Practice Essentials
Hepatocellular carcinoma (HCC) is a primary malignancy of the liver and occurs predominantly in patients with underlying chronic liver disease and cirrhosis, appearing 20-30 years following the initial insult to the liver. However, 25% of patients have no history of cirrhosis or risk factors for it. The extent of hepatic dysfunction limits treatment options, and as many patients die of liver failure as die from tumor progression. Tumors progress with local expansion, intrahepatic spread, and distant metastases. HCC generally leads to death within 6-20 months. [1, 2, 3]
(See the HCC images below.)
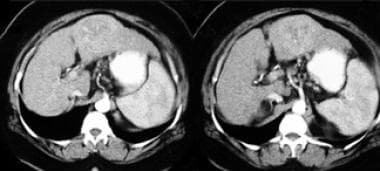 CT scan in the hepatic arterial phase of contrast enhancement showing neovascularity in a low-density hepatic mass.
CT scan in the hepatic arterial phase of contrast enhancement showing neovascularity in a low-density hepatic mass.
Preferred examination
Cross-sectional imaging with computed tomography (CT) scanning and magnetic resonance imaging (MRI) is most commonly used to detect hepatocellular carcinoma (HCC). CT scanning is frequently the first examination; however, MRI has superior contrast resolution and may better detect lesions less than 1 cm in diameter. Ultrasonography (US) can be sensitive in detecting HCC and, depending on the operator, can detect small lesions. US can evaluate for vascular invasion of the portal and hepatic veins through color Doppler imaging. Nuclear medicine imaging, angiography, and plain films are less useful. [4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15]
CT scanning should be performed in hepatic arterial, portal venous, and delayed phases. Similarly, if MRI is used, precontrast, arterial, venous, and delayed phases are essential. Enhancement patterns of regenerative, dysplastic, and HCC nodules overlap; therefore, nodules of cirrhosis may not be differentiated from small HCCs.
Nonspecific findings on plain film are standard. An abdominal mass may be visible. Plain films amay show a mass in the upper abdomen if the HCC is large. Calcification is rare in HCC but is more frequent in other hepatic masses, such as fibrolamellar HCC. Patients with hemochromatosis as a predisposing factor in the development of HCC may show deposition of calcium pyrophosphate in the cartilage of joints. Many other causes of chondrocalcinosis exist, such as gout, hyperparathyroidism, Wilson disease, and degenerative joint disease.
Nuclear imaging provides relatively nonspecific findings. The HCC may present as a "cold" defect on a sulfur-colloid study or may demonstrate uptake of radiopharmaceuticals if the mass produces bile. Gallium uptake is seen in 90% of HCCs. The US appearance of HCC varies; it may be hyperechoic or hypoechoic. A small hyperechoic HCC may be confused with hemangioma.
Angiography may show increased vascularity of other hepatic tumors, including benign masses.
Guidelines
According to the National Comprehensive Cancer Network (NCCN), screening and surveillance for HCC is considered cost-effective in patients with cirrhosis or chronic hepatitis B. The NCCN recommended ultrasonography with or without α-fetoprotein (AFP). If ultrasonography-detected nodules are negative, testing should be repeated in 6 months. If the nodules are small (< 10 mm), repeat in 3 to 6 months. For patients who have a positive AFP test result or have large nodules (≥10 mm) or have capsular retraction or vascular invasion, further imaging with computed tomography (CT) or MRI allows for a definitive diagnosis. [16]
The American Association for the Study of Liver Diseases (AASLD) guidelines, like NCCN, recommend routine screening for HCC in adults with cirrhosis. The initial screening is performed with ultrasound with or without alpha- fetoprotein (AFP) every 6 months. Unlike NCCN, there are no recommendations for screening and surveillance of HCC in noncirrhotic patients. [17]
In adults with cirrhosis and suspected HCC, the AASLD recommends diagnostic evaluation with either multiphasic CT or multiphasic MRI. The selection of the optimal modality and contrast agent for a particular patient depends on multiple factors beyond diagnostic accuracy. These include modality availability, scan time, throughput, scheduling backlog, institutional technical capability, examination costs and charges, radiologist expertise, patient preference, and safety considerations. [17]
The American College of Radiology (ACR) imaging guidelines acknowledge that all international organizations recommend ultrasonography to screen for HCC, however, the ACR notes that this modality is particularly limited for identifying HCC in patients with obesity, nonalcoholic fatty liver disease (NAFLD), and nodular cirrhotic livers. According to the ACR, in these patient groups, as well as in patients who are on the liver transplant wait list, ultrasonography is so limited that consideration should be made for screening for HCC with either MRI or multiphase CT. [18, 19]
The ACR guidelines also state that if a suspicious liver lesion greater than 1 cm is identified on ultrasound, the diagnosis must be confirmed by MRI or multiphase CT. MRI is preferable because of its slightly increased accuracy over CT and because MRI can detect premalignant nodules. However, multiphase CT can accurately diagnose HCC as well. [18] The guidelines also note that patients who have been previously diagnosed with and treated for HCC require continued surveillance for recurrent HCC. Multiphase CT or MRI is recommended to assess response 1 month after resection or therapy, followed by imaging every 3 months for at least 2 years. [18]
The Liver Image Reporting Data System (LIRADS) was created to standardize the acquisition, interpretation, reporting, and data collection of HCC cases. LIRADS advocates using multiphase CT or MRI, as well as US. [3]
Computed Tomography
Proper technical performance of CT scanning with imaging in the hepatic arterial and portal venous phases, as well as delayed contrast images, is important in detecting hepatocellular carcinoma (HCC). Lesions may be missed if early vascular imaging is not performed. It is important to use high injection rates and appropriate bolus timing. Sensitivity of good-quality dual- or triple-phase CT scanning for the detection of patients with tumors is 60-70%. [10, 16, 17, 18, 20, 21]
The CT appearance of HCC varies depending on tumor size and the imaging phase. The most common attenuation pattern is iso-hyper-isoattenuation on prephase, arterial phase, and venous phase, respectively; however, this pattern is shared by other hepatocellular nodules, including regenerative and dysplastic nodules.
Unenhanced CT typically reveals an iso-hypodense mass. If the mass is large, central areas of necrosis may be seen. Look for signs of cirrhosis or hemochromatosis.
In the hepatic arterial phase (seen in the image below), lesions typically are hyperdense (relative to hepatic parenchyma) as a result of hepatic arterial supply. Larger tumors may have necrotic central regions that are typically hypodense during this imaging phase. Look for neovascularity to indicate the presence of inconspicuous lesions.
CT scan in the hepatic arterial phase of contrast enhancement showing neovascularity in a low-density hepatic mass.
In the portal venous phase, small lesions may be isodense or hypodense and difficult to see, since the remainder of the liver increases in attenuation. Larger lesions with necrotic regions remain hypodense.
In the delayed-postcontrast phase, small lesions may be inconspicuous on late phases. Delayed phase scans may show a tumor capsule, which is one of the more specific signs of HCC.
CT can also evaluate complications of HCC, such as portal venous or hepatic venous invasion. In addition, be alert and evaluate for other complications such as bleeding within the tumor and hemoperitoneum.
Evaluate underlying disease on CT, which can indicate the etiology of a hepatic mass. Look for signs of cirrhosis and hemochromatosis.
Cirrhotic nodules cannot be reliably differentiated from small HCCs. Since success of therapy depends on early HCC detection, the distinction is important; MRI can assist with nodule differentiation.
False-negative CT imaging can occur. Even the best CT scanner may have difficulty detecting small lesions, especially if good-quality, triphasic scanning is not performed. Prospective detection rates of tumors and tumor nodules were reported as 59% and 37%, respectively, in a large series with pathologic correlation. [21]
In the setting of an abnormal liver with elevated alpha-fetoprotein (AFP), a vascular mass or a large necrotic mass strongly suggests HCC; however, other hepatic lesions, benign or malignant, can mimic HCC on CT. MRI or nuclear imaging can assist in this differentiation.
Magnetic Resonance Imaging
Hepatocellular carcinoma (HCC) appearance varies on MRI depending on multiple factors, such as hemorrhage, degree of fibrosis, histologic pattern, degree of necrosis, and the amount of fatty change. HCC on T1-weighted images may be isointense, hypointense, or hyperintense relative to the liver. On T2-weighted images, HCC is usually hyperintense. Precontrast and postcontrast MRI has a 70-85% chance of detecting a solitary mass of HCC. [5, 8, 10, 16, 17, 18, 22]
MRI can help differentiate cirrhotic nodules from HCC as follows:
-
If the mass is bright on T2-weighted images, it is HCC until proven otherwise.
-
If the mass is dark on T1- and T2-weighted images, it is a siderotic regenerative nodule or siderotic dysplastic nodule.
-
If the mass is bright on T1-weighted images and dark or isointense on T2-weighted images, it is a dysplastic nodule or low-grade HCC.
On T2-weighted images, HCC generally demonstrates high signal intensity. [23]
Gadolinium-enhanced MRI typically demonstrates that HCCs densely enhance, usually in the arterial phase, particularly if they are small. A lesion showing arterial enhancement is most likely HCC; however, dysplastic nodules and, less likely, regenerative nodules can show similar enhancement. The degree of enhancement varies, particularly with the degree of necrosis in larger tumors. Look carefully for enhancement in small portions of tumor. (In addition, a "flash filling" hemangioma can have rapid arterial enhancement but could be differentiated by lack of washout on delayed images.)
Administration of superparamagnetic iron oxide may demonstrate HCC, because most HCCs contain fewer or no Kupffer cells.
The contrast agent mangafodipir trisodium can evaluate questionable lesions in the liver. Mangafodipir trisodium is taken up by normal hepatocytes and masses that contain hepatocytes, causing increased signal intensity on T1-weighted images. This agent may help differentiate a tumor of hepatocellular origin, such as HCC, from secondary hepatic masses.
Complications (eg, vascular invasion) are evaluated well by MRI.
Gadolinium-based contrast agents have been linked to the development of nephrogenic systemic fibrosis (NSF) or nephrogenic fibrosing dermopathy (NFD). The disease has occurred in patients with moderate to end-stage renal disease after being given a gadolinium-based contrast agent to enhance MRI or MRA scans. NSF/NFD is a debilitating and sometimes fatal disease. Characteristics include red or dark patches on the skin; burning, itching, swelling, hardening, and tightening of the skin; yellow spots on the whites of the eyes; joint stiffness with trouble moving or straightening the arms, hands, legs, or feet; pain deep in the hip bones or ribs; and muscle weakness.
Some well-differentiated HCCs can mimic cirrhotic nodules on MRI.
Some HCCs can contain Kupffer cells, thus having signal characteristics similar to those of normal liver tissue on images contrasted with superparamagnetic iron oxide.
Ultrasonography
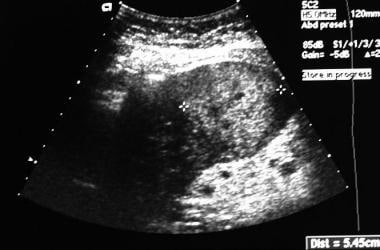
US appearance of hepatocellular carcinoma (HCC) is variable. Note that the quality of a US examination is operator dependent. Take care to evaluate the entire liver completely because it is not difficult to overlook a small hepatic mass. Small HCCs can be homogeneously hyperechoic and can mimic hemangioma. This can result from a large proportion of fat being present in the tumor. Small HCCs also can appear hypoechoic, with larger HCCs frequently mixed in echogenicity.Good-quality US with careful evaluation of the entire liver can, in combination with serum alpha-fetoprotein (AFP) evaluation, be a screening examination for HCC in patients at risk; however, sensitivity of US for the detection of lesions in a cirrhotic liver is limited. [8, 10, 16, 17, 18, 24, 25, 26, 27]
(See the image below.)
The FDA approved sulfur hexafluoride (Lumason) for ultrasonography of the liver in adults and children to enhance the characterization of focal liver lesions. Contrast-enhanced ultrasound (CEUS) greatly improved diagnosis as compared to ultrasound without contrast. In one study, CEUS allowed a correct diagnosis in more than 80% of focal liver lesions and led to a change in the diagnostic workup in 131/157 patients (83.4%) and in the therapeutic workup in 93/157 patients (59.2%). [27]
One retrospective review of patients with HCC found that almost half of HCCs had posterior acoustic enhancement to some degree. This may be linked to the tissue characteristics of the tumor or the cirrhotic liver itself. During sonographic screening, focusing on this finding, including scanning without spatial compounding, is advised. [28]
Vascular invasion can be adequately evaluated using color Doppler imaging with conventional gray-scale US. Look for tumor thrombus in hepatic and portal veins as well as in the inferior vena cava. Portal venous invasion is more common in HCC, but hepatic vein invasion is more specific for HCC.
In particular, small hyperechoic masses seen on US require further evaluation because they can represent hemangioma (most commonly), metastatic disease or, less likely, HCC. Further imaging with CT scanning or MRI during dynamic contrast enhancement shows the typical peripheral, nodular contrast enhancement pattern of hemangioma. MRI or CT scanning can further characterize many nonspecific hepatic masses seen on US.
Some studies have reported US as having a 60% sensitivity and a 97% specificity in patients with cirrhosis [11, 29]
A meta-analysis by Hanna et al found that CEUS had a sensitivity of 84.4% and a positive predictive value of 89.3% for detection of HCC. [30]
The ACR released the Ultrasound Liver Imaging Reporting Data System (LI-RADS) algorithm to classify lesions at risk of HCC as investigated by CEUS. [19, 31]
Nuclear Imaging
On a gallium scan, up to 90% of hepatocellular carcinomas (HCCs) demonstrate uptake of the radiopharmaceutical. Gallium may help distinguish regenerating nodules of cirrhosis from HCC, as regenerating nodules typically do not label with gallium.
On a liver-spleen scan, a sulfur-colloid study typically demonstrates an area of decreased labeling in HCC. Look for signs of cirrhosis, such as heterogeneous labeling of the liver with a large spleen and colloid shift to the bone marrow. Prominent left and caudate lobes of the liver are also signs of cirrhosis. A "cold" defect in the liver with signs of cirrhosis strongly suggests HCC.
Hepatobiliary scans can show labeling of HCC due to the presence of hepatocytes. HCC may have no uptake initially but may show delayed uptake as the rest of the normal liver clears. This is related to malignant hepatocytes, which are hypofunctional relative to normal hepatocytes.
Positron emission tomography with fluorodeoxyglucose (FDG-PET) is primarily useful in assessing the degree of differentiation and in staging moderately and poorly differentiated tumors, rather than in primary lesion detection. Sensitivity of FDG-PET for the detection of HCC is 50-70%. This limited sensitivity is due to the low level of FDG uptake in well-differentiated tumors; however, FDG-PET may be superior to CT in detecting extrahepatic spread.
On a gallium scan, the liver normally labels early and may obscure HCC labeling. Differential diagnoses of a mass that shows labeling in the liver include other types of malignancy and infection.
Questions & Answers
Overview
What is hepatocellular carcinoma (HCC)?
Which imaging modalities are used in the workup of hepatocellular carcinoma (HCC)?
What are the imaging guidelines for hepatocellular carcinoma (HCC)?
What is the role of CT scanning in the workup of hepatocellular carcinoma (HCC)?
What is the role of MRI in the workup of hepatocellular carcinoma (HCC)?
What is the role of ultrasonography in the workup of hepatocellular carcinoma (HCC)?
What is the role of nuclear imaging in the workup of hepatocellular carcinoma (HCC)?
-
CT scan in the hepatic arterial phase of contrast enhancement showing neovascularity in a low-density hepatic mass.
-
Ultrasound shows hyperechoic mass representing hepatocellular carcinoma.







