Practice Essentials
Gastroesophageal reflux disease (GERD) is the excessive retrograde movement of acid-containing gastric secretions or bile and acid-containing secretions from the duodenum and stomach into the esophagus. A study by Richter and a Gallup Organization National Survey estimated that 25-40% of healthy adult Americans experience symptomatic GERD, most commonly manifested clinically by pyrosis (heartburn), at least once a month. Furthermore, approximately 7-10% of the adult population in the United States experiences such symptoms on a daily basis. GERD has an estimated worldwide prevalence of 8-33%, [1, 2, 3] There are 3 subtypes of GERD: nonerosive reflux disease, reflux esophagitis, and Barrett esophagus. [4, 5]
(See the images of GERD below.)
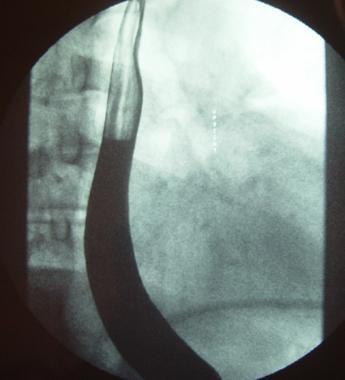 Barium esophagogram demonstrating gastroesophageal reflux with the patient in the upright position.
Barium esophagogram demonstrating gastroesophageal reflux with the patient in the upright position.
 Gastroesophageal reflux at the level of the thoracic inlet is demonstrated on this barium esophagogram.
Gastroesophageal reflux at the level of the thoracic inlet is demonstrated on this barium esophagogram.
In most people people with GERD, endogenous defense mechanisms either limit the amount of noxious material that is introduced into the esophagus or rapidly clear the material from the esophagus, so that symptoms and esophageal mucosal irritation are minimized. Examples of the defense mechanisms include actions of the lower esophageal sphincter (LES) and normal esophageal motility.
When the defense mechanisms are defective or become overwhelmed, so that the esophagus is bathed in acid or bile and acid-containing fluid for prolonged periods, GERD can be said to exist. Patients typically have numerous daily episodes of symptomatic reflux, including pyrosis, water brash or sour taste in the mouth, nighttime coughing or aspiration, pneumonia or pneumonitis, bronchospasm, and laryngitis and voice changes, including hoarseness. In addition, objective evidence of esophageal damage can be seen on esophagogastroduodenoscopy.
Typical GERD symptoms consist of heartburn and regurgitation, and a clinical diagnosis is made on the basis of these symptoms. Most patients with typical symptoms of GERD receive empirical treatment with a proton pump inhibitor (PPI) and do not undergo diagnostic testing. However, in patients with symptoms such as dysphagia, odynophagia, anorexia, weight loss, and upper gastrointestinal bleed, further investigation is generally undertaken. [6, 7]
Preferred examination
Mandatory studies include upper GI endoscopy and manometry. Barium esophagogram findings can demonstrate anatomy and possible complications of reflux disease (strictures). Reflux and inadequate gastric emptying may also be demonstrated. [8] High-resolution esophageal manometry (HRM) is an integral part of the diagnostic evaluation of patients with refractory reflux symptoms and should be performed before antireflux surgery. [7, 9, 3, 10, 11, 12]
If symptoms persist despite empirical therapy and if esophagogastroduodenoscopy (EGD) does not reveal evidence of GERD (esophagitis, peptic esophageal stricture, Barrett mucosa), esophageal function tests are performed, including esophageal manometry and ambulatory reflux monitoring. [9] A conclusive diagnosis of reflux disease cannot be made by using barium esophagography. This technique is not sensitive for the detection of motility disorders.
Studies have shown that narrow-band imaging endoscopy can reveal subtle changes of esophageal superficial mucosa in GERD patients. Narrow-band imaging is a technique in which the spectrum of white light is narrowed to specific blue and green wavelengths (410 nm and 540 nm, respectively) to better visualize changes in the mucosa. [13, 14]
Nuclear medicine gastric emptying studies are sensitive in evaluating for incomplete gastric emptying. [15] Nuclear medicine gastric-emptying study does not help in assessing anatomy and cannot help in the diagnosis of reflux disease.
Esophageal inflammation demonstrated by 18F-fluorodeoxyglucose (FDG) PET/CT has been shown to correlate with endoscopic findings and symptomatology of GERD. [16] .
Conclusive evidence for reflux on esophageal testing include (1) advanced grade erosive esophagitis and (2) long-segment Barrett mucosa or peptic strictures on EGD or distal esophageal acid exposure time (AET) greater than 6% on ambulatory pH or pH-impedance monitoring. A normal endoscopy does not exclude GERD but provides supportive evidence refuting GERD in conjunction with distal AET less than 4% and fewer than 40 reflux episodes on pH-impedance monitoring off proton pump inhibitors. [9]
Radiography
Plain radiographic findings are not useful in evaluating patients for GERD, but they are helpful in evaluating pulmonary status and basic anatomy. Chest images may demonstrate a large hiatal hernia, but small hernias can be missed easily.
(See the image of hiatal hernia below.)

In patients with pulmonary symptoms, an infiltrate due to aspiration pneumonia may be seen. The standard radiologic workup of a patient with reflux disease does not require chest radiography.
Upper GI series
Upper GI contrast-enhanced studies are the initial radiologic procedure of choice in the workup of the patient in whom GERD is suggested.
The primary use of upper GI contrast-enhanced studies in suspected reflux is to evaluate anatomy and not to detect reflux, as sensitivity is limited in patients with known esophagitis and normal controls can have visualized reflux. Drinking 15-30 mL of ice water can improve the sensitivity and specificity for reflux.
Barium esophagograms or swallows are helpful for identifying structural abnormalities of the esophagus and esophageal hiatus, which include esophageal rings, strictures and ulcers, and hiatal hernias.
(Barium esophagograms are presented below.)
Barium esophagogram demonstrating gastroesophageal reflux with the patient in the upright position.
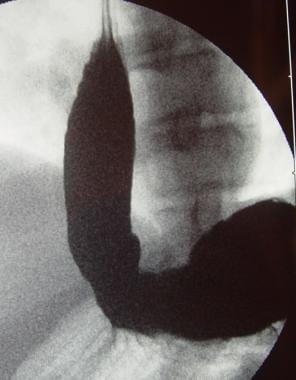 Barium esophagogram demonstrating gastroesophageal reflux with the patient in the supine position.
Barium esophagogram demonstrating gastroesophageal reflux with the patient in the supine position.
 Gastroesophageal reflux at the level of the thoracic inlet is demonstrated on this barium esophagogram.
Gastroesophageal reflux at the level of the thoracic inlet is demonstrated on this barium esophagogram.
Various techniques are used, and each has relative strengths and weaknesses in the ability to detect specific abnormalities or disease processes.
A typical barium esophagogram is performed in multiple steps or phases. A high-density barium suspension is administered, and double-contrast views are used for images taken with the patient in the upright position. Prone-positioned images are typically obtained with single contrast and a lower-density barium suspension. Mucosal relief images can be made to complement these techniques.
Esophageal inflammatory and neoplastic diseases are better detected with double-contrast techniques. Conversely, single-contrast techniques are more sensitive for structural defects such as hiatal hernias and strictures or esophageal rings. [17]
The presence of Barrett esophagus occasionally is detected as a reticular mucosal pattern. As may be expected, the more advanced the esophageal disease, the more sensitive is barium swallow at detecting it.
Early esophagitis is not well demonstrated and decreases the overall sensitivity of barium swallows, especially compared to tests such as 24-hour pH monitoring. This is why many clinicians reserve barium swallow for the evaluation of patients with GERD and symptoms that include dysphagia.
Barium swallow is not sensitive in the detection of actual reflux, except in the occasional patient who has a wide-open LES and free reflux. Barium swallow is a very important study in the investigation and detection of postoperative complications following fundoplication. Recurrent hiatal hernia, disruption or slippage of the fundoplication, and other structural abnormalities can be identified. [18, 19, 20]
Late postoperative dysphagia can be investigated by a combination of manometry and esophageal fluoroscopic examination. Increases in esophagogastric transit time of liquid barium and solid boluses correlate positively with the presence of postoperative dysphagia. [21]
Nuclear Imaging
Gastric-emptying studies may be worthwhile in the evaluation of patients in whom delayed gastric emptying is believed to contribute to the manifestation of GERD symptoms.
Gastroesophageal reflux scintigraphy can be performed with acidified orange juice labeled with technetium-99m (99mTc) sulfur colloid. Compared with fluoroscopy, this allows for a longer time of evaluation, a decreased radiation dose, and the ability to semiquantitate the amount of reflux. However, gastroesophageal reflux scintigraphy has little role in the adult patient because of limited sensitivity and the availability of other methods of evaluation.
Gastroesophageal reflux scintigraphy is much more commonly used in infants and children because of the noninvasive nature of the study and relatively low radiation dose. In infants and children, the study is often performed with labeled milk. In addition to evaluating the degree of reflux, pulmonary aspiration can be detected by imaging over the lungs.
Scintigraphic studies are neither sensitive nor specific for the diagnosis of GERD. The results should always be confirmed with another study, preferably upper GI endoscopy or 24-hour pH monitoring.
-
Barium esophagogram demonstrating gastroesophageal reflux with the patient in the upright position.
-
Barium esophagogram demonstrating gastroesophageal reflux with the patient in the supine position.
-
Hiatal hernia 1.
-
Reflux esophagitis is demonstrated on barium esophagogram.
-
Gastroesophageal reflux at the level of the thoracic inlet is demonstrated on this barium esophagogram.







