Practice Essentials
Intussusception is the most common cause of bowel obstruction in children 3 months to 6 years of age. [1, 2, 3] Invagination of a bowel segment (usually, the small bowel) into the lumen of the more distal bowel (usually, the colon) occurs. The invaginated segment (intussusceptum) is carried distally by peristalsis. Mesentery and vessels become involved with the intraluminal loop and are squeezed within the engulfing segment (intussuscipiens). Almost all occurrences are acute, and bowel obstruction is often the presenting sign of intussusception. [4]
When this condition occurs in neonates and in children older than 2 years, there is a high incidence of associated bowel abnormality that serves as an initiating lead point for intussusception (about 5% of patients are found to have a lead point). In addition, intussusception is known to occur with greater frequency in children who have undergone abdominal surgery recently, either intraperitoneal or retroperitoneal operations. It is thought that early adhesions or focal edema of the bowel wall create a lead point for the intussusception. A number of studies have shown that rotavirus vaccine is associated with an increased risk of intussusception, particularly after administration of the first dose. [5, 6, 7, 8, 9, 10, 11, 12, 13, 14]
(See the image below.)
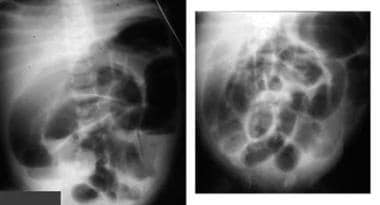 Upright and supine anteroposterior abdominal radiographs in an infant with crying and bloody diarrhea for 12 hours show a small bowel obstruction pattern and little gas in the cecal region.
Upright and supine anteroposterior abdominal radiographs in an infant with crying and bloody diarrhea for 12 hours show a small bowel obstruction pattern and little gas in the cecal region.
A loop of bowel infolds (and inverts) more distally into the lumen of the bowel and is then carried distally by peristalsis. Approximately 90% of intussusceptions are ileocolic, in which the terminal ileum is carried through the ileocecal valve into the colon; it may reach the rectum. Idiopathic intussusceptions usually lack an identifiable lead point and occur in children aged 6 months to 2 years. Lymphoid hyperplasia or hypertrophic lymph nodes have been postulated but not proven. Lead points in nonidiopathic intussusception may include the following:
-
Lymphoma of bowel
-
Leukemia involving bowel
-
Henoch-Schonlein purpura with intramural hemorrhage
-
Cystic fibrosis with inspissated bowel content
-
Postoperative complication following retroperitoneal surgery
-
Post abdominal trauma
-
Polyps
-
Peutz-Jeghers syndrome appendix (normal or appendicitis)
Imaging modalities
In some countries, history and physical findings are sufficient criteria for undertaking reduction procedures for intussusception. However, abdominal radiography and ultrasonography may be useful studies, and in some institutions, reduction of the intussusception takes place under ultrasonographic guidance with fluid or air. [15, 16, 17, 18, 19, 20, 21]
Studies advocating the use of point-of-care ultrasound (POCUS) for emergent diagnosis by emergency department physicians have reported sensitivities of 94.9-100% and specificities of 95.6-99.1%. [22, 23, 24] A retrospective study of 70 confirmed cases of intussusception using POCUS noted that intussusception was largely diagnosed in the early stages. The researchers concluded that early diagnosis benefited patients by reducing the duration of symptoms to a relatively short mean of 11.7 hours. Only 2 patients required surgical intervention, while the remaining 68 patients (97.1%) were successfully treated with air enema reduction. [23]
In a prospective cohort study conducted by Tonson la Tour et al at a tertiary care pediatric ED, POCUS identified 39 of 45 intussusception cases, with a sensitivity of .87% (95% confidence interval [CI] = 0.74 to 0.94). A normal or inconclusive POCUS was reported for 83 of the 86 negative studies, with a specificity of 97% (95% CI = 0.90 to 0.99). [25]
Abdominal radiography may be used to search for dilated small bowel and an absence of gas in the region of the cecum (see the image below). In some cases, a mass impression within the colonic gas indicates an intraluminal mass created by the intussuscepting loop.
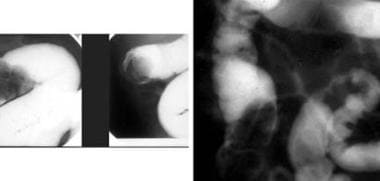
 Left: Radiograph from a 14-month-old boy who experienced blood in the stool for 3 days. An absence of cecal air and an obstruction pattern are seen. Right, top: A spot radiograph during an air reduction shows the intussusceptum. Right, bottom: The reduced intussusception with air in the small bowel is seen.
Left: Radiograph from a 14-month-old boy who experienced blood in the stool for 3 days. An absence of cecal air and an obstruction pattern are seen. Right, top: A spot radiograph during an air reduction shows the intussusceptum. Right, bottom: The reduced intussusception with air in the small bowel is seen.
Transverse ultrasonograms show a mass with a swirled appearance of alternating sonolucent and hyperechoic bowel wall of the loop-within-a-loop. On longitudinal ultrasonograms, the intussuscipiens and the intussusceptum have the appearance of a submarine sandwich. There appear to be multiple layers, which represent the walls of the intussuscepted bowel loops, as seen in the image below.
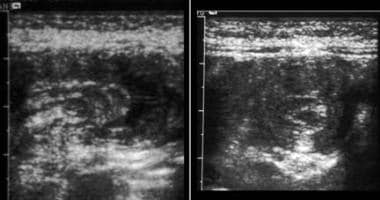 Longitudinal ultrasonograms of a patient with suspected intussusception shows the layered bowel walls of the outer and inner loop, the intussuscipiens, and the intussusceptum.
Longitudinal ultrasonograms of a patient with suspected intussusception shows the layered bowel walls of the outer and inner loop, the intussuscipiens, and the intussusceptum.
Intussusception may not be apparent on plain-film abdominal radiography. Radiographs may appear indeterminate or normal; therefore, the presence of an unremarkable abdominal radiograph should not be the basis for excluding a diagnosis of intussusception.
Ultrasonographic examination is almost always positive, although overlying loops of air-containing bowel may obscure intussusception (see the image below).
 Note the typical mass creates a curved density to the air in the transverse colon.
Note the typical mass creates a curved density to the air in the transverse colon.
The differential diagnosis should include appendicitis and cecal volvulus. Other conditions that should be considered include inflammatory bowel disease, incarcerated inguinal hernia, internal hernia, Henoch-Schonlein purpura, hemolytic uremic syndrome, small bowel obstruction, sigmoid volvulus, and abdominal wall hernia.
Radiologic interventions
Prolonged intussusception may result in bowel necrosis and/or perforation. Once the patient is stabilized, reduction procedures should be initiated immediately; radiographic examination and physical examination should be performed to ensure that neither free air nor peritonitis is present. It should be ascertained by physical examination that no peritonitis is present.
Both air and radiopaque liquid contrast have been used to reduce ileocolic intussusception under fluoroscopy. Fluoroscopic intussusception reduction using air enema has been found to use less than 50% of the radiation dose of liquid-contrast enema. [21]
Unless perforation, peritonitis, or Henoch-Schonlein purpura is present, radiologic reduction should be attempted. The success rate is 50-85%, depending on factors such as the length of time of the intussusception and degree of edema of the loop and ileocecal valve. Reduction is still possible, although more difficult, in intussusceptions that have been in place for longer than 48 hours. In patients older than 2 years, it should be assumed that intussusception has a lead point etiology; in such cases, further investigation should be undertaken. [19, 20, 21, 26, 27, 28, 29, 30]
Spontaneous reduction has been reported, but it is unusual. and surgery is advised when radiologic reduction is unsuccessful. Despite positive results from reduction through the use of imaging techniques, reduction or re-intussusception may be unsuccessful, necessitating surgery. Rarely, complications from reduction with imaging techniques (perforation) require emergency surgery. The use of air, gas, or water-soluble contrast to reduce the intussusception decreases potential complications. [31, 32]
In the current method of air reduction, room air is introduced through a rectal catheter and is taped well in place. A manometer is attached to a Y-connector to monitor pressure in the colon. Pressure should never exceed 110 mm Hg. The air pressure on the intussusception usually forces the inverted bowel back through the ileocecal valve and into its proper position. When reduction occurs, the observed pressure falls precipitously.
Radiographs may offer prognostic information regarding the potential success of therapeutic air enema, as well as potential surgical outcomes in patients in whom enema reduction fails. [19]
Contrast reduction was widely used until the current decade. A large rectal tube is taped firmly in place, and dilute water-soluble contrast is introduced slowly by gravity drip into the rectum; hydrostatic pressure is used to reduce the intussusception. The fluid is placed a maximum of 3 ft above the level of the radiography table. No more than 3 attempts at reduction are undertaken, and the column is pressed against the intussusception mass no longer than 3 min at each attempt. Visualization of the small bowel usually indicates that intussusception has been reduced. Palpation of the abdomen should be avoided during reduction.
Reduction may proceed at an uneven rate, and it may slow at various locations; this is particularly true at the ileocecal valve, which is swollen and often resists passage of the intussusception (see the images below). To ensure reduction, contrast should be observed entering the ileum. Once contrast enters the ileum, it often proceeds quickly through the ileum. Vomiting is a frequent side effect of reduction.
 Reduction of an intussusceptum through the ileocecal valve is the most difficult part of the reduction. The mass is seen in the cecum.
Reduction of an intussusceptum through the ileocecal valve is the most difficult part of the reduction. The mass is seen in the cecum.
 Same patient as in the previous image. On the second attempt at reduction, the intussusceptum still extends through the ileocecal valve. Reduction was unsuccessful.
Same patient as in the previous image. On the second attempt at reduction, the intussusceptum still extends through the ileocecal valve. Reduction was unsuccessful.
 The ileocecal valve is usually quite edematous after an intussusception has occurred; it may remain large for several days. In this patient, the ileocecal valve was mistaken for an intussusception, although barium had entered the ileum.
The ileocecal valve is usually quite edematous after an intussusception has occurred; it may remain large for several days. In this patient, the ileocecal valve was mistaken for an intussusception, although barium had entered the ileum.
The appendix usually fills before the ileum and should not be confused with the ileal reflux of contrast. If there is a problem with reduction across the ileocecal valve, the patient should be allowed to evacuate, and the ileum should then be refilled; this relaxes the valve and allows for better control on refilling. A swollen ileocecal valve may appear unreduced; therefore, identifying air or contrast material in the ileum is important (see the image below).
 From the same patient as in the previous image. The appearance of the ileocecal valve at resection is edematous and enlarged.
From the same patient as in the previous image. The appearance of the ileocecal valve at resection is edematous and enlarged.
Special concerns
One should be aware of conditions that lead to intussusception and that are predictive of perforation (eg, Henoch-Schonlein purpura). Contrast enema procedures should be avoided in patients with these conditions.
There are a number of case reports of intussusception in infants 2.5-10 mo of age who had laboratory-confirmed SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2) infection but no respiratory symptoms. One case was fatal. COVID-19 testing should be considered for children with intussusception, especially in those with a history of SARS-CoV-2 exposure or with signs and symptoms of COVID-19. Development of gastrointestinal symptoms in COVID-19–positive children should raise concern about the development of intussusception. [33, 34]
Radiography
Radiographic findings may be normal. However, usually, a pattern of small bowel obstruction with absence of gas in the right colon is visible. An intraluminal colonic filling defect may indicate intussusceptum, and intraluminal blood may create a speckled pattern of gas and colonic material.
A careful search should be made for intraperitoneal free air; the presence of free air is a contraindication for reduction by enema, because the presence of free air indicates that the bowel is already perforated (see the images below).
 In these x-rays of a patient being treated with contrast enema, the convex-shaped filling defect of the intussusceptum should be noted; the intussusceptum is reduced to the level of the cecum.
In these x-rays of a patient being treated with contrast enema, the convex-shaped filling defect of the intussusceptum should be noted; the intussusceptum is reduced to the level of the cecum.
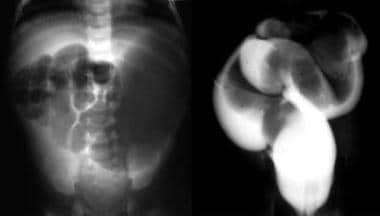 Images from a vomiting 10-month-old infant with a palpable abdominal mass. Note the obstruction pattern on plain radiograph and the intussusceptum in the sigmoid colon on contrast enema.
Images from a vomiting 10-month-old infant with a palpable abdominal mass. Note the obstruction pattern on plain radiograph and the intussusceptum in the sigmoid colon on contrast enema.
 A contrast-reduced intussusception shows backward flow of barium into the small bowel.
A contrast-reduced intussusception shows backward flow of barium into the small bowel.
The appearance of small bowel obstruction in conjunction with characteristic clinical findings almost always indicates intussusception, as does the appearance of a gasless cecum and/or an intraluminal bowel mass. Unless otherwise indicated, the diagnosis should be confirmed with an air or barium enema.
Any abnormality that has an appearance that looks like that of small bowel obstruction mimics intussusception, because findings often are nonspecific. In addition, appendicitis may have an "empty cecum" appearance that looks like intussusception, whereas inflammatory bowel disease may involve the cecum and appear like intussusception. Severe edema of the bowel wall, as found in shigellosis, Salmonella infection, or enterohemorrhagic Escherichia coli infection, may appear to be intussusception.
Radiographs may offer prognostic information regarding the potential success of therapeutic air enema, as well as potential surgical outcomes in patients in whom enema reduction fails. [19]
Computed Tomography
Computed tomography (CT) scanning is not normally indicated in child intussusception; however, if a lead point (eg, lymphoma) is suspected, CT scanning may be helpful (See the image below). Volvulus and some intraperitoneal masses (eg, cystic teratoma) mimic intussusception.
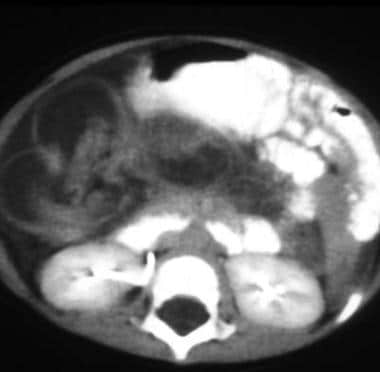 Computed tomography (CT) scanning is not indicated for intussusception; however, this infant was thought to have an abdominal mass. Note the dilated bowel with an internal loop shown on the single section from an abdominal CT scan.
Computed tomography (CT) scanning is not indicated for intussusception; however, this infant was thought to have an abdominal mass. Note the dilated bowel with an internal loop shown on the single section from an abdominal CT scan.
Ultrasonography
Transverse sonography of the intussusception mass reveals a swirled pattern of alternating hyperechogenicity and hypoechogenicity, representing the alternating layers of mucosa, muscularis, and serosa. Some centers use ultrasonography to monitor reduction of the intussusception with fluid introduced via the rectum. On ultrasonography, intussusception has a characteristic appearance; it is usually not mistaken for other bowel abnormalities. [35, 36] On longitudinal sonography, alternating loops of bowel and a loop-within-loop have a sandwichlike appearance (see the image below).
Longitudinal ultrasonograms of a patient with suspected intussusception shows the layered bowel walls of the outer and inner loop, the intussuscipiens, and the intussusceptum.
Studies advocating the use of point-of-care ultrasound (POCUS) for emergent diagnosis by emergency department physicians have reported sensitivities of 94.9-100% and specificities of 95.6-99.1%. [22, 23, 7, 24, 30] A retrospective study of 70 confirmed cases of intussusception using POCUS noted that intussusception was largely diagnosed in the early stages. The researchers concluded that early diagnosis benefited patients by reducing the duration of symptoms to a relatively short mean of 11.7 hours. Only 2 patients required surgical intervention, while the remaining 68 patients (97.1%) were successfully treated with air enema reduction. [23]
In a prospective cohort study conducted by Tonson la Tour et al at a tertiary care pediatric ED, POCUS identified 39 of 45 intussusception cases, with a sensitivity of 87% (95% confidence interval [CI] = 0.74 to 0.94). A normal or inconclusive POCUS was reported for 83 of the 86 negative studies, with a specificity of 97% (95% CI = 0.90 to 0.99). [25]
-
Upright and supine anteroposterior abdominal radiographs in an infant with crying and bloody diarrhea for 12 hours show a small bowel obstruction pattern and little gas in the cecal region.
-
In these x-rays of a patient being treated with contrast enema, the convex-shaped filling defect of the intussusceptum should be noted; the intussusceptum is reduced to the level of the cecum.
-
Longitudinal ultrasonograms of a patient with suspected intussusception shows the layered bowel walls of the outer and inner loop, the intussuscipiens, and the intussusceptum.
-
Images from a vomiting 10-month-old infant with a palpable abdominal mass. Note the obstruction pattern on plain radiograph and the intussusceptum in the sigmoid colon on contrast enema.
-
Left: Radiograph from a 14-month-old boy who experienced blood in the stool for 3 days. An absence of cecal air and an obstruction pattern are seen. Right, top: A spot radiograph during an air reduction shows the intussusceptum. Right, bottom: The reduced intussusception with air in the small bowel is seen.
-
Surgical specimen of an intussusception. Note the dilated intussuscipiens.
-
Note the internal inverted loop of bowel in the specimen.
-
Computed tomography (CT) scanning is not indicated for intussusception; however, this infant was thought to have an abdominal mass. Note the dilated bowel with an internal loop shown on the single section from an abdominal CT scan.
-
Note the typical mass creates a curved density to the air in the transverse colon.
-
A contrast-reduced intussusception shows backward flow of barium into the small bowel.
-
Reduction of an intussusceptum through the ileocecal valve is the most difficult part of the reduction. The mass is seen in the cecum.
-
Same patient as in the previous image. On the second attempt at reduction, the intussusceptum still extends through the ileocecal valve. Reduction was unsuccessful.
-
The ileocecal valve is usually quite edematous after an intussusception has occurred; it may remain large for several days. In this patient, the ileocecal valve was mistaken for an intussusception, although barium had entered the ileum.
-
From the same patient as in the previous image. The appearance of the ileocecal valve at resection is edematous and enlarged.





