Practice Essentials
Femoral neck fractures are serious injuries associated with a high mortality and significant morbidity in the geriatric population. The incidence has increased since the 1960s and is expected to continue to increase as life expectancies increase. [1, 2, 3] Despite advances in surgical hardware and techniques, these injuries still pose a significant clinical challenge. The primary complications arising from femoral neck fractures are nonunion and avascular necrosis (AVN).
Preferred examination
Radiography should always be the initial imaging modality. [4, 5] Then, depending on the clinical concern, additional studies can be obtained. In the American College of Radiology (ACR) Appropriateness Criteria, MRI is recommended if the presence of a fracture is equivocal on radiographs. [5] Nuclear medicine scintigraphy may also be appropriate. [6, 5] CT scanning may be useful if more osseous details (eg, degree of comminution and possible intra-articular bone fragments) are required. [7, 8, 9, 10]
Ten percent of all hip fractures are occult on plain radiography, requiring further investigation to ascertain the diagnosis. [11] Spiral fractures can be difficult to detect on a single view. Some stress fractures may not be seen at all. In general, nondisplaced or minimally displaced fractures are difficult to perceive on plain radiographs. Although MRI is considered the goal standard for evaluation of suspected fractures in patients with a negative or equivocal radiograh, surgery within 48 hours is associated with lower overall morbidity and mortality. Thus, if MRI is not available within 24 hours or is contraindicated, CT should be performed. [11, 5]
Ultrasonography does not play a significant role in the routine evaluation of hip fractures. However, this modality has been used in research to evaluate the degree of distention of the hip joint capsule after fractures and in the study of elevated intracapsular pressures. Sonograms can also depict the presence of an intracapsular hematoma, which is mildly echogenic, as distinguished from synovial fluid, which is anechoic.
Classification of fractures
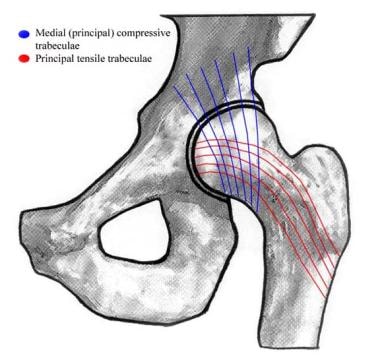
The Garden classification of subcapital femoral fractures is the most widely used today. This system is used to describe fractures on the basis of the distortions of the principal (medial) compressive trabeculae before reduction, as seen on anteroposterior (AP) radiographs. The anatomic basis of the Garden classification system is depicted in the illustration below. [12]
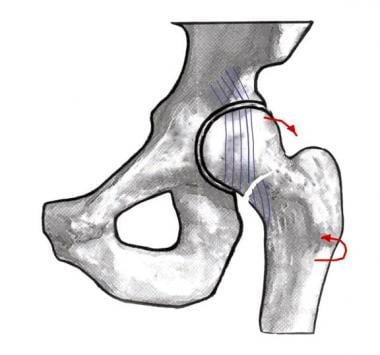
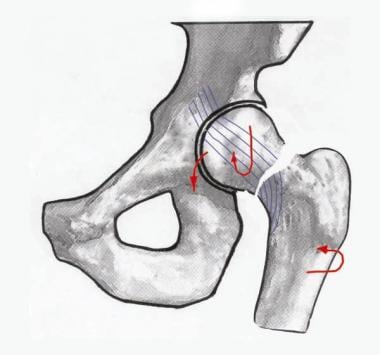
A stage I Garden fracture (seen in the images below) is an incomplete subcapital fracture. The femoral shaft is twisted externally. The alignment of the trabeculations of the distal femoral neck relative to the femoral head (which itself is adducted) causes the fracture to be in a valgus configuration. In other words, the trabecular markings in the femoral neck are displaced away from the midline relative to those in the femoral head. The altered angle of the trabeculations is greater than 180º when viewed on the AP projection (normally 160º). Such fractures are inherently stable.

 Magnetic resonance image of a Garden I hip fracture. Bone marrow edema is now present in the femoral neck on this short-tau inversion recovery (STIR) image.
Magnetic resonance image of a Garden I hip fracture. Bone marrow edema is now present in the femoral neck on this short-tau inversion recovery (STIR) image.
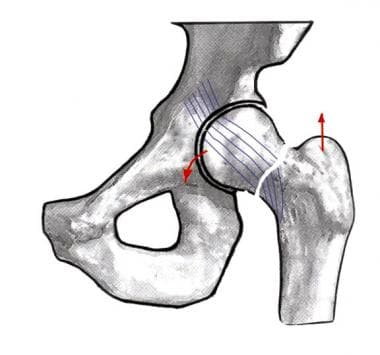
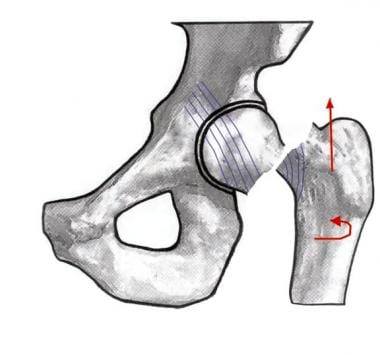
A stage II Garden fracture (seen in the images below) is a complete, but nondisplaced, fracture. The femoral head is abducted, but the femoral neck has moved in such a way as to maintain normal alignment with the femoral head. These fractures are considered stable and have a favorable prognosis.

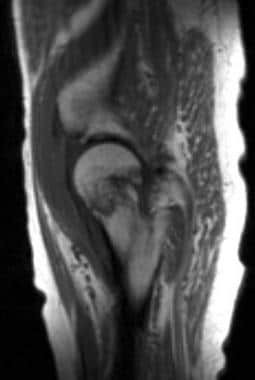 Sagittal T1-weighted magnetic resonance image of a Garden II hip fracture. This image demonstrates a low-signal-intensity line that passes through the femoral neck.
Sagittal T1-weighted magnetic resonance image of a Garden II hip fracture. This image demonstrates a low-signal-intensity line that passes through the femoral neck.
 Coronal short-tau inversion recovery (STIR) magnetic resonance image of a Garden II hip fracture. This image demonstrates bone marrow edema in the femoral neck, as well as edema in the adjacent muscles.
Coronal short-tau inversion recovery (STIR) magnetic resonance image of a Garden II hip fracture. This image demonstrates bone marrow edema in the femoral neck, as well as edema in the adjacent muscles.
A stage III Garden fracture (seen in the images below) is a complete, partially displaced subcapital fracture. The femoral shaft is externally rotated. The femoral head is abducted and axially rotated such that its superior surface resides more anteriorly. The alignment of the femoral neck relative to the head is in varus deformity.

A stage IV Garden fracture (seen in the images below) is a complete and fully displaced fracture. The femur is externally rotated and superiorly displaced relative to the femoral head. The head, now completely detached from the neck, remains in anatomic position relative to the acetabulum. This fracture is considered unstable with a poor prognosis.

Avascular necrosis staging
The most widely used classification system for AVN of the femoral head is the one proposed by Ficat and Arlet. [12, 13] This system is based on plain radiographic appearances, as follows:
-
Stage 0 has no radiographic findings. This preclinical stage is diagnosed by MRI or bone scanning.
-
Stage 1 manifests as slight osteoporosis on plain images. Clinical symptoms may be present, but sclerosis is not.
-
Stage 2 involves diffuse osteoporosis and sclerosis at the region of the infarction. The infarcted area is well delineated due to a reactive shell of bone. The spherical shape of the femoral head is maintained.
-
Stage 3 results in the crescent sign, or a radiolucency under the subchondral bone, which represents a fracture. The contour of the femoral head is abnormal. The joint space is preserved.
-
Stage 4 is characterized by femoral head collapse, joint-space narrowing, and subchondral sclerosis.
The Ficat-Arlet classification is especially pertinent in Garden III and IV fractures, in which there is a significant incidence of AVN.
Radiography
Radiography remains the first-line modality for imaging and classifying femoral neck fractures. Fractures can be broadly described according to their location along the femoral neck where the fracture line is located. Therefore, descriptive terms, such as subcapital, midcervical, and basicervical fractures of the neck are sometimes used. However, more specific descriptions are necessary, especially in relation to orthopedic management. Radiographs of Garden hip fractures I-IV are presented below. [9, 10]
Degree of confidence
Radiography is the preferred initial imaging modality for evaluating femoral neck fractures because of its near universal availability, its ease of acquisition, and its documented correlation with surgical results over many years of use. However, radiography has some limitations (as demonstrated in the image below). Spiral fractures are difficult to assess on a single view. Comminution is also not as easily demonstrated as it is with CT scanning. Some stress fractures are simply not visible on plain images.
 Radiograph with a poor depiction of an incomplete fracture of the left femoral neck.
Radiograph with a poor depiction of an incomplete fracture of the left femoral neck.
If the clinical suspicion for a femoral neck fracture is strong, even if it is not visible on radiographs obtained during the initial evaluation, the patient can be further evaluated with MRI, which shows bone marrow edema, or nuclear medicine bone scanning, which shows increased tracer uptake.
Computed Tomography
CT scanning plays an increasingly important role in the evaluation of the hip after a fracture. CT scanning is exquisitely useful for imaging abnormalities of the bone itself. Because of this modality's superior resolution, cross-sectional capabilities, and amenability to image reconstruction in the coronal and sagittal planes, CT scanning is useful for preoperatively assessing fracture comminution and in postoperatively determining the extent of union (or lack thereof). [8]
Although CT scanning is the most useful test for evaluating bony injury, axial fractures in the plane of the images can occasionally be missed. This potential risk is decreased with the use of images that are reconstructed in the orthogonal planes and with newer multidetector CT (MDCT) scanners.
Magnetic Resonance Imaging
MRI is sensitive and specific in the detection of femoral neck fractures, because this modality can show both actual fracture line and the resulting bone marrow edema (as demonstrated in the images below). [14, 7]
Magnetic resonance image of a Garden I hip fracture. Bone marrow edema is now present in the femoral neck on this short-tau inversion recovery (STIR) image.
Sagittal T1-weighted magnetic resonance image of a Garden II hip fracture. This image demonstrates a low-signal-intensity line that passes through the femoral neck.
Coronal short-tau inversion recovery (STIR) magnetic resonance image of a Garden II hip fracture. This image demonstrates bone marrow edema in the femoral neck, as well as edema in the adjacent muscles.
MRI is the premiere imaging modality, especially in the setting of stress fractures, which can appear normal on initial plain images, because of the superior contrast of MRI when appropriate pulse sequences are used, the modality's intrinsic spatial resolution, and MRI's ability to image in multiple planes (coronal, axial, and, less commonly, sagittal).
Popular pulse sequences include coronal and axial T1-weighted and T2-weighted fat-suppressed sequences, although several other bone marrow sequences can also be used. In practice, a large field of view is generally used so that both hips and the bony pelvis can be imaged simultaneously. Intravenous contrast enhancement is not routinely used in the assessment of fractures. The fracture line can be visualized as linear low-signal-intensity areas surrounded by bone marrow edema, which is hypointense relative to normal marrow on T1-weighted images or hyperintense on T2-weighted images.
The drawbacks of MRI include its longer imaging time, its relative lack of widespread availability, its higher costs, and the exclusion of patients with cardiac pacemakers and certain metal hardware in their body. With continued technological advances, however, the imaging time of MRI has decreased, as have the costs.
MRI is the most sensitive modality for detecting bone marrow changes that are related to AVN, even when radiographic findings are normal; therefore, MRI is the imaging modality of choice in this regard. When AVN is detected after surgical fixation for a femoral fracture, the patient can become a candidate for placement of a prosthesis. More importantly, MRI can be used to detect the early stages of ischemic necrosis in the femoral head, so that interventions can be initiated before further damage occurs, such as femoral head collapse, secondary osteoarthritis, and fragmentation.
Degree of confidence
MRI is currently the best imaging modality for detecting femoral neck fractures. Several facts must be kept in mind, however. The normal bone marrow of the pelvis and hips can have an appearance that is patchy and of intermediate signal intensity, corresponding to the persistence of red marrow. Also, the subchondral area of the femoral head can sometimes have a thin rim of red marrow. These normal variants should not be confused with fractures.
Fractures and contusions should not be confused with idiopathic transient osteoporosis of the hip. Transient osteoporosis is an uncommon, self-limited disease that affects middle-aged men and pregnant women. This condition appears as osteopenia on plain radiographs and as areas of decreased T1 signal intensity and increased T2 signal intensity that generally extend from the femoral head to the intertrochanteric line on MRI. Usually, only one hip is affected at a given time. To complicate matters, transient osteoporosis can predispose patients to a fracture if proper care (eg, protected weight bearing) is not implemented.
Nuclear Imaging
Approximately 80% of fractures can be visualized 24 hours after trauma, via diffusely increased tracer uptake. [15] By 3 days after trauma, 95% of fractures are visualized, and maximal fracture sensitivity is found at 7 days; this knowledge may be helpful in equivocal cases. Given the high sensitivity of nuclear medicine studies, they can be used to diagnose suspected femoral neck fractures that have not been confirmed by means of plain radiography.
(See the image below.)
 Bone scan of the left hip. This image shows increased uptake in the left femoral neck.
Bone scan of the left hip. This image shows increased uptake in the left femoral neck.
Bryant et al concluded that single-photon emission computed tomography (SPECT) scanning should be performed with planar bone scintigraphy for evaluation of suspected femoral neck stress fractures. The investigators compared the accuracy of planar scintigraphy alone with that of planar scintigraphy with SPECT for initial evaluation of femoral neck stress fractures in a young military population. They retrospectively identified 38 patients who had undergone planar scintigraphy and 33 patients who had undergone planar scintigraphy and SPECT before MRI of the hips. In the patients who underwent planar scintigraphy alone, 12 fractures were identified; in patients who underwent planar scintigraphy with SPECT, 13 fractures were identified. The sensitivity of planar scintigraphy alone was 50%, and its accuracy for high-grade fractures was 12.5%. When planar scintigraphy was combined with SPECT, sensitivity was 92.3%, and accuracy for high-grade fractures was 70%. [16]
When MRI is contraindicated, SPECT/CT can be used to assess blood supply within the femoral head after femoral neck fracture to help predict the occurrence of AVN. [17] SPECT/CT has 92% specificity and 77% sensitivity, which are comparable to that of MRI. [18]
Degree of confidence
Although sensitive, bone scintigraphy is not specific for fractures. Other processes, such as infection, inflammation, and tumor formation, can also demonstrate increased radionuclide uptake. However, in the right clinical setting (eg, known trauma), bone scintigraphy is highly sensitive for the detection of fractures.
-
Image depicting the trabecular system of the hip that is used in Garden staging.
-
Image depicting a Garden I hip fracture.
-
Image depicting a Garden II hip fracture.
-
Image depicting a Garden III hip fracture.
-
Image depicting a Garden IV hip fracture.
-
Radiograph demonstrating a Garden I hip fracture.
-
Magnetic resonance image of a Garden I hip fracture. Bone marrow edema is now present in the femoral neck on this short-tau inversion recovery (STIR) image.
-
Radiograph with a poor depiction of an incomplete fracture of the left femoral neck.
-
Bone scan of the left hip. This image shows increased uptake in the left femoral neck.
-
Radiograph depicting a Garden II hip fracture.
-
Sagittal T1-weighted magnetic resonance image of a Garden II hip fracture. This image demonstrates a low-signal-intensity line that passes through the femoral neck.
-
Coronal short-tau inversion recovery (STIR) magnetic resonance image of a Garden II hip fracture. This image demonstrates bone marrow edema in the femoral neck, as well as edema in the adjacent muscles.
-
Radiograph depicting a Garden III hip fracture.
-
Radiograph depicting a Garden IV hip fracture.









