Practice Essentials
Lymphoma of the kidneys is diagnosed at the time of autopsy in almost one half of cases. It is rarely suspected on conventional urologic studies, such as intravenous urography. However, renal involvement with lymphoma is commonly discovered in patients with known lymphoma, who may be diagnosed, staged, or followed by cross-sectional imaging, such as computed tomography (CT) scanning (see the images below) or magnetic resonance imaging (MRI). [1, 2, 3, 4, 5] Patients with renal lymphoma may not be symptomatic; however, renal function laboratory studies occasionally reveal elevated blood urea nitrogen and creatinine levels, which may suggest an obstruction. Therefore, the patient may need to undergo radiologic evaluation. [6, 7, 8, 9, 10, 11]
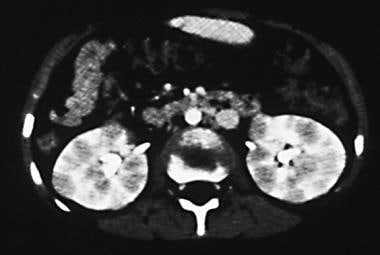
 Contrast-enhanced computed tomography (CT) scan obtained during the pyelographic phase for staging in a 17-year-old male adolescent with known lymphoma. This image reveals a hypoattenuating nodular pattern of different-sized lesions in both kidneys that represent bilateral renal lymphoma. Hypoattenuating nodes are also shown in the retroperitoneum.
Contrast-enhanced computed tomography (CT) scan obtained during the pyelographic phase for staging in a 17-year-old male adolescent with known lymphoma. This image reveals a hypoattenuating nodular pattern of different-sized lesions in both kidneys that represent bilateral renal lymphoma. Hypoattenuating nodes are also shown in the retroperitoneum.
 Computed tomography scan in a 17-year-old male adolescent with known lymphoma (same patient as in the previous image). This image was obtained 7 months after the initiation of chemotherapy in the patient and reveals complete resolution of the bilateral hypoattenuating lesions. The appearance and function of the kidneys are normal. Note the complete resolution of the retroperitoneal nodes.
Computed tomography scan in a 17-year-old male adolescent with known lymphoma (same patient as in the previous image). This image was obtained 7 months after the initiation of chemotherapy in the patient and reveals complete resolution of the bilateral hypoattenuating lesions. The appearance and function of the kidneys are normal. Note the complete resolution of the retroperitoneal nodes.
Preferred examination
Numerous diagnostic studies are available for the evaluation of renal involvement from lymphoma, including intravenous urography, ultrasonography, nuclear medicine, MRI, and CT scanning. [12, 13, 14] Although each technique may provide useful information in the detection, characterization, and staging of the disease, CT scanning remains the most sensitive, efficient, and comprehensive modality. [15, 16, 2] Indirect signs of primary renal lymphoma include renal size enlargement, sinus or hilum direct infiltration by a bulky mass, or diffuse retroperitoneal infiltration. [17]
Urography provides information regarding involvement of the collecting system, the functional status of the kidneys, and the severity of hydronephrosis. Ultrasonography is a good screening examination, particularly for the assessment and follow-up of patients with hydronephrosis. Intravenous urography can depict only the renal collecting system and suggestive large masses that have caused calyceal distortion. Small parenchymal masses and tumors around the kidney and in the retroperitoneum are often not demonstrated with this diagnostic examination.
Nuclear medicine studies, particularly those that use gallium-67 citrate, have a higher degree of specificity in the detection of lymphomatous infiltration of the kidneys. Although gallium-67 citrate is an isotope that often accumulates in lymphomatous tissue, it can also be taken up by inflammatory masses. 18F-fluorodeoxyglucose (FDG) positron emission tomography (PET) scanning has very high but not absolute specificity for malignant lymphoma. It has been reported that increased FDG uptake may also be observed in patients without active disease; in most cases, however, nonpathologic FDG accumulation is properly identified. [18, 19, 20]
MRI provides information for characterizing the lesion, and it is also helpful in assessing the renal vascular pedicle. [2, 5]
CT scanning is the diagnostic modality of choice in patients with suspected renal masses (see the images below). CT scans depict renal involvement in most patients with lymphoma, often help in defining the extent of disease within and outside of the kidneys, and provide information for staging of the patient's underlying malignancy. In addition, the result of treatment can be assessed on follow-up CT scans. The CT scan examination must be done with intravenous contrast media. Therefore, if contrast media cannot be used in patients for reasons such as renal failure or allergy to iodine, MRI then becomes the diagnostic modality of choice. Nonenhanced CT scan studies or MRIs can cause masses to be missed, particularly when such masses are small. [21, 22, 5]
On sonograms, the parenchymal masses are often hypoechoic, reflecting tissue homogeneity, and they can be misidentified as renal cysts.
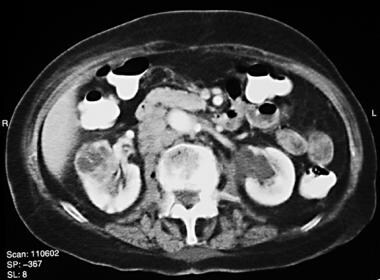
 Contrast-enhanced computed tomography scan in a 15-year-old male adolescent with non-Hodgkin lymphoma. This image shows a bilateral pattern of multiple small nodules that are almost of equal size and involve both kidneys.
Contrast-enhanced computed tomography scan in a 15-year-old male adolescent with non-Hodgkin lymphoma. This image shows a bilateral pattern of multiple small nodules that are almost of equal size and involve both kidneys.
 Sagittal baseline sonogram in a 15-year-old male adolescent with non-Hodgkin lymphoma. This image shows near-normal architecture of the left kidney. Both kidneys were reported as normal (left kidney size, 11.4 X 5.7 cm), and no indication of hydronephrosis was noted.
Sagittal baseline sonogram in a 15-year-old male adolescent with non-Hodgkin lymphoma. This image shows near-normal architecture of the left kidney. Both kidneys were reported as normal (left kidney size, 11.4 X 5.7 cm), and no indication of hydronephrosis was noted.
 Contrast-enhanced computed tomography scan obtained during the nephrographic phase in a 93-year-old woman with non-Hodgkin lymphoma, in whom renal lymphoma mimicked renal cell carcinoma. This image reveals a single mass with heterogeneous attenuation that involves the right kidney, as well as an associated lymphadenopathy in the right side of the retroperitoneum. The findings suggest renal cell carcinoma with ipsilateral adenopathy. A normal variant of an extrarenal pelvis is noted in the left side.
Contrast-enhanced computed tomography scan obtained during the nephrographic phase in a 93-year-old woman with non-Hodgkin lymphoma, in whom renal lymphoma mimicked renal cell carcinoma. This image reveals a single mass with heterogeneous attenuation that involves the right kidney, as well as an associated lymphadenopathy in the right side of the retroperitoneum. The findings suggest renal cell carcinoma with ipsilateral adenopathy. A normal variant of an extrarenal pelvis is noted in the left side.
 Contrast-enhanced, breath-hold, T1-weighted magnetic resonance image (MRI) (repetition time, 190 ms; echo time, 4 ms) in a 93-year-old woman with non-Hodgkin lymphoma. This image shows a mass with heterogeneous signal intensity in the right kidney; areas of low signal intensity reveal necrosis in the mass. MRI was performed to assess the renal vascular pedicle and inferior vena cava, both of which were free of tumor. Because of the patient's history of non-Hodgkin lymphoma (for which she received treatment), biopsy was performed to exclude renal cell carcinoma. The diagnosis of renal lymphoma was proven, and the patient received appropriate treatment.
Contrast-enhanced, breath-hold, T1-weighted magnetic resonance image (MRI) (repetition time, 190 ms; echo time, 4 ms) in a 93-year-old woman with non-Hodgkin lymphoma. This image shows a mass with heterogeneous signal intensity in the right kidney; areas of low signal intensity reveal necrosis in the mass. MRI was performed to assess the renal vascular pedicle and inferior vena cava, both of which were free of tumor. Because of the patient's history of non-Hodgkin lymphoma (for which she received treatment), biopsy was performed to exclude renal cell carcinoma. The diagnosis of renal lymphoma was proven, and the patient received appropriate treatment.
Radiography
With urography, the degree of confidence for the diagnosis of renal lymphoma is low. If renal involvement is suggested on an intravenous urogram, contrast-enhanced CT scanning or MRI must be performed. If the urographic findings are considered normal but the clinical findings (eg, abnormal renal function) suggest renal involvement, a cross-sectional study is indicated. [3]
Plain radiographs are limited when compared to other available modalities, such as CT scanning, ultrasonography, and MRI. Intravenous urography may show distortion of the collecting system as a result of a single or multiple renal masses. This finding cannot be differentiated from findings in simple cysts or renal cystic disease. However, intravenous urograms of renal lymphoma can demonstrate normal or near-normal findings. [23, 24]
In lymphomatous renal involvement, findings of an intravenous urogram can be normal and, therefore, falsely negative. With urography, a high rate of false-negative diagnoses is possible.
(See the images below.)
 Intravenous urogram obtained during the excretory phase in a 52-year-old woman with non-Hodgkin lymphoma who presented with flank pain. This image reveals a near-normal renal collecting system, with slightly enlarged kidneys and minimal narrowing of the proximal ureter that are suggestive of an external mass effect.
Intravenous urogram obtained during the excretory phase in a 52-year-old woman with non-Hodgkin lymphoma who presented with flank pain. This image reveals a near-normal renal collecting system, with slightly enlarged kidneys and minimal narrowing of the proximal ureter that are suggestive of an external mass effect.
 Autopsy specimen from a 52-year-old woman with non-Hodgkin lymphoma. Numerous lymphomatous nodules are visible throughout the kidneys.
Autopsy specimen from a 52-year-old woman with non-Hodgkin lymphoma. Numerous lymphomatous nodules are visible throughout the kidneys.
Computed Tomography
CT scans demonstrate a wide variety of appearances in renal lymphoma; the study patterns depend on the technique of CT scanning. Multidetector and spiral/helical CT scanning are universally accepted as the techniques of choice in patients with renal involvement, and they have a high degree of sensitivity in the detection of renal lymphoma. [21, 25, 22, 2, 3, 4, 5]
Breath-hold images can be quickly obtained during the multiple phases of renal enhancement after the intravenous injection of contrast medium. The nephrographic phase is the most important phase for renal parenchymal assessment. These images are essentially free of motion artifact and respiratory misregistration. This approach helps in accurately detecting and characterizing most renal masses, including smaller lesions that may involve the renal parenchyma in lymphoma.
In addition, the vascular phase of contrast enhancement enables characterization of the renal vasculature, which may be involved in renal cell carcinoma but uncommonly in renal lymphoma. Without intravenously administered contrast material, infiltrative forms of renal lymphoma can be entirely missed on CT scan studies. Also, CT scanning should not be limited to the cortical medullary phase of contrast enhancement because the lesions can be missed in this phase.
Typical imaging findings of renal lymphoma include multiple poorly enhancing masses, retroperitoneal tumors that directly invade the kidneys, a solitary mass, bilateral renal enlargement, and perirenal soft-tissue masses. Unless the renal lesions manifest in the setting of widespread lymphoma, percutaneous biopsy is indicated to differentiate lymphoma from metastases. Radiologists should be familiar with both the typical and atypical manifestations of renal lymphoma and should recommend imaging-guided percutaneous biopsy for diagnostic confirmation to avoid unnecessary nephrectomy. [26]
Multiple renal masses are most common in patients with lymphoma. The masses are typically bilateral, but they may also be unilateral. Multiple masses are seen in approximately 60% of patients, and they reflect advanced disease in patients who present for staging evaluation. Depending on the size and expansile nature of individual neoplastic deposits, little mass effect on the renal contour may be seen. Therefore, although renal involvement may be extensive, imaging findings can be subtle, and intravenous contrast enhancement is essential.
The masses range in size from a few millimeters to several centimeters and are seen as areas of low attenuation. Although the masses are often homogeneous on CT scans, they can be heterogeneous or low density, as well as mimic a complicated cyst. This is typically a sign of tumor necrosis in patients undergoing chemotherapy. In approximately 50% of patients, associated retroperitoneal adenopathy is noted.
(See the images below.)
 Computed tomography scan in a 36-year-old woman. This image reveals multiple lymphomatous masses that involve the right kidney, in which the largest mass shows areas of necrosis. A few lymph nodes are evident in the right-sided renal pedicle. Note that the patient has splenomegaly, with probable involvement of the liver and associated ascites and a vertebral bony lesion.
Computed tomography scan in a 36-year-old woman. This image reveals multiple lymphomatous masses that involve the right kidney, in which the largest mass shows areas of necrosis. A few lymph nodes are evident in the right-sided renal pedicle. Note that the patient has splenomegaly, with probable involvement of the liver and associated ascites and a vertebral bony lesion.
Solitary masses are reported in approximately 10-20% of patients (see the images below). The mass can be as large as 15 cm and can cause significant distortion of the renal contour. Solitary lesions resemble other renal neoplasms that grow primarily by expansion, including renal cell carcinoma or isolated metastasis.
 Computed tomography scan in a 53-year-old woman with lymphoma. A large relatively homogeneous mass involving the left kidney is associated with ipsilateral adenopathy. Note the beginning of minimal necrotic changes in the renal mass and the para-aortic nodes (cursors). A lymphomatous mass is seen in the liver. The pattern can be easily mistaken for renal cell carcinoma and associated with retroperitoneal adenopathy and hepatic metastasis. Note the thick-walled loop of small bowel from lymphoma anterior to the nodal mass.
Computed tomography scan in a 53-year-old woman with lymphoma. A large relatively homogeneous mass involving the left kidney is associated with ipsilateral adenopathy. Note the beginning of minimal necrotic changes in the renal mass and the para-aortic nodes (cursors). A lymphomatous mass is seen in the liver. The pattern can be easily mistaken for renal cell carcinoma and associated with retroperitoneal adenopathy and hepatic metastasis. Note the thick-walled loop of small bowel from lymphoma anterior to the nodal mass.
 Contrast-enhanced computed tomography (CT) scan in a 28-year-old woman with non-Hodgkin lymphoma, who presented with left flank pain. A renal sonogram (not shown) depicted left hydronephrosis and renal mass. This CT scan shows retroperitoneal extension of lymphoma to the left kidney, in which a large mass in the left side of the retroperitoneum extends into the left kidney. Adenopathy in the left hilar region appears to displace the renal vein and surround the renal artery without obstructing the blood flow. The posterior collecting system is dilated as a result of obstruction of the ureter by adenopathy that is present more caudally in the retroperitoneum (not shown).
Contrast-enhanced computed tomography (CT) scan in a 28-year-old woman with non-Hodgkin lymphoma, who presented with left flank pain. A renal sonogram (not shown) depicted left hydronephrosis and renal mass. This CT scan shows retroperitoneal extension of lymphoma to the left kidney, in which a large mass in the left side of the retroperitoneum extends into the left kidney. Adenopathy in the left hilar region appears to displace the renal vein and surround the renal artery without obstructing the blood flow. The posterior collecting system is dilated as a result of obstruction of the ureter by adenopathy that is present more caudally in the retroperitoneum (not shown).
Continuous retroperitoneal extension into the kidney is a common pattern of renal involvement in lymphoma and is seen in approximately 30% of patients (see the image below). Continuous extension typically results in a large, bulky retroperitoneal mass that envelops the renal vasculature and invades the renal hilus. In most patients, the renal vascular pedicle is patent and engulfed by the retroperitoneal mass. Continuous extension of retroperitoneal involvement in the renal collecting system can often cause obstruction, and patients commonly present with hydronephrosis.
 Contrast-enhanced computed tomography scan in a 28-year-old woman with non-Hodgkin lymphoma (same patient as in the previous image) that was obtained to evaluate response to chemotherapy approximately 5 months after the patient underwent treatment. This image shows a mild degree of atrophy in the left kidney but complete resolution of the adenopathy and mass. The atrophy may also have been the result of long-standing hydronephrosis.
Contrast-enhanced computed tomography scan in a 28-year-old woman with non-Hodgkin lymphoma (same patient as in the previous image) that was obtained to evaluate response to chemotherapy approximately 5 months after the patient underwent treatment. This image shows a mild degree of atrophy in the left kidney but complete resolution of the adenopathy and mass. The atrophy may also have been the result of long-standing hydronephrosis.
Rarely, perirenal disease is seen in an isolated form without involvement of the renal parenchyma or retroperitoneal nodes (see the images below). Occasionally, this feature is seen without compression of the renal parenchyma or functional impairment; such a finding is rare and virtually pathognomonic for perirenal lymphoma. A variety of CT scan manifestations of perirenal lymphoma, including renal sinus infiltration, thickening of the Gerota fascia, and perirenal masses, have been described. The normal renal parenchyma cannot be differentiated from the perirenal abnormality if intravenous contrast enhancement is not used in CT scanning.
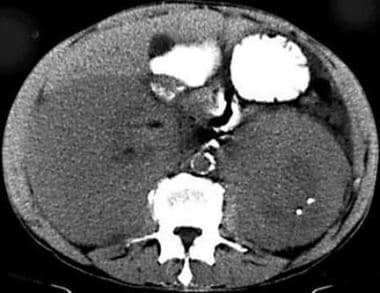 Nonenhanced computed tomography scan obtained in a 62-year-old man with a palpable flank mass and elevated levels of serum blood urea nitrogen and creatinine. This image shows large bilateral masses that cannot be distinguished from the renal parenchyma. A few calcifications are seen on the left side. No retroperitoneal adenopathy is noted.
Nonenhanced computed tomography scan obtained in a 62-year-old man with a palpable flank mass and elevated levels of serum blood urea nitrogen and creatinine. This image shows large bilateral masses that cannot be distinguished from the renal parenchyma. A few calcifications are seen on the left side. No retroperitoneal adenopathy is noted.
 Computed tomography scan in a 72-year-old woman with a known diagnosis of non-Hodgkin lymphoma. This image shows perirenal lymphoma with retroperitoneal adenopathy. Massive retroperitoneal adenopathy, splenomegaly, and a bilateral rim of low-attenuating tissue that surrounds the kidneys are noted. These findings are typical of perirenal lymphoma. The spleen has a large area of low attenuation as a result of tumor infiltration. Adenopathy, splenomegaly, and the perirenal process completely resolved after chemotherapy.
Computed tomography scan in a 72-year-old woman with a known diagnosis of non-Hodgkin lymphoma. This image shows perirenal lymphoma with retroperitoneal adenopathy. Massive retroperitoneal adenopathy, splenomegaly, and a bilateral rim of low-attenuating tissue that surrounds the kidneys are noted. These findings are typical of perirenal lymphoma. The spleen has a large area of low attenuation as a result of tumor infiltration. Adenopathy, splenomegaly, and the perirenal process completely resolved after chemotherapy.
Infiltrative disease is associated with lymphomatous proliferation within the interstitium of the kidney, which manifests as nephromegaly, with preservation of renal contour (see the image below). Diffuse infiltration is often bilateral and is seen in approximately 20% of patients. The diagnosis is often subtle and depends on the finding of global renal enlargement. Usually, kidneys infiltrated by lymphoma have poor function, but the disease is often clinically silent.
 Nonenhanced computed tomography scan in a 22-year-old woman with non-Hodgkin lymphoma and elevated levels of blood urea nitrogen and creatinine. An infiltrative pattern of renal lymphoma is seen as lymphomatous infiltration within the interstitium of the kidneys, which causes bilateral nephromegaly. Note the areas of slightly lower attenuation and the preservation of the renal contour.
Nonenhanced computed tomography scan in a 22-year-old woman with non-Hodgkin lymphoma and elevated levels of blood urea nitrogen and creatinine. An infiltrative pattern of renal lymphoma is seen as lymphomatous infiltration within the interstitium of the kidneys, which causes bilateral nephromegaly. Note the areas of slightly lower attenuation and the preservation of the renal contour.
Atypical manifestations of renal lymphomatous mass, such as spontaneous hemorrhage, necrosis, heterogeneous attenuation, cystic transformation, and calcifications, are occasionally depicted on CT scans. Often, these findings are the result of previous treatment for renal lymphoma. More commonly, the findings of renal lymphoma regress after chemotherapy, and the kidneys regain a normal CT scan appearance.
In patients who are immunocompromised, the prevalence of lymphoma is increased. Lymphoma typically occurs in patients with human immunodeficiency virus infection or in secondarily immunosuppressed recipients of organ transplants. Lymphoma is particularly common in patients who have undergone cyclosporine therapy.
Typically, lymphoma in patients who are immunocompromised is of small, noncleaved cell or immunoblastic origin and has a B-cell phenotype. This condition often has an extranodal origin, and the most common sites include the central nervous system, bone marrow, gastrointestinal tract, lungs, heart, and liver. Renal involvement also occurs in these patients, but it is uncommon.
Degree of confidence
In a patient with known lymphoma, low-attenuating perirenal masses or nodules almost always represent renal lymphoma. On contrast-enhanced CT scans, these lesions have attenuation values higher than those of simple fluid. Contrary to typical primary renal cell carcinoma, lymphomatous masses are often homogeneous and do not display significant enhancement. If the renal mass is exophytic, it causes vascular displacement and not encasement; the latter feature is common in renal cell carcinoma.
Such findings may be associated with retroperitoneal adenopathy; however, when a single mass is found, their differentiation from renal cell carcinoma may become difficult, and occasionally, biopsy may become necessary. In perirenal lymphoma (halo sign on sonograms), the degree of confidence is higher.
Magnetic Resonance Imaging
MRI findings in lymphoma are similar to those seen on CT scans, and they are diagnostic to the same degree. Usually, lymphoma displays low signal intensity on T1-weighted MRIs, and it is either isointense or moderately hyperintense on T2-weighted images. Lymphomatous tissue may be minimally enhancing, but it does not enhance as much as normal renal parenchyma; therefore, the lymphomatous tissue remains hypointense relative to the kidney on contrast-enhanced T1-weighted MRIs. [12, 22, 12, 22, 2, 3, 4, 5]
(See the images below.)
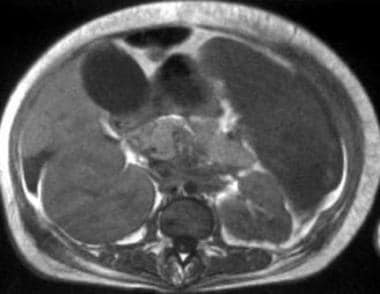 T1-weighted magnetic resonance image (repetition time, 650 ms; echo time, 25 ms) in a 36-year-old woman with bilateral renal lymphoma. This image reveals right-sided nephromegaly. No discrete nodule can be seen in the kidneys.
T1-weighted magnetic resonance image (repetition time, 650 ms; echo time, 25 ms) in a 36-year-old woman with bilateral renal lymphoma. This image reveals right-sided nephromegaly. No discrete nodule can be seen in the kidneys.
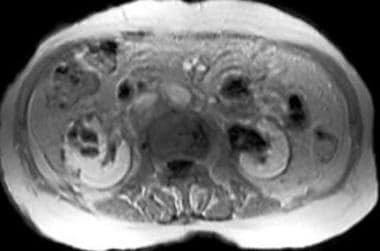
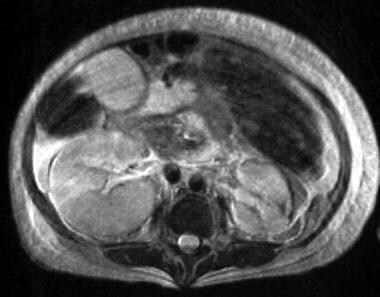 T2-weighted magnetic resonance image (repetition time, 2200 ms; echo time, 90 ms) in a 36-year-old woman with bilateral renal lymphoma. This image reveals heterogeneous intensity of the kidneys. Detection of discrete nodules is difficult.
T2-weighted magnetic resonance image (repetition time, 2200 ms; echo time, 90 ms) in a 36-year-old woman with bilateral renal lymphoma. This image reveals heterogeneous intensity of the kidneys. Detection of discrete nodules is difficult.
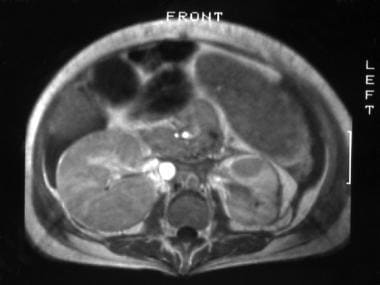 Contrast-enhanced T1-weighted magnetic resonance image (repetition time, 650 ms; echo time, 25 ms) in a 36-year-old woman with bilateral renal lymphoma. This image reveals enlargement of the right kidney with diffuse low signal intensity. The discrete low-intensity lesion in the left kidney is better depicted on the contrast-enhanced image. Note the splenomegaly with splenic involvement and ascites.
Contrast-enhanced T1-weighted magnetic resonance image (repetition time, 650 ms; echo time, 25 ms) in a 36-year-old woman with bilateral renal lymphoma. This image reveals enlargement of the right kidney with diffuse low signal intensity. The discrete low-intensity lesion in the left kidney is better depicted on the contrast-enhanced image. Note the splenomegaly with splenic involvement and ascites.
The degree of confidence of MRI for renal lymphoma depends on the technique that is used for scanning. On breath-hold high-resolution MRIs that are obtained with nonenhanced and contrast-enhanced sequences, MRI is probably equivalent to CT scanning.
When renal involvement is unilateral, it can mimic renal cell carcinoma (see the image below). When diffuse renal infiltration is noted without a discrete lesion, the possibility of a false-negative finding increases.
Contrast-enhanced, breath-hold, T1-weighted magnetic resonance image (MRI) (repetition time, 190 ms; echo time, 4 ms) in a 93-year-old woman with non-Hodgkin lymphoma. This image shows a mass with heterogeneous signal intensity in the right kidney; areas of low signal intensity reveal necrosis in the mass. MRI was performed to assess the renal vascular pedicle and inferior vena cava, both of which were free of tumor. Because of the patient's history of non-Hodgkin lymphoma (for which she received treatment), biopsy was performed to exclude renal cell carcinoma. The diagnosis of renal lymphoma was proven, and the patient received appropriate treatment.
Ultrasonography
Ultrasonography often demonstrates single or multiple renal masses that have low-level echoes (see the the first image below). Occasionally, the ultrasonographic findings may appear normal because of the small size of the renal nodules (see the second image below). In addition, varying degrees of hydronephrosis may be seen because of compression of the renal hilum that is caused by lymph nodes or obstruction of the ureters. [27, 5] As a result of the homogeneous nature of large lesions, these lesions appear hypoechoic on ultrasonography, but without enhanced through-transmission. Occasionally, differentiating large lesions from a simple or a complicated cyst is difficult. If the lesions are small or if the nature of involvement is diffuse, the ultrasonographic findings can be normal.
 Axial sonogram in a 22-year-old woman with known lymphoma. A baseline sonogram was performed, which demonstrated renal lymphoma. This image depicts a large kidney with heterogeneous echotexture and poorly defined areas of hypoechogenicity. A mild degree of hydronephrosis is noted. After chemotherapy, follow-up ultrasonographic images showed complete resolution of the renal lymphoma.
Sagittal baseline sonogram in a 15-year-old male adolescent with non-Hodgkin lymphoma. This image shows near-normal architecture of the left kidney. Both kidneys were reported as normal (left kidney size, 11.4 X 5.7 cm), and no indication of hydronephrosis was noted.
Axial sonogram in a 22-year-old woman with known lymphoma. A baseline sonogram was performed, which demonstrated renal lymphoma. This image depicts a large kidney with heterogeneous echotexture and poorly defined areas of hypoechogenicity. A mild degree of hydronephrosis is noted. After chemotherapy, follow-up ultrasonographic images showed complete resolution of the renal lymphoma.
Sagittal baseline sonogram in a 15-year-old male adolescent with non-Hodgkin lymphoma. This image shows near-normal architecture of the left kidney. Both kidneys were reported as normal (left kidney size, 11.4 X 5.7 cm), and no indication of hydronephrosis was noted.
On sonograms, a perirenal hypoechoic halo is characteristic of perirenal lymphoma (see the image below).
 Sonogram in a 62-year-old man who presented with palpable flank masses demonstrates perirenal lymphoma without retroperitoneal adenopathy. Although the left kidney appears to show no indication of a mass or hydronephrosis, a hypoechoic but solid-appearing area surrounds the kidney. The ultrasonographic findings may simply represent a perirenal complicated fluid collection or edema; however, perirenal lymphoma should be considered. Because of the underlying renal disease, the echotexture is increased throughout the kidney. This study was followed by computed tomography scanning and magnetic resonance imaging.
Sonogram in a 62-year-old man who presented with palpable flank masses demonstrates perirenal lymphoma without retroperitoneal adenopathy. Although the left kidney appears to show no indication of a mass or hydronephrosis, a hypoechoic but solid-appearing area surrounds the kidney. The ultrasonographic findings may simply represent a perirenal complicated fluid collection or edema; however, perirenal lymphoma should be considered. Because of the underlying renal disease, the echotexture is increased throughout the kidney. This study was followed by computed tomography scanning and magnetic resonance imaging.
Nuclear Imaging
Gallium-67 citrate has been used for diagnosing and staging lymphoma. This radioisotope concentrates in lymphoma; gallium is taken up by lymphomatous tissue in the kidneys, and it is also concentrated in inflammatory masses of the kidney. Therefore, obtaining the clinical history of patients is important. [13, 14]
18F-fluorodeoxyglucose (FDG) positron emission tomography (PET) scanning has very high but not absolute specificity for malignant lymphoma. It has been reported that increased FDG uptake may also be observed in patients without active disease; in most cases, however, nonpathologic FDG accumulation is properly identified. [18, 19, 20]
The use of another agent, technetium-99m (99Tc)-labeled antibody (LL2), has been advocated in imaging and staging lymphomas. Testing with gallium-67 citrate has an overall sensitivity of approximately 80% (see the image below). However, in patients with high-grade lymphoma, gallium scanning has a higher degree of sensitivity. LL2 scanning also has a sensitivity of 80%; however, in patients with low-grade lymphoma, LL2 imaging usually has a higher degree of sensitivity. [28]
Inconclusive scans are encountered with both gallium-67 citrate and FDG-PET. These cases are usually caused by inflammation, which subsequently resolves.
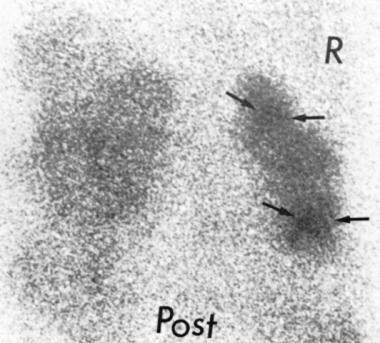 Gallium scan in a 55-year-old woman with known diffuse, poorly differentiated lymphoma who was admitted to the hospital because of renal failure. The patient had a creatinine level of 3. A sonogram (not shown) was performed and revealed no hydronephrosis. However, the echotexture of the kidneys was abnormal on the sonogram, and the possibility of renal lymphoma was suggested. This posterior view of the kidneys (Post) obtained at 72 hours after the injection of gallium-67 citrate shows multiple abnormal areas of increased uptake (arrows), particularly on the right side (R). This finding is consistent with renal involvement by lymphoma. Urinalysis results were normal, excluding underlying infection. Some residual gallium was noted in the colon. Gallium scan findings were normal 4 months after appropriate chemotherapy.
Gallium scan in a 55-year-old woman with known diffuse, poorly differentiated lymphoma who was admitted to the hospital because of renal failure. The patient had a creatinine level of 3. A sonogram (not shown) was performed and revealed no hydronephrosis. However, the echotexture of the kidneys was abnormal on the sonogram, and the possibility of renal lymphoma was suggested. This posterior view of the kidneys (Post) obtained at 72 hours after the injection of gallium-67 citrate shows multiple abnormal areas of increased uptake (arrows), particularly on the right side (R). This finding is consistent with renal involvement by lymphoma. Urinalysis results were normal, excluding underlying infection. Some residual gallium was noted in the colon. Gallium scan findings were normal 4 months after appropriate chemotherapy.
Questions & Answers
Overview
How is renal lymphoma diagnosed?
What is the role of imaging in the diagnosis of renal lymphoma?
What are limitations of imaging techniques for renal lymphoma?
What is the role of radiography in renal lymphoma imaging?
What is the role of CT scans in renal lymphoma imaging?
Which findings on CT scans are characteristic of renal lymphoma?
What is the accuracy of CT scanning in identifying renal lymphoma?
Which findings on MRI are characteristic of renal lymphoma?
Which findings on ultrasonography are characteristic of renal lymphoma?
What is the role of nuclear imaging in renal lymphoma imaging?
What is the role of angiography in renal lymphoma imaging?
-
Contrast-enhanced computed tomography (CT) scan obtained during the pyelographic phase for staging in a 17-year-old male adolescent with known lymphoma. This image reveals a hypoattenuating nodular pattern of different-sized lesions in both kidneys that represent bilateral renal lymphoma. Hypoattenuating nodes are also shown in the retroperitoneum.
-
Computed tomography scan in a 17-year-old male adolescent with known lymphoma (same patient as in the previous image). This image was obtained 7 months after the initiation of chemotherapy in the patient and reveals complete resolution of the bilateral hypoattenuating lesions. The appearance and function of the kidneys are normal. Note the complete resolution of the retroperitoneal nodes.
-
Contrast-enhanced computed tomography scan in a 15-year-old male adolescent with non-Hodgkin lymphoma. This image shows a bilateral pattern of multiple small nodules that are almost of equal size and involve both kidneys.
-
Sagittal baseline sonogram in a 15-year-old male adolescent with non-Hodgkin lymphoma. This image shows near-normal architecture of the left kidney. Both kidneys were reported as normal (left kidney size, 11.4 X 5.7 cm), and no indication of hydronephrosis was noted.
-
Contrast-enhanced computed tomography scan obtained during the nephrographic phase in a 93-year-old woman with non-Hodgkin lymphoma, in whom renal lymphoma mimicked renal cell carcinoma. This image reveals a single mass with heterogeneous attenuation that involves the right kidney, as well as an associated lymphadenopathy in the right side of the retroperitoneum. The findings suggest renal cell carcinoma with ipsilateral adenopathy. A normal variant of an extrarenal pelvis is noted in the left side.
-
Contrast-enhanced, breath-hold, T1-weighted magnetic resonance image (MRI) (repetition time, 190 ms; echo time, 4 ms) in a 93-year-old woman with non-Hodgkin lymphoma. This image shows a mass with heterogeneous signal intensity in the right kidney; areas of low signal intensity reveal necrosis in the mass. MRI was performed to assess the renal vascular pedicle and inferior vena cava, both of which were free of tumor. Because of the patient's history of non-Hodgkin lymphoma (for which she received treatment), biopsy was performed to exclude renal cell carcinoma. The diagnosis of renal lymphoma was proven, and the patient received appropriate treatment.
-
Intravenous urogram obtained during the excretory phase in a 52-year-old woman with non-Hodgkin lymphoma who presented with flank pain. This image reveals a near-normal renal collecting system, with slightly enlarged kidneys and minimal narrowing of the proximal ureter that are suggestive of an external mass effect.
-
Computed tomography (CT) scan in a 52-year-old woman with non-Hodgkin lymphoma. This image reveals diffuse renal lymphoma, in which diffuse, small nodules are scattered throughout both kidneys. The finding was not appreciated on the intravenous urogram and was only seen on contrast-enhanced CT scans. In fact, nonenhanced CT findings (not shown) were almost normal. The slight, narrowed ureter at the proximal portion, as seen on the urogram, was attributed to nephromegaly and compression of the ureter by the medial aspect of the kidney.
-
Autopsy specimen from a 52-year-old woman with non-Hodgkin lymphoma. Numerous lymphomatous nodules are visible throughout the kidneys.
-
Computed tomography scan in a 36-year-old woman. This image reveals multiple lymphomatous masses that involve the right kidney, in which the largest mass shows areas of necrosis. A few lymph nodes are evident in the right-sided renal pedicle. Note that the patient has splenomegaly, with probable involvement of the liver and associated ascites and a vertebral bony lesion.
-
Computed tomography scan in a 53-year-old woman with lymphoma. A large relatively homogeneous mass involving the left kidney is associated with ipsilateral adenopathy. Note the beginning of minimal necrotic changes in the renal mass and the para-aortic nodes (cursors). A lymphomatous mass is seen in the liver. The pattern can be easily mistaken for renal cell carcinoma and associated with retroperitoneal adenopathy and hepatic metastasis. Note the thick-walled loop of small bowel from lymphoma anterior to the nodal mass.
-
Contrast-enhanced computed tomography (CT) scan in a 28-year-old woman with non-Hodgkin lymphoma, who presented with left flank pain. A renal sonogram (not shown) depicted left hydronephrosis and renal mass. This CT scan shows retroperitoneal extension of lymphoma to the left kidney, in which a large mass in the left side of the retroperitoneum extends into the left kidney. Adenopathy in the left hilar region appears to displace the renal vein and surround the renal artery without obstructing the blood flow. The posterior collecting system is dilated as a result of obstruction of the ureter by adenopathy that is present more caudally in the retroperitoneum (not shown).
-
Contrast-enhanced computed tomography scan in a 28-year-old woman with non-Hodgkin lymphoma (same patient as in the previous image) that was obtained to evaluate response to chemotherapy approximately 5 months after the patient underwent treatment. This image shows a mild degree of atrophy in the left kidney but complete resolution of the adenopathy and mass. The atrophy may also have been the result of long-standing hydronephrosis.
-
Sonogram in a 62-year-old man who presented with palpable flank masses demonstrates perirenal lymphoma without retroperitoneal adenopathy. Although the left kidney appears to show no indication of a mass or hydronephrosis, a hypoechoic but solid-appearing area surrounds the kidney. The ultrasonographic findings may simply represent a perirenal complicated fluid collection or edema; however, perirenal lymphoma should be considered. Because of the underlying renal disease, the echotexture is increased throughout the kidney. This study was followed by computed tomography scanning and magnetic resonance imaging.
-
Nonenhanced computed tomography scan obtained in a 62-year-old man with a palpable flank mass and elevated levels of serum blood urea nitrogen and creatinine. This image shows large bilateral masses that cannot be distinguished from the renal parenchyma. A few calcifications are seen on the left side. No retroperitoneal adenopathy is noted.
-
T2-weighted magnetic resonance image (repetition time, 2000 ms; echo time, 80 ms) in a 62-year-old man with a palpable flank mass. This image reveals homogeneous high signal intensity masses that surround the kidneys. The left kidney can be distinguished because of the collecting system and the vascular pedicle. Note the patency of the renal vascular pedicle in the left side.
-
T2-weighted magnetic resonance image (repetition time, 2000 ms; echo time, 80 ms) in a 62-year-old man with a palpable flank mass. This image shows patency of the renal vascular pedicle on the right side. The normal renal parenchyma has a signal intensity that is slightly different from that of the surrounding perirenal mass. A diagnosis of perirenal lymphoma was proven by percutaneous biopsy.
-
Computed tomography scan in a 72-year-old woman with a known diagnosis of non-Hodgkin lymphoma. This image shows perirenal lymphoma with retroperitoneal adenopathy. Massive retroperitoneal adenopathy, splenomegaly, and a bilateral rim of low-attenuating tissue that surrounds the kidneys are noted. These findings are typical of perirenal lymphoma. The spleen has a large area of low attenuation as a result of tumor infiltration. Adenopathy, splenomegaly, and the perirenal process completely resolved after chemotherapy.
-
Nonenhanced computed tomography scan in a 22-year-old woman with non-Hodgkin lymphoma and elevated levels of blood urea nitrogen and creatinine. An infiltrative pattern of renal lymphoma is seen as lymphomatous infiltration within the interstitium of the kidneys, which causes bilateral nephromegaly. Note the areas of slightly lower attenuation and the preservation of the renal contour.
-
Contrast-enhanced computed tomography scan in a 36-year-old woman. This image shows bilateral small masses of different sizes due to lymphoma with involvement of the kidneys. The right kidney is more involved than the left. Associated adenopathy is noted in the retroperitoneum.
-
T1-weighted magnetic resonance image (repetition time, 650 ms; echo time, 25 ms) in a 36-year-old woman with bilateral renal lymphoma. This image reveals right-sided nephromegaly. No discrete nodule can be seen in the kidneys.
-
T2-weighted magnetic resonance image (repetition time, 2200 ms; echo time, 90 ms) in a 36-year-old woman with bilateral renal lymphoma. This image reveals heterogeneous intensity of the kidneys. Detection of discrete nodules is difficult.
-
Contrast-enhanced T1-weighted magnetic resonance image (repetition time, 650 ms; echo time, 25 ms) in a 36-year-old woman with bilateral renal lymphoma. This image reveals enlargement of the right kidney with diffuse low signal intensity. The discrete low-intensity lesion in the left kidney is better depicted on the contrast-enhanced image. Note the splenomegaly with splenic involvement and ascites.
-
Axial sonogram in a 22-year-old woman with known lymphoma. A baseline sonogram was performed, which demonstrated renal lymphoma. This image depicts a large kidney with heterogeneous echotexture and poorly defined areas of hypoechogenicity. A mild degree of hydronephrosis is noted. After chemotherapy, follow-up ultrasonographic images showed complete resolution of the renal lymphoma.
-
Gallium scan in a 55-year-old woman with known diffuse, poorly differentiated lymphoma who was admitted to the hospital because of renal failure. The patient had a creatinine level of 3. A sonogram (not shown) was performed and revealed no hydronephrosis. However, the echotexture of the kidneys was abnormal on the sonogram, and the possibility of renal lymphoma was suggested. This posterior view of the kidneys (Post) obtained at 72 hours after the injection of gallium-67 citrate shows multiple abnormal areas of increased uptake (arrows), particularly on the right side (R). This finding is consistent with renal involvement by lymphoma. Urinalysis results were normal, excluding underlying infection. Some residual gallium was noted in the colon. Gallium scan findings were normal 4 months after appropriate chemotherapy.









