Practice Essentials
The word hydranencephaly is a fusion of hydrocephalus and anencephaly, but the condition actually represents a distinct disorder and is primarily a disease of the fetus; encephaloclastic encephalomalacia can occur in cases of severe perinatal insult. [1] Hydranencephaly occurs in less than 1 in 10,000 births and is characterized by near-total or total absence of the cerebral cortex and basal ganglia. The thalami, pons, cerebral peduncles, and cerebellum are usually present, as may be a small amount of tissue from the occipital, frontal, and temporal lobes. [2] There is no known sex or racial predilection. [3]
Knowledge about possible etiologies of hydranencephaly comes from various observations and experiments. [4] Studies in sheep and monkeys have demonstrated that bilateral ligation of the carotid arteries results in destruction of the cerebral hemispheres, with relative preservation of the portions of the brain supplied by the posterior circulation, giving an appearance similar to that of hydranencephaly. [5]
Because cerebrospinal fluid (CSF) diversion can successfully treat children with hydrocephalus, the distinction between hydranencephaly and hydrocephalus is critical. [6] This distinction is also important in prognostic terms, as well as in connection with family support. However, differentiating hydranencephaly from hydrocephalus and alobar holoprosencephaly in the prenatal period can be challenging; in difficult cases, prenatal magnetic resonance imaging (MRI) can be used to establish the correct diagnosis [7] (see MRI).
In utero, hydranencephaly is frequently diagnosed with ultrasonography (see the following images); postnatally, cranial ultrasonography can detect the absence of cerebral tissue (see Ultrasound). However, MRI is probably the best modality for the overall evaluation of the anomaly and for the documentation of cortical remnants. [8, 9]
On prenatal ultrasound, an intact falx and a fluid-filled cranium can be seen. in newborns, macrocephaly and calvarial transillumination are present. The intact falx in hydranencephaly differentiates it from alobar holoprosencephaly. [10, 11]
 Ultrasonogram obtained at 14 weeks' gestation in a fetus with hydranencephaly shows unfused thalami surrounded by fluid. Note the lack of cerebral hemispheric tissue.
Ultrasonogram obtained at 14 weeks' gestation in a fetus with hydranencephaly shows unfused thalami surrounded by fluid. Note the lack of cerebral hemispheric tissue.
 Sagittal image in a fetus with hydranencephaly at 14 weeks' gestation. This ultrasonogram demonstrates the absence of the cerebral hemispheres (which have been replaced by fluid). Because of the early age of gestation, hydranencephaly was difficult to distinguish from hydrocephalus. Hydranencephaly was confirmed on a level III ultrasonogram (not shown).
Sagittal image in a fetus with hydranencephaly at 14 weeks' gestation. This ultrasonogram demonstrates the absence of the cerebral hemispheres (which have been replaced by fluid). Because of the early age of gestation, hydranencephaly was difficult to distinguish from hydrocephalus. Hydranencephaly was confirmed on a level III ultrasonogram (not shown).
Computed Tomography
In hydranencephaly, computed tomography (CT) scanning demonstrates an absence of most of the supratentorial structures, with preservation of the falx, thalami, and various amounts of the occipital lobes and basal ganglia (see the images below). Macrocrania or microcrania may be present, or the head circumference may be normal.
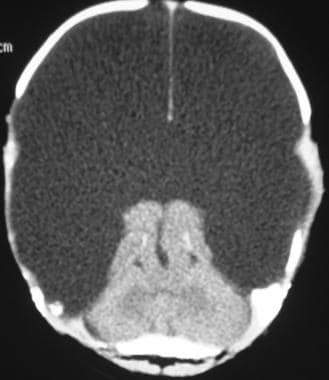 Axial computed tomography (CT) scan demonstrates an intact falx and separate thalami that suggest a diagnosis of hydranencephaly. Note the presence of the posterior fossa structures but the absence of the cerebral hemispheres.
Axial computed tomography (CT) scan demonstrates an intact falx and separate thalami that suggest a diagnosis of hydranencephaly. Note the presence of the posterior fossa structures but the absence of the cerebral hemispheres.
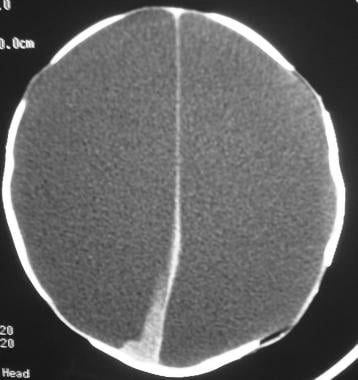 Computed tomography (CT) scan in a patient in whom another CT scan demonstrated an intact falx and separate thalami that suggested a diagnosis of hydranencephaly. The image shown here demonstrates a complete absence of the cerebral hemispheres, with a small amount of occipital cortex remaining. The absence of a circumferential rim of residual cerebral hemispheric tissue eliminates hydrocephalus as a diagnostic consideration.
Computed tomography (CT) scan in a patient in whom another CT scan demonstrated an intact falx and separate thalami that suggested a diagnosis of hydranencephaly. The image shown here demonstrates a complete absence of the cerebral hemispheres, with a small amount of occipital cortex remaining. The absence of a circumferential rim of residual cerebral hemispheric tissue eliminates hydrocephalus as a diagnostic consideration.
Although no normal variants mimic hydranencephaly, hydranencephaly and severe hydrocephalus may appear similar on CT scans owing to the fact that in both entities the falx is present and the thalami are unfused. [9] The brainstem is seen in hydranencephaly and hydrocephalus.
The key to distinguishing hydrocephalus from hydranencephaly is the presence of a thin rim of residual cerebral cortical tissue in hydrocephalus that is not present in hydranencephaly. Because cortical tissue below the parietal bony convexity may be overlooked on CT scans, thin sections and overlapped coronal reconstructions may be helpful in detecting this rim. In severe hydrocephalus, MRI can reliably depict the remaining cerebral cortical rim. [8, 9] In addition, the third ventricle, which is absent in hydranencephaly, is identifiable in hydrocephalus.
Magnetic Resonance Imaging
MRI is probably the best modality for the overall evaluation of the anomaly and for the documentation of cortical remnants. [8, 9, 12] MRI findings and degree of confidence are similar to those of CT scanning (see CT Scan), although the improved soft-tissue contrast achieved with MRI allows for more confident identification of the falx and any residual supratentorial brain tissue.
Differentiating hydranencephaly from hydrocephalus and alobar holoprosencephaly in the prenatal period can be challenging. In difficult cases, prenatal MRI can be used to establish the correct diagnosis. In addition, if fetal ultrasonographic findings are equivocal, fetal MRI is useful for the accurate prenatal diagnosis of hydranencephaly. [8, 9, 13]
Ultrasonography
Most cases of hydranencephaly can be detected with prenatal ultrasonography, although fetal MRI may be necessary to confirm the diagnosis. [14, 15] If ultrasonography is performed before the etiologic insult, the initial study may be normal.
On prenatal ultrasound, an intact falx and a fluid-filled cranium can be seen. in newborns, macrocephaly and calvarial transillumination are present. The intact falx in hydranencephaly differentiates it from alobar holoprosencephaly. [10, 11]
Prenatal period
On ultrasonograms, hydranencephaly appears as a supratentorial fluid collection that replaces the cerebral hemispheres, with preserved, nonfused thalami and minimal (if any) preserved cerebral cortical tissue, usually in the occipital area. [16, 17] There is no uniform rim of preserved cerebral cortical tissue, as seen in fetal hydrocephalus. See the following images.
Ultrasonogram obtained at 14 weeks' gestation in a fetus with hydranencephaly shows unfused thalami surrounded by fluid. Note the lack of cerebral hemispheric tissue.
Sagittal image in a fetus with hydranencephaly at 14 weeks' gestation. This ultrasonogram demonstrates the absence of the cerebral hemispheres (which have been replaced by fluid). Because of the early age of gestation, hydranencephaly was difficult to distinguish from hydrocephalus. Hydranencephaly was confirmed on a level III ultrasonogram (not shown).
In cases caused by a massive intracranial hemorrhage, blood may initially be visualized as an echogenic mass in the supratentorial tissue. [18, 19] On sequential scans, blood evolves into an anechoic fluid collection that replaces the frontal and parietal lobes. In the early stages of hydranencephaly, the brain may appear heterogeneous, with multiple, small cystic areas seen; this appearance may mistakenly be attributed to intracranial teratoma. Using ultrasonographic images, Greene and colleagues described the in utero evolution of hydranencephaly in a fetus in which massive intracranial hemorrhage had been diagnosed at 27 weeks' gestation. [18]
Hydranencephaly versus alobar holoprosencephaly and hydrocephalus
When fetal ultrasonography is performed early in gestation, hydrocephalus and alobar holoprosencephaly can be difficult to distinguish from hydranencephaly.
Hydranencephaly and alobar holoprosencephaly should not be confused on high-resolution postnatal images or fetal MRIs. Alobar holoprosencephaly is characterized by the presence of a pancake-shaped mass of fused frontal lobe tissue, fusion of the thalami, and a large dorsal cyst. In hydranencephaly, there is no fusion of cerebral hemispheric tissue; indeed, little normal supratentorial tissue remains. The presence of a normal falx and the absence of thalamic fusion help to exclude holoprosencephaly. [16]
Differentiation from hydrocephalus is somewhat more difficult, because the rim of peripheral cerebral cortical tissue that is diagnostic of fetal hydrocephalus may be difficult or impossible to visualize with prenatal ultrasonography. In difficult cases, prenatal MRI can be used to establish the correct diagnosis (see MRI).
Postnatal period
Postnatally, cranial ultrasonography can detect the absence of cerebral tissue, differentiated from a lobar holoprosencephaly by the cleaved thalami and the presence of the falx cerebri. Because the brain beneath the fontanelle is clearly visible, THE absence of any cortical remnant at this level is helpful in the important differentiation of hydranencephaly from severe hydrocephalus. However, if the fontanelle is small or if appropriate high-frequency transducers are not available, it is possible in severe hydrocephalus to overlook a thin rim of cortical mantle.
No normal variants mimic hydranencephaly.
-
Ultrasonogram obtained at 14 weeks' gestation in a fetus with hydranencephaly shows unfused thalami surrounded by fluid. Note the lack of cerebral hemispheric tissue.
-
Sagittal image in a fetus with hydranencephaly at 14 weeks' gestation. This ultrasonogram demonstrates the absence of the cerebral hemispheres (which have been replaced by fluid). Because of the early age of gestation, hydranencephaly was difficult to distinguish from hydrocephalus. Hydranencephaly was confirmed on a level III ultrasonogram (not shown).
-
Axial computed tomography (CT) scan demonstrates an intact falx and separate thalami that suggest a diagnosis of hydranencephaly. Note the presence of the posterior fossa structures but the absence of the cerebral hemispheres.
-
Computed tomography (CT) scan in a patient in whom another CT scan demonstrated an intact falx and separate thalami that suggested a diagnosis of hydranencephaly. The image shown here demonstrates a complete absence of the cerebral hemispheres, with a small amount of occipital cortex remaining. The absence of a circumferential rim of residual cerebral hemispheric tissue eliminates hydrocephalus as a diagnostic consideration.



