Practice Essentials
Hepatoblastoma is the most common malignant liver tumor in early childhood. Most patients present before the age of 3 years with an enlarging asymptomatic abdominal mass. Some patients have fever, pain, anorexia, and weight loss. The 2 most important genetic conditions associated with hepatoblastoma are Beckwith-Wiedemann syndrome and familial adenomatous polyposis. [1, 2, 3, 4, 5, 6] The incidence of hepatoblastoma in familial adenomatous polyposis kindreds is 200-800 times greater than that in the general population.
There are 2 histologic types: epithelial and mixed. Neoadjuvant chemotherapy is the standard of care for most cases, along with surgical resection, with cure rate being about 70%. A third of cases may be associated with Beckwith-Weidemann syndrome, familial adenomatous polyposis, and Edward syndrome (trisomy 18). [1]
The results of a large population-based study found children with several forms of nonchromosomal congenital heart disease were at increased risk for hepatoblastoma. In addition, the study's findings confirmed an association seen in earlier trials between hepatoblastoma and trisomy 18. [7]
Evidence also exists of an association between hepatoblastoma and maternal exposure to metals, paints, and oil products. A significant number of patients with hepatoblastoma (10%) have a history of prematurity with prolonged hospitalization. Unlike hepatocellular carcinoma, hepatoblastoma has no association with cirrhosis.
Imaging modalities
For evaluation of the primary tumor, MRI is the preferred imaging modality. Because of the orthogonal-imaging capability of MRI, it is superior to CT in defining tumor margins and determining tumor resectability. [8, 9] However, 3-dimensional CT-reconstructed images may compare favorably to MRI. Magnetic resonance angiography (MRA) can evaluate the tumor blood supply, which is valuable information for surgical planning. Postoperatively, MRI is superior to CT in detecting residual or recurrent tumor in the surgical bed. CT is the imaging modality of choice for detecting pulmonary metastases. [10, 11, 12, 13, 14, 15, 16, 17, 18]
The PRETEXT (PRE-Treatment EXTent of tumor) system is considered the primary method of risk stratification. It consists of the PRETEXT group and the annotation factors. The PRETEXT group describes the extent of tumor in the liver, and the annotation factors help describe features such as vascular involvement, extrahepatic disease, multifocality, tumor rupture and metastatic disease. [19]
One limitation of MRI is that patients with hepatoblastoma typically require sedation for the procedure because they are young. The value of MRI also may be limited by breathing motion. However, diagnostic-quality, standard-sequence MRI now can be performed in breathing-sedated patients. Rapid-scanning techniques allow diagnostic-quality MRI and MRA in breathing-sedated patients and in those capable of only limited cooperation.
Conversely, helical CT imaging of both the chest and abdomen can be performed quickly, easily, and usually without sedation. [20] However, CT may not be as accurate as MRI in defining tumor margins, evaluating the portal vein, or detecting residual or recurrent tumor following surgery.
(See the image below.)
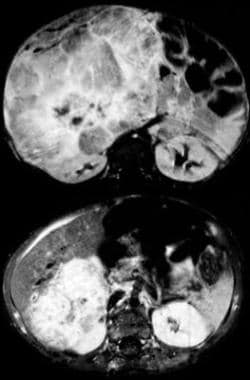 Contrast-enhanced, fat-suppressed, axial, T-1 weighted MRI (conventional spin echo [CSE]: 800/14) of an 8-month-old boy with hepatoblastoma before (top) and after (bottom) chemotherapy (vincristine, carboplatin, 5-fluorouracil). Approximately 70% of hepatoblastomas are unresectable at initial presentation. Current chemotherapy methods can convert approximately 75% of these tumors to a resectable condition.
Contrast-enhanced, fat-suppressed, axial, T-1 weighted MRI (conventional spin echo [CSE]: 800/14) of an 8-month-old boy with hepatoblastoma before (top) and after (bottom) chemotherapy (vincristine, carboplatin, 5-fluorouracil). Approximately 70% of hepatoblastomas are unresectable at initial presentation. Current chemotherapy methods can convert approximately 75% of these tumors to a resectable condition.
Radiography
Abdominal radiography may show hepatomegaly as evidenced by elevation of the right hemidiaphragm and displacement of bowel gas. Although they are not diagnostically specific, hepatic calcifications may be present. Chest radiography may demonstrate pulmonary metastases and can aid in the differential diagnosis. The degree of confidence is low. Plain films cannot localize the tumor to the liver definitively, distinguish between the solid or cystic nature of a neoplasm, or provide information regarding tumor vascularity. A normal abdominal plain film cannot exclude hepatoblastoma.
(See the image below.)
 Anteroposterior view of the right shoulder demonstrates a metastatic deposit in the proximal humeral metadiaphysis in an 11-year-old girl with hepatoblastoma. Bone is the second most common site of metastatic disease from hepatoblastoma.
Anteroposterior view of the right shoulder demonstrates a metastatic deposit in the proximal humeral metadiaphysis in an 11-year-old girl with hepatoblastoma. Bone is the second most common site of metastatic disease from hepatoblastoma.
Computed Tomography
Appearance of hepatoblastoma on CT varies greatly. Prior to contrast administration, an epithelial-type tumor appears as a homogeneous hypodense mass, while a mixed mesenchymal-epithelial tumor demonstrates a more heterogeneous appearance. [21] Calcifications may be present in either type: small and fine in the epithelial type and coarse and extensive in the mixed type.
Following the injection of IV contrast, some enhancement of the tumor is seen, usually less than in normal liver tissue (see the CT images below). The enhancement pattern typically is inhomogeneous, and a peripheral rim of enhancement may be observed if imaging is performed during the early arterial phase. If peripheral enhancement is seen, perform delayed serial scans at a single level of the tumor to distinguish hepatoblastoma from hemangioendothelioma. The tumor may involve 1, 2, or 3 segments or may diffusely involve the entire liver.
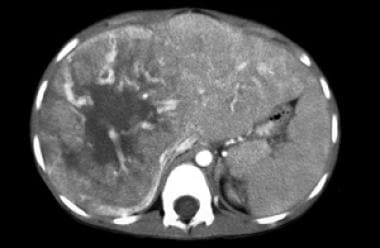 Contrast-enhanced CT of a 7-year-old boy with hepatoblastoma. Large feeding vessels lead to the tumor. Large central area of necrosis is not unusual for hepatoblastoma, especially the anaplastic type.
Contrast-enhanced CT of a 7-year-old boy with hepatoblastoma. Large feeding vessels lead to the tumor. Large central area of necrosis is not unusual for hepatoblastoma, especially the anaplastic type.
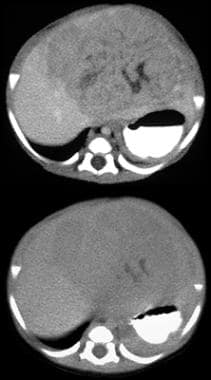 Immediate (top) and delayed (bottom) contrast-enhanced CT of a 1-month-old boy with hepatoblastoma. The immediate image shows inhomogeneous contrast enhancement with focal unenhanced areas consistent with necrosis. Most hepatoblastomas enhance less than the surrounding normal liver, as seen in this patient. The delayed image shows washout of contrast material from the tumor.
Immediate (top) and delayed (bottom) contrast-enhanced CT of a 1-month-old boy with hepatoblastoma. The immediate image shows inhomogeneous contrast enhancement with focal unenhanced areas consistent with necrosis. Most hepatoblastomas enhance less than the surrounding normal liver, as seen in this patient. The delayed image shows washout of contrast material from the tumor.
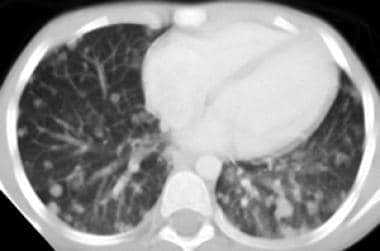 CT of the chest demonstrates diffuse bilateral pulmonary metastases in a 7-year-old boy with hepatoblastoma. The lungs are the most common site of metastatic disease in patients with hepatoblastoma and are involved in 10% of patients at diagnosis.
CT of the chest demonstrates diffuse bilateral pulmonary metastases in a 7-year-old boy with hepatoblastoma. The lungs are the most common site of metastatic disease in patients with hepatoblastoma and are involved in 10% of patients at diagnosis.
The degree of confidence is moderate. Tumor margins and segmental involvement may be difficult to determine. The status of the portal vein may be difficult to assess, and the selective use of ultrasonography (US), Doppler US, MRI, or MRA may be necessary. CT cannot differentiate hepatoblastoma from hepatocellular carcinoma. The patient's age is the most important criterion for differentiating these tumors; patients younger than 5 years are more likely to have hepatoblastoma; those older than 5 years are more likely to have hepatocellular carcinoma.
False-negative images for tumor recurrence may be observed following tumor resection. In addition, CT of both the abdomen and chest may fail to recognize neoplasm when rising serum AFP levels are seen until a sufficient volume of disease is present. In these patients, recurrent tumor usually becomes evident on follow-up imaging.
Magnetic Resonance Imaging
Similar to CT, the MRI appearance of hepatoblastoma varies with its histologic nature. The epithelial type has a homogeneous appearance and is hypointense on T1-weighted images and hyperintense on T2-weighted images. The mixed type is more heterogeneous, depending on the presence of necrosis, hemorrhage, fibrosis, calcification, cartilage, and septa.
(See the MRIs of hepatoblastoma below.)
Contrast-enhanced, fat-suppressed, axial, T-1 weighted MRI (conventional spin echo [CSE]: 800/14) of an 8-month-old boy with hepatoblastoma before (top) and after (bottom) chemotherapy (vincristine, carboplatin, 5-fluorouracil). Approximately 70% of hepatoblastomas are unresectable at initial presentation. Current chemotherapy methods can convert approximately 75% of these tumors to a resectable condition.
 Contrast-enhanced 3-dimensional MR angiogram (gradient echo [GRE]:6.2/2.2) of a 16-month-old boy with hepatoblastoma. Portal venous-phase image clearly demonstrates normal portal-venous anatomy.
Contrast-enhanced 3-dimensional MR angiogram (gradient echo [GRE]:6.2/2.2) of a 16-month-old boy with hepatoblastoma. Portal venous-phase image clearly demonstrates normal portal-venous anatomy.
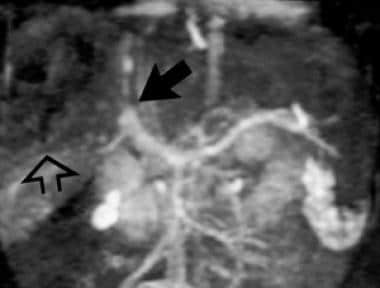 Contrast-enhanced 3-dimensional MR angiogram (gradient echo [GRE]:5/2) of a 2-year-old girl with hepatoblastoma. Portal-venous-phase image demonstrates the dark tumor in the right lobe of the liver (open arrow) that compresses and obstructs the right portal vein (closed arrow). There is no thrombus within the portal vein.
Contrast-enhanced 3-dimensional MR angiogram (gradient echo [GRE]:5/2) of a 2-year-old girl with hepatoblastoma. Portal-venous-phase image demonstrates the dark tumor in the right lobe of the liver (open arrow) that compresses and obstructs the right portal vein (closed arrow). There is no thrombus within the portal vein.
Septations appear as hypointense bands on both T1- and T2-weighted images. Vascular invasion is demonstrated best by gradient-echo MRI or contrast-enhanced MRA (see the image below).
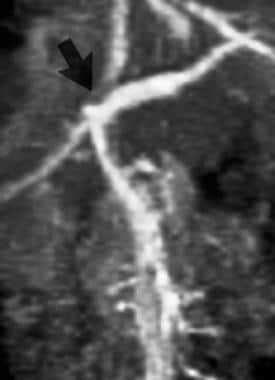 Contrast-enhanced 3-dimensional MR angiogram (gradient echo [GRE]:5/2) of a 9-year-old girl with hepatoblastoma. Venous-phase image demonstrates occlusion of the right portal vein and a filling defect in the proximal left portal vein suggestive of tumor thrombus. Tumor thrombus in this location was proven at surgery. Courtesy of Fredric Hoffer, MD, St. Jude Children's Research Hospital, Memphis, Tenn.
Contrast-enhanced 3-dimensional MR angiogram (gradient echo [GRE]:5/2) of a 9-year-old girl with hepatoblastoma. Venous-phase image demonstrates occlusion of the right portal vein and a filling defect in the proximal left portal vein suggestive of tumor thrombus. Tumor thrombus in this location was proven at surgery. Courtesy of Fredric Hoffer, MD, St. Jude Children's Research Hospital, Memphis, Tenn.
Three-dimensional contrast-enhanced MRA also can be performed to assess tumor blood supply and to evaluate for the presence of normal-variant vascular anatomy (see the images below). [22]
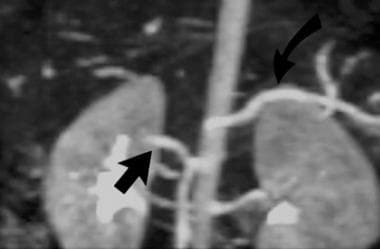 Contrast-enhanced 3-dimensional MR angiogram (gradient echo [GRE]:5/2) of a 3-year-old girl with hepatoblastoma. Arterial-phase image demonstrates a replaced right hepatic artery (straight arrow) originating from the superior mesenteric artery. The splenic artery, originating from the celiac axis, also is demonstrated. Information about the vascular anatomy is crucial for surgical planning. Courtesy of Fredric Hoffer, MD, St. Jude Children's Research Hospital, Memphis, Tenn.
Contrast-enhanced 3-dimensional MR angiogram (gradient echo [GRE]:5/2) of a 3-year-old girl with hepatoblastoma. Arterial-phase image demonstrates a replaced right hepatic artery (straight arrow) originating from the superior mesenteric artery. The splenic artery, originating from the celiac axis, also is demonstrated. Information about the vascular anatomy is crucial for surgical planning. Courtesy of Fredric Hoffer, MD, St. Jude Children's Research Hospital, Memphis, Tenn.
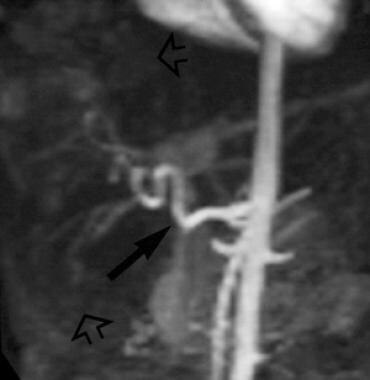 Contrast enhanced 3-dimensional MR angiogram (gradient echo [GRE]:5/2) of a 9-year-old girl with hepatoblastoma. The hepatoblastoma is located in the right lobe of the liver and is supplied by the right hepatic artery. MR angiogram demonstrates enlarged and tortuous common, proper, and right hepatic arteries. Courtesy of Fredric Hoffer, MD, St. Jude Children's Research Hospital, Memphis, Tenn.
Contrast enhanced 3-dimensional MR angiogram (gradient echo [GRE]:5/2) of a 9-year-old girl with hepatoblastoma. The hepatoblastoma is located in the right lobe of the liver and is supplied by the right hepatic artery. MR angiogram demonstrates enlarged and tortuous common, proper, and right hepatic arteries. Courtesy of Fredric Hoffer, MD, St. Jude Children's Research Hospital, Memphis, Tenn.
The combination of MRI and contrast-enhanced MRA provides the surgeon with complete information for operative planning of partial hepatectomy or orthotopic liver transplantation.
The degree of confidence is high. MRI appearance of hepatoblastoma is unlike common infantile hemangioma (the other primary liver tumor in this age group), because hepatoblastoma usually lacks enlarged feeding hepatic arteries and draining veins. The infantile hemangioma, if extensive, may exhibit multiple lesions in the liver and soft tissues. The child may exhibit cardiomegaly and overcirculation or even congestive heart failure.
The Kaposiform hemangioendothelioma that produces a consumptive coagulopathy may be a single lesion and is more difficult to distinguish from hepatoblastoma because no arteriovenous (AV) shunting may be present. MRI is superior to CT in determining tumor margins and portal vein invasion. However, MRI cannot detect pulmonary nodules with confidence. CT remains the most sensitive imaging screening test for this purpose.
MRI appearance of hepatoblastoma may mimic embryonal sarcoma and fibrolamellar hepatocellular carcinoma, which are more likely to occur in older teenagers. The embryonal sarcoma may have a distinctive pattern of central necrosis and hemorrhage with a rim of viable tissue of varying thickness. Fibrolamellar hepatocellular carcinoma may have a fibrous center, benign regional reactive lymphadenopathy, and an indolent course.
Gadolinium-based contrast agents have been linked to the development of nephrogenic systemic fibrosis (NSF) or nephrogenic fibrosing dermopathy (NFD). NSF/NFD has occurred in patients with moderate to end-stage renal disease after being given a gadolinium-based contrast agent to enhance MRI or MRA scans. Characteristics include red or dark patches on the skin; burning, itching, swelling, hardening, and tightening of the skin; yellow spots on the whites of the eyes; joint stiffness with trouble moving or straightening the arms, hands, legs, or feet; pain deep in the hip bones or ribs; and muscle weakness.
Ultrasonography
On US, hepatoblastoma may appear as a solitary mass, a dominant mass with smaller satellite lesions, or multiple nodules throughout the liver. [23] Rarely, hepatoblastoma may infiltrate the entire liver. Most tumors have some hyperechoic areas relative to normal liver, often with some inhomogeneity resulting from the presence of mesenchymal elements. Calcifications may be present and appear as brightly echogenic punctate or linear foci with acoustic shadowing. Portal vein invasion is seen as echogenic intraluminal thrombus. Areas of necrosis and hemorrhage appear as anechoic foci.
The degree of confidence is low. The patient's age helps narrow the differential diagnosis. Prenatal diagnosis is possible, but hepatoblastoma must be distinguished from hepatic hemangioma. Diagnosis must be confirmed postnatally with CT and liver biopsy. [24]
Findings on US are nonspecific and may be seen with other primary malignant neoplasms, metastatic disease, abscesses, and benign vascular lesions. However, US is useful as a preliminary imaging study and usually determines the tumor's organ of origin. This is aided by watching the tumor in real time with normal respirations and detecting motion between the tumor and the noninvolved organs. US can be performed quickly, does not require sedation, is relatively inexpensive, and does not involve ionizing radiation. Doppler sonography may detect neovascularity around the rim of the neoplasm with high velocity and low-resistance vasculature.
The presence of high-velocity Doppler signals within a mass and invasion of the portal vein strongly support the diagnosis of malignant neoplasm. Common infantile hemangioma may be distinguished from hepatoblastoma by the presence of enlargement of the hepatic artery and a tapering of the aortic dimension distal to the celiac axis. Often, it is difficult to assess tumor margins accurately by US, although in the future, this limitation may be overcome by US contrast agents (see the image below).
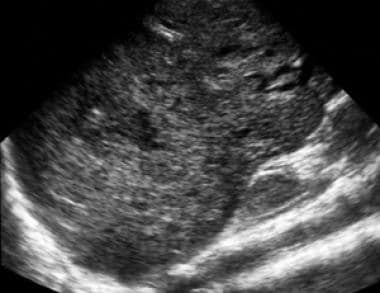 Longitudinal ultrasound image of the right lobe of the liver demonstrates diffuse heterogeneity of the liver parenchyma in this 8-year-old boy with hepatoblastoma. Note the difficulty in determining the tumor's margins by ultrasound.
Longitudinal ultrasound image of the right lobe of the liver demonstrates diffuse heterogeneity of the liver parenchyma in this 8-year-old boy with hepatoblastoma. Note the difficulty in determining the tumor's margins by ultrasound.
Nuclear Imaging
On technetium-99m sulfur-colloid liver scintigraphy, hepatoblastomas usually demonstrate hypervascularity, with prominent tracer avidity at the site of the tumor within a few seconds of the appearance of the bolus in the abdominal aorta. [25] This increased activity persists into the venous phase.
Delayed images typically demonstrate a photopenic defect at the tumor site from replacement of Kupffer cells by the tumor. Less commonly, in tumors containing large foci of necrosis, a photopenic defect is seen on both the static and dynamic portions of the examination. Rarely, hepatoblastomas may demonstrate increased uptake on delayed imaging.
The degree of confidence is low. Findings seen with hepatoblastoma usually are indistinguishable from those observed with hepatocellular carcinoma, embryonal sarcoma, and other malignant liver tumors. A liver lesion must be at least 1.5-2.0 cm to be detected by planar scintigraphy. Detection of smaller lesions with single photon emission computed tomography (SPECT) is possible but not practical in this entity.
Angiography
Historically, the role of angiography has been to demonstrate normal and variant vascular anatomy (eg, a replaced right hepatic artery), tumor vascularity, segmental and lobar extent of tumor, and potential for surgical resection. Venous-phase arteriography also has demonstrated the portal vein and defined tumor thrombus. These questions usually can be answered accurately with MRI and 3-dimensional contrast-enhanced MRA or at times by CT or US. Therefore, hepatic angiography is now reserved for patients in whom noninvasive cross-sectional images fail to demonstrate crucial anatomy prior to resection or transplantation. The degree of confidence is high for demonstrating vascular anatomy and segmental involvement by tumor.
-
Contrast-enhanced, fat-suppressed, axial, T-1 weighted MRI (conventional spin echo [CSE]: 800/14) of an 8-month-old boy with hepatoblastoma before (top) and after (bottom) chemotherapy (vincristine, carboplatin, 5-fluorouracil). Approximately 70% of hepatoblastomas are unresectable at initial presentation. Current chemotherapy methods can convert approximately 75% of these tumors to a resectable condition.
-
Contrast-enhanced 3-dimensional MR angiogram (gradient echo [GRE]:5/2) of a 3-year-old girl with hepatoblastoma. Arterial-phase image demonstrates a replaced right hepatic artery (straight arrow) originating from the superior mesenteric artery. The splenic artery, originating from the celiac axis, also is demonstrated. Information about the vascular anatomy is crucial for surgical planning. Courtesy of Fredric Hoffer, MD, St. Jude Children's Research Hospital, Memphis, Tenn.
-
Contrast-enhanced 3-dimensional MR angiogram (gradient echo [GRE]:5/2) of a 9-year-old girl with hepatoblastoma. Venous-phase image demonstrates occlusion of the right portal vein and a filling defect in the proximal left portal vein suggestive of tumor thrombus. Tumor thrombus in this location was proven at surgery. Courtesy of Fredric Hoffer, MD, St. Jude Children's Research Hospital, Memphis, Tenn.
-
Contrast enhanced 3-dimensional MR angiogram (gradient echo [GRE]:5/2) of a 9-year-old girl with hepatoblastoma. The hepatoblastoma is located in the right lobe of the liver and is supplied by the right hepatic artery. MR angiogram demonstrates enlarged and tortuous common, proper, and right hepatic arteries. Courtesy of Fredric Hoffer, MD, St. Jude Children's Research Hospital, Memphis, Tenn.
-
Contrast-enhanced 3-dimensional MR angiogram (gradient echo [GRE]:6.2/2.2) of a 16-month-old boy with hepatoblastoma. Portal venous-phase image clearly demonstrates normal portal-venous anatomy.
-
Contrast-enhanced 3-dimensional MR angiogram (gradient echo [GRE]:5/2) of a 2-year-old girl with hepatoblastoma. Portal-venous-phase image demonstrates the dark tumor in the right lobe of the liver (open arrow) that compresses and obstructs the right portal vein (closed arrow). There is no thrombus within the portal vein.
-
Contrast-enhanced CT of a 7-year-old boy with hepatoblastoma. Large feeding vessels lead to the tumor. Large central area of necrosis is not unusual for hepatoblastoma, especially the anaplastic type.
-
Immediate (top) and delayed (bottom) contrast-enhanced CT of a 1-month-old boy with hepatoblastoma. The immediate image shows inhomogeneous contrast enhancement with focal unenhanced areas consistent with necrosis. Most hepatoblastomas enhance less than the surrounding normal liver, as seen in this patient. The delayed image shows washout of contrast material from the tumor.
-
Longitudinal ultrasound image of the right lobe of the liver demonstrates diffuse heterogeneity of the liver parenchyma in this 8-year-old boy with hepatoblastoma. Note the difficulty in determining the tumor's margins by ultrasound.
-
CT of the chest demonstrates diffuse bilateral pulmonary metastases in a 7-year-old boy with hepatoblastoma. The lungs are the most common site of metastatic disease in patients with hepatoblastoma and are involved in 10% of patients at diagnosis.
-
Anteroposterior view of the right shoulder demonstrates a metastatic deposit in the proximal humeral metadiaphysis in an 11-year-old girl with hepatoblastoma. Bone is the second most common site of metastatic disease from hepatoblastoma.


