage.
MR imaging, larynx. Sagittal localizer showing the epiglottis, valleculae, and base of the tongue.
MR imaging, larynx. Sagittal T1-weighted MRI of the larynx in a patient with squamous cell carcinoma. Note extension into the supraglottis.
MR imaging, larynx. Axial T1-weighted MRI of a patient with squamous cell carcinoma of the larynx. The tumor has invaded the thyroid cartilage.
MRI technique
MRI is performed by using an anterior neck surface coil. T1- and T2-weighted images are obtained in the axial and coronal planes by using 3- or 5-mm-thick sections with a 1-mm gap. Peripheral gating and/or flow compensation may be used to decrease artifact from vascular flow. [8, 22]
Unlike CT, portions of the MRI examination should be performed before and after contrast enhancement. On nonenhanced studies, tumors are of intermediate signal intensity and easily distinguished from adjacent fat. After gadolinium enhancement, fat suppression helps in differentiating enhancing tumor from the normal pre-epiglottic and paraglottic fat.
Gadolinium-based contrast agents have been linked to the development of nephrogenic systemic fibrosis (NSF) or nephrogenic fibrosing dermopathy (NFD). The disease has occurred in patients with moderate to end-stage renal disease after being given a gadolinium-based contrast agent to enhance MRI or MRA scans. NSF/NFD is a debilitating and sometimes fatal disease. Characteristics include red or dark patches on the skin; burning, itching, swelling, hardening, and tightening of the skin; yellow spots on the whites of the eyes; joint stiffness with trouble moving or straightening the arms, hands, legs, or feet; pain deep in the hip bones or ribs; and muscle weakness.
Supraglottic carcinomas
The epiglottis is the most frequent location for cancers that arise in the supraglottic larynx. Tumors may arise from either the suprahyoid or infrahyoid epiglottis. Radiographically, these lesions are often exophytic and circumferential masses that, when detected early, are confined to the midline of the supraglottis. On MRI, these lesions are of intermediate signal intensity and homogeneously enhancing with the administration of contrast material.
Advanced lesions may extend superiorly to invade the vallecula and base of the tongue and also laterally to involve the aryepiglottic folds, false vocal cord, and paralaryngeal space. Direct inferior extension to involve the anterior commissure and subglottis is seen only in advanced lesions.
Tumors arising from the epiglottis may extend anteriorly to involve the pre-epiglottic space. This form of spread is facilitated by the presence of numerous foramina that provide access for tumoral invasion. Invasion of the pre-epiglottic space is often difficult to detect by means of clinical examination and, when present, alters the tumor stage (stage T3). Invasion of the pre-epiglottic space is readily seen on MRIs and best evaluated with nonenhanced T1 weighted images, which show replacement of normal high-signal-intensity fat by intermediate-signal-intensity tumor.
Tumors of the aryepiglottic fold are typically exophytic lesions that, when detected early, are confined laterally along the aryepiglottic fold. Advanced lesions may extend laterally to involve the adjacent wall of the pyriform sinus or medially to invade the epiglottis. These malignancies may also grow superiorly to involve the pharyngoepiglottic folds, and they may eventually involve the suprahyoid portion of the epiglottis. Inferiorly, these lesions may involve the false vocal cords and ventricle.
Advanced lesions may extend to involve the cricoarytenoid joint, resulting in fixation of the true vocal cord. They may invade the laryngeal cartilages, and they may also extend into the base of the tongue and pharyngeal walls.
Radiographically, early lesions are identified as lobulated masses arising from the aryepiglottic fold. Early mucosal lesions may not be depicted on MRIs.
Squamous cell cancers that arise from the false vocal cords and laryngeal ventricle tend to be ulcerative and infiltrative with a limited exophytic component. Deep invasion by such tumors results in their access to the paraglottic space, and this may lead to fixation of the supraglottic larynx. Because of their close proximity, these tumors may extend inferiorly to involve the true vocal cords. Such submucosal spread is often occult on clinical examination, and understaging of the lesions is possible if this extension is undetected before surgery.
Tumors of the false vocal cords may extend laterally to involve the medial wall of the pyriform sinus and medially to the inferior portion of the epiglottis, thereby increasing the likelihood of invasion of the pre-epiglottic space. MRI is well suited for the imaging of false vocal cord carcinomas. Coronal imaging is beneficial for evaluating the superior and inferior extent of these lesions and for evaluating the presence of transglottic spread.
Glottic carcinomas
The true vocal cords are the most common site of laryngeal carcinomas; the ratio of glottic carcinomas to supraglottic carcinomas is approximately 3:1. The anterior portion of the true vocal cord is the most common location of squamous cell cancer, with most lesions occurring along the free margin of the vocal cord. Anteriorly, the tumor may extend to the anterior commissure, where it may involve the contralateral true vocal cord.
Advanced lesions arising within the anterior aspect of the vocal cord or tumors arising along the posterior one third of the cord may extend posteriorly to involve the cricoarytenoid joint and interarytenoid region. Tumors may extend inferiorly, either mucosally or submucosally, to involve the subglottic region.
Early superficial mucosal lesions may not be detected with either CT or MRI. Larger lesions may result in thickening of the involved vocal cord.
The combination of coronal and axial images may be used to determine the amount of subglottic extension and the presence of cartilage invasion. Because the mucosa is near the perichondrium of the thyroid cartilage anteriorly and the cricoid cartilage posteriorly, the presence of soft tissue thicker than 1 mm in both of these areas is considered abnormal.
Invasion of the cartilage may be detected with both CT and MRI, and it is more common in glottic tumors than in subglottic carcinomas. MRI is more sensitive, but less specific, than CT in demonstrating cartilage involvement. The fatty marrow in the ossified cartilage has high signal intensity on T1-weighted images. Tumor infiltration into the cartilage results in decreased signal intensity of the marrow. If the cartilage is nonossified, T2-weighted images are more helpful because the tumor is usually hyperintense relative to the nonossified cartilage. Unfortunately, edema may be mistaken for tumor invasion on T2-weighted images.
The likelihood of nodal involvement associated with glottic carcinomas depends on the stage of the tumor. The incidence of early T1 lesions has been reported to be as low as 2%. This figure increases to approximately 20% for T3 and T4 lesions. The lymph nodes most at risk of metastases are those of the internal jugular chain. Paratracheal lymph nodes may be involved in glottic tumors that have significant subglottic spread.
Subglottic carcinomas
Subglottic carcinomas are rare and account for only 5% of all laryngeal carcinomas. The subglottic region is more commonly involved by the direct extension of a glottic or supraglottic carcinoma than by tumors elsewhere.
When present, these lesions are characteristically circumferential and often extend to involve the undersurface of the true vocal cords. They have a tendency for early invasion of the cricoid cartilage and extension through the cricothyroid membrane.
Primary subglottic carcinomas have a propensity to drain to the paratracheal lymph nodes. The reported incidence of clinically positive nodes in patients with subglottic carcinoma is 10%.
Hypopharyngeal carcinomas
Hypopharyngeal tumors can remain relatively asymptomatic for a long time. Extensive submucosal growth is common. At the time of diagnosis, as many as 75% of patients with hypopharyngeal tumors have metastases to cervical lymph nodes. Systemic metastases also develop in 20-40% of patients with hypopharyngeal tumors.
CT or MRI studies of hypopharyngeal cancer may demonstrate tumor that is more extensive than is apparent on clinical examination, usually because of submucosal spread of the cancer. [23] Carcinoma of the hypopharynx is most common in the pyriform sinus (60%), followed by the postcricoid region (25%) and the post-pharyngeal wall (15%).
Tumors of the pyriform sinus
Superficial mucosal extension into the apex of the pyriform sinus is not well seen with cross-sectional imaging, and it is best evaluated by means of endoscopy. A pyriform sinus tumor may spread submucosally into the posterior wall of the hypopharynx, the postcricoid region, or the aryepiglottic fold. Large tumors also extend up into the paraglottic fat, the pre-epiglottic fat, and the base of the tongue. These tumors may erode the posterosuperior cricoid cartilage and invade the upper pole of the thyroid gland. Tumors arising from the lateral wall or apex of the pyriform sinus have often already invaded the thyroid cartilage at the time of diagnosis.
Lesions of the medial wall of the pyriform sinus may spread along the aryepiglottic fold into the false vocal cord and anterior cartilage. They also may grow posteriorly into the postcricoid region and then cross the midline to involve the contralateral pyriform sinus. Medial wall lesions also invade paraglottic and pre-epiglottic fat.
Tumors of the postcricoid region
Tumors confined to the postcricoid region are rare. The exception occurs in patients (mostly women) with Plummer-Vinson syndrome. Often, tumors of the posterior wall invade the posterior larynx (arytenoids and posterior cricoid cartilage), causing vocal cord paralysis and hoarseness. Large tumors concentrically infiltrate and narrow the lumen of the hypopharynx. These tumors may extend to the cervical esophagus. The junction of the postcricoid region with the esophageal verge should be evaluated for tumor involvement.
Nuclear Imaging
Positron emission tomography (PET) with or without CT is emerging as a critical modality in the staging and monitoring of many head and neck cancers. Although PET provides little information about the extent of tumor within the larynx, the detection of metastases and the follow-up of treated patients increasingly relies on these modalities. [24] PET with CT is also becoming a critical component of intensity-modulated radiation treatment (IMRT). [8]
PET imaging relies on the increased glycolytic activity of neoplastic cells. Although highly sensitive, it does not provide the same anatomic detail that CT or MRI does, and therefore, it does not necessarily allow for precise localization of pathology or determination of involved structures within the larynx. Combined PET and CT scanners may help circumvent this limitation.
FDG-PET has been used to look for unknown primary lesions and second primaries, to stage disease prior to therapy, to detect residual and or recurrent disease after therapy, to assess the response to therapy, and to detect distant metastases. A significant limitation of 2-[fluorine-18]-fluoro-2-deoxy-D-glucose (FDG) PET scanning is its insensitivity to small tumor deposits, in the order of 3-4 mm or less.
PET has an advantage over CT and MRI for detection of distant metastases and for N-staging. It should be considered in patients with a high risk for distant metastases. [25] However, the negative predictive value in nodal metastasis assessment may not be sufficient to justify a change in treatment. Currently, the major value of PET may be in evaluation of the posttreatment larynx.
In a meta-analysis of 8 studies, PET showed a sensitivity of 89% and specificity of 74% for the diagnosis of recurrent laryngeal carcinoma after radiotherapy [26] . False-positive PET studies due to inflammation are not uncommon, particularly after therapy. However, the use of combined PET/CT imaging will reduce false-positive results. [27]
Pretreatment FDG PET/CT parameters have been shown to have prognostic value in patients with head and neck cancers, including oral, oropharyngeal, hypopharyngeal, and laryngeal squamous cell carcinomas. In one study, all of the FDG PET/CT parameters—maximum standardized uptake value (>10 g/mL) of the primary tumor, metabolic total volume (>20 cm3), total lesion glycolysis (>70 g), and uptake pattern (ring-shaped)—were significantly associated with negative effects on disease-specific survival and disease-free survival. Uptake pattern, in particular, provided better prognostic information to the clinical staging of head and neck squamous cell carcinomas than the other PET/CT parameters. [28]
In a study of the prognostic value of FDG-PET in patients with laryngeal cancer, the pretreatment SUVmax of nodal disease in patients with laryngeal cancer was found to be prognostic for recurrence. Multivariate analysis demonstrated that only the nodal SUVmax was a significantly unfavorable factor for progression-free survival and nodal progression-free survival. ROC curve analysis and log-rank test showed that patients with a high nodal SUVmax (≥4) had a significantly lower progression-free survival rate than those with a low SUVmax (< 4). [29]
Slevin et al confirmed that response-assessment FDG PET-CT after radiotherapy, with or without chemotherapy, for laryngeal and hypopharyngeal carcinomas has a high negative predictive value for both primary sites and lymph node sites and can therefore be used to guide treatment decisions. In 35 patients, sensitivity, specificity, positive predictive value, and negative predictive value for response-assessment FDG PET-CT for primary sites, respectively, were 100%, 73%, 46%, and 100%; and for nodal sites, 83%, 95%, 83%, and 95%. [18]
-
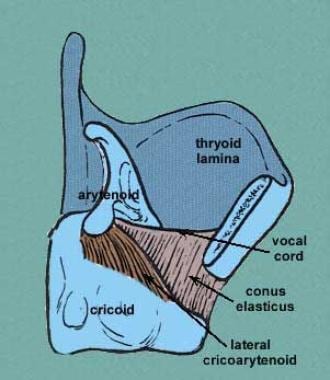
Image shows membranes of the larynx. Courtesy of Wesley Norman, PhD, DSc.
-
Anterior view of the laryngeal skeleton. Courtesy of Wesley Norman, PhD, DSc.
-
Posterior view of the laryngeal skeleton. Courtesy of Wesley Norman, PhD, DSc.
-
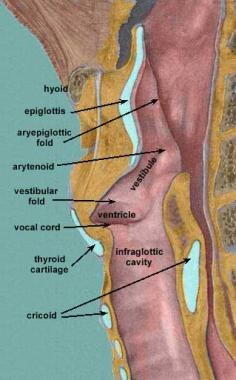
Sagittal view of the larynx. Courtesy of Wesley Norman, PhD, DSc.
-
Sagittal view of the larynx. Courtesy of Wesley Norman, PhD, DSc.
-
Posterior view of the laryngeal muscles. Courtesy of Wesley Norman, PhD, DSc.
-
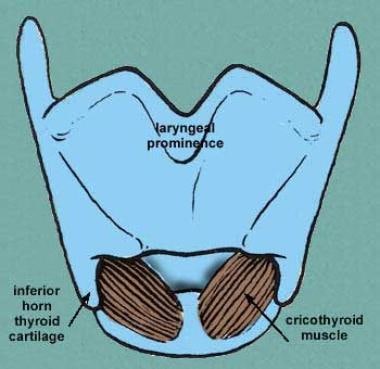
Anterior view of the laryngeal muscles. Courtesy of Wesley Norman, PhD, DSc.
-
Lateral radiograph of the neck showing the different structures of the larynx: a, vallecula; b, hyoid bone; c, epiglottis; d, pre-epiglottic space; e, ventricle (air-space between false and true cords); f, arytenoid; g, cricoid; and h, thyroid cartilage.
-
CT scan shows tumoral involvement of the right vocal cord.
-
CT scan shows a subglottic cancer along the cricoid cartilage.
-
MR imaging, larynx. Image 1 of 3. Axial T1-weighted slice of the larynx showing the thyroid cartilage (T), arytenoid (a), and the thyroarytenoid muscle (M).
-
MR imaging, larynx. Image 2 of 3. Axial slice (slightly lower than Image 1) showing the cricoid cartilage.
-
MR imaging, larynx. Image 3 of 3. T1-weighted axial slice above Image 1 showing the epiglottis (arrow) and the vallecula, the hypointense area just anterior to the epiglottis.
-
MR imaging, larynx. Sagittal localizer showing the epiglottis, valleculae, and base of the tongue.
-
MR imaging, larynx. Sagittal T1-weighted MRI of the larynx in a patient with squamous cell carcinoma. Note extension into the supraglottis.
-
MR imaging, larynx. Axial T1-weighted MRI of a patient with squamous cell carcinoma of the larynx. The tumor has invaded the thyroid cartilage.









