Practice Essentials
Fibrous dysplasia (FD) is a skeletal developmental anomaly of the bone-forming mesenchyme that manifests as a defect in osteoblastic differentiation and maturation. FD is a congenital disorder resulting from sporadic mutation of the α-subunit of the Gs stimulatory protein. Osseous changes are characterized by normal bone being replaced and distorted by poorly organized, structurally unsound, fibrous tissue. Virtually any bone, a single bone or multiple bones, may be affected, and virtually any bone in the body can be affected. [1, 2, 3, 4, 5, 6, 7]
Monostotic FD accounts for about 80% of cases. The most common locations of monostotic FD are the rib, the skull, and the femur. The most frequently affected sites of the polyostotic form are the skull, the mandible, the pelvic bones, and the femur. [8, 9, 10]
McCune-Albright syndrome features polyostotic fibrous dysplasia, often unilateral, with skin pigmentation lesions and endocrine dysfunction. Mazabraud syndrome is a polyostotic variant featuring coexistent single or multiple intramuscular myxomas. [11, 12, 13]
Plain radiography is the first-line study. Usually, the diagnosis is straightforward when typical features are present. The bone lesions can be classified as cystic, sclerotic, or mixed. A typical FD lesion in the axial skeleton appears as radiolucent ground-glass matrix that is usually smooth and homogeneous. Craniofacial FD typically displays dense and sclerotic lesions. The FD lesions usually cause cortical thinning because of enlarged fibro-osseous masses. [14, 15, 8]
Computed tomography (CT) scanning may be required to assess complex regions such as the spine, pelvis, chest, and facial skeleton. [16, 17, 18, 19, 15] CT imaging is better than radiography in delineating morphologic changes in bone. CT can define the anatomy of individual lesions and establish extent of disease. CT scans may identify soft-tissue masses and bone destruction and suggest malignant transformation. [15]
Typically, on magnetic resonance images (MRI), FD lesions show sharply demarcated borders and intermediate to low signal intensity on T1-weighted images and intermediate to high signal intensity on T2-weighted images. The higher the number of bony trabeculae, the lower the T2 signal. FD lesions may also contain small cystic areas, resulting in a brighter T2 signal. MRI is not particularly useful in differentiating FD from other lesions but can be helpful for complex cases, such as compression of neurologic structures. [20, 21, 14, 8, 22, 23]
Bone scintigraphy has a limited role in the detection of subtle pathologic fractures. In fibrous dysplasia, the features on a bone scan are nonspecific for diagnostic purposes. Technetium-99m-methyldiphosphonate (99mTc-MDP) may be used to detect metabolically active lesions and assess the extent of disease. On PET/CT, 18F-fluorodeoxyglucose (18F-FDG) and 18F-sodium fluoride (18F-NaF) uptake may mimic that of malignant lesions or metastases. Rapid, increased 18F-FDG uptake may suggest sarcomatous change. [8, 24]
(See the images below.)
 Image shows homogeneous loss of the normal trabecular pattern in the shaft of the humerus, with a ground-glass appearance caused by fibrous dysplasia.
Image shows homogeneous loss of the normal trabecular pattern in the shaft of the humerus, with a ground-glass appearance caused by fibrous dysplasia.
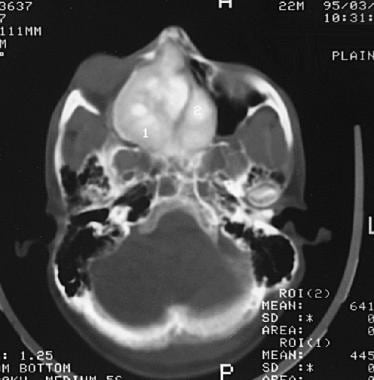
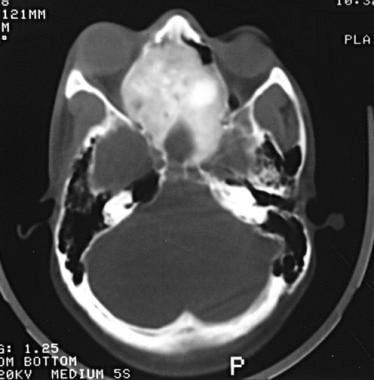 Axial bone-window CT scan shows a bony mass that expands the ethmoidal sinuses; this finding is consistent with fibrous dysplasia. Note the relative homogeneous attenuation of the lesion.
Axial bone-window CT scan shows a bony mass that expands the ethmoidal sinuses; this finding is consistent with fibrous dysplasia. Note the relative homogeneous attenuation of the lesion.
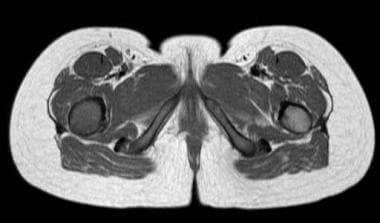 T1-weighted axial MR scan showing low signal within the shaft of right femur in a patient with fibrous dysplasia.
T1-weighted axial MR scan showing low signal within the shaft of right femur in a patient with fibrous dysplasia.
Radiography
Plain radiographs are highly specific when characteristic features are present in a lesion. However, the specificity decreases when the lesion occurs at more complex sites, such as the spine, the skull, and, sometimes, the pelvis. The identification of malignant change and soft-tissue extension on plain radiographs may be difficult; cross-sectional imaging may be required. Radiographic features suggestive of malignant degeneration include a rapid increase in the size of the lesion and a change from a previously mineralized bony lesion to a lytic lesion. [8, 11]
Long and short tubular bones
The usual appearance of fibrous dysplasia includes a lucent lesion in the diaphysis or metaphysis, with endosteal scalloping and with or without bone expansion and the absence of periosteal reaction. Usually, the matrix of the lucency is smooth and relatively homogeneous; classically, this finding is described as a ground-glass appearance. Irregular areas of sclerosis may be present with or without calcification. The lucent lesion has a thick sclerotic border and is called the rind sign.
(See the image below.)
Image shows homogeneous loss of the normal trabecular pattern in the shaft of the humerus, with a ground-glass appearance caused by fibrous dysplasia.
The lesion may extend into the epiphysis only after fusion. Premature fusion of the ossification centers may occur, resulting in adult dwarfism. The dysplastic bone may undergo calcification and enchondral bone formation.
Skull and facial bones
The frontal bone is involved more frequently than the sphenoid, with obliteration of the sphenoid and frontal sinuses. The skull base may be sclerotic. Single or multiple, symmetrical or asymmetrical, radiolucent or sclerotic lesions in the skull or facial bones may be present. The external occipital protuberance may be prominent; however, these features are less common in Paget disease, neurofibromatosis, and meningioma.
Most commonly, maxillary and mandibular involvement has a mixed radiolucent and radiopaque pattern, with displacement of the teeth and distortion of the nasal cavities. The diploic space is widened, with displacement of the outer table. The inner table of the skull is spared in fibrous dysplasia, unlike in Paget disease. Cystic calvarial lucencies, which commonly cross the sutures with sclerotic margins, may have a doughnut configuration.
Pelvis and ribs
The pelvis and ribs have lucencies, with a diffuse ground-glass appearance and rind lesions. Cystic lesions are common. Protrusio acetabuli is a feature on the pelvic radiograph.
(See the image below.)
 Chest radiograph shows expansion of multiple ribs involved by fibrous dysplasia that mimics pleural masses.
Chest radiograph shows expansion of multiple ribs involved by fibrous dysplasia that mimics pleural masses.
Spine
Spinal involvement is common in polyostotic disease and rare in monostotic disease. Well-defined, expansile, radiolucent lesions with multiple internal septa or striations involve the vertebral body and, occasionally, the pedicles and arches. Paraspinal soft-tissue extension and vertebral collapse are rare. Kyphotic deformity and spinal cord compression may occur.
Computed Tomography
CT scanning is not often required for diagnosis. CT scanning is not optimal for the differentiation of fibrous dysplasia from other lesions that mimic it. CT findings complement plain radiographic findings.The modality demonstrates the nature of the lesion better by characterizing the matrix of the lesion. It also depicts expansion of the affected bone and its subtle mineral contents. It can demonstrate subtle nondisplaced pathologic fractures. CT is extremely useful in evaluating the extent of disease in complex locations, such as the facial bones, pelvis, chest wall, and spine. Usually, attenuation is in the range of 70-130 HU (Hounsfield unit). [16, 17, 18, 19, 8, 11]
In the skull, the outer table always expands outward. Therefore, the lesion is invariably convex; both tables are intact, although they are thinner. In the spine, CT can demonstrate the extent of bony disease and compromise of the spinal canal space. Paraspinal soft-tissue extension can be demonstrated at CT. CT scans may suggest malignant transformation, with the definition of an extraosseous soft-tissue mass and bone destruction.
(See the images below.)
Axial bone-window CT scan shows a bony mass that expands the ethmoidal sinuses; this finding is consistent with fibrous dysplasia. Note the relative homogeneous attenuation of the lesion.
 Coronal image shows craniofacial fibrous dysplasia extending posteriorly into the sphenoidal sinus.
Coronal image shows craniofacial fibrous dysplasia extending posteriorly into the sphenoidal sinus.
 Coronal CT scan shows craniofacial fibrous dysplasia with expansion of paranasal sinuses caused by a homogeneous mass. The inferior part of the vestibule of the nasal cavity has a soft-tissue component.
Coronal CT scan shows craniofacial fibrous dysplasia with expansion of paranasal sinuses caused by a homogeneous mass. The inferior part of the vestibule of the nasal cavity has a soft-tissue component.
Magnetic Resonance Imaging
On T1-weighted MRIs, the lesion has low-to-intermediate signal intensity equal to that of muscle. T2-weighted images also show low signal intensity because of the high content of collagen and bone. Cartilaginous islands may be present in some lesions, and they appear as areas of high signal intensity on T2-weighted images. In children, T2-weighted images show hyperintense signal greater than that of subcutaneous fat; this finding is characteristic of fibrous dysplasia. [18, 8, 11, 22, 23]
(See the images below.)
 An area of low signal on T1-weighted MR scan, within the proximal shaft of the right femur. Note the narrow zone of transition from lesion to normal marrow.
T1-weighted axial MR scan showing low signal within the shaft of right femur in a patient with fibrous dysplasia.
An area of low signal on T1-weighted MR scan, within the proximal shaft of the right femur. Note the narrow zone of transition from lesion to normal marrow.
T1-weighted axial MR scan showing low signal within the shaft of right femur in a patient with fibrous dysplasia.
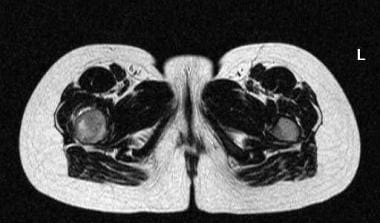 T2-weighted axial image showing a heterogeneous high signal within a fibrous dysplasia in the proximal shaft of the right femur.
T2-weighted axial image showing a heterogeneous high signal within a fibrous dysplasia in the proximal shaft of the right femur.
 Sagittal T2-weighted image of fibrous dysplasia lesion in the shaft of the femur. Note there is some degree of expansion of the bone.
Sagittal T2-weighted image of fibrous dysplasia lesion in the shaft of the femur. Note there is some degree of expansion of the bone.
Also, fluid-fluid levels are reported in fibrous dysplasia. On short–inversion time inversion-recovery (STIR) images, the signal intensity of the lesion may be very high. MRI may be useful in assessing malignant change and demonstrating extension of the tumor into the surrounding soft tissues.
Milk cloud appearance is a characteristic sign of fibrous dysplasia on contrast-enhanced T1-weighted MR images. [22]
For postoperative follow-up, gadolinium-enhanced MRI is useful in demonstrating the proliferation of fibrocellular tissue.
Gadolinium-based contrast agents have been linked to the development of nephrogenic systemic fibrosis (NSF) or nephrogenic fibrosing dermopathy (NFD). The disease has occurred in patients with moderate to end-stage renal disease after being given a gadolinium-based contrast agent to enhance MRI or MRA scans. NSF/NFD is a debilitating and sometimes fatal disease. Characteristics include red or dark patches on the skin; burning, itching, swelling, hardening, and tightening of the skin; yellow spots on the whites of the eyes; joint stiffness with trouble moving or straightening the arms, hands, legs, or feet; pain deep in the hip bones or ribs; and muscle weakness.
Nuclear Imaging
Bone scintigraphy has a limited role in the detection of subtle pathologic fractures. In fibrous dysplasia, the features on a bone scan are nonspecific for diagnostic purposes. Accumulation of isotope increases because of the lesion's hypervascularity. Hot spots or increased uptake of the radioisotope tracer technetium-99m methylene diphosphonate (99mTc MDP) occurs in the spine, pelvis, ribs, and appendicular skeleton. Pathologic or stress fractures also can increase isotopic activity in the lesions. Tc-99m-MDP may be used to detect metabolically active lesions and assess the extent of disease. On PET/CT, 18F-fluorodeoxyglucose (18F-FDG) and 18F-sodium fluoride (18F-NaF) uptake may mimic that of malignant lesions or metastases. Rapid, increased 18F-FDG uptake may suggest sarcomatous change. [20, 21, 8, 24]
-
Image shows homogeneous loss of the normal trabecular pattern in the shaft of the humerus, with a ground-glass appearance caused by fibrous dysplasia.
-
Chest radiograph shows expansion of multiple ribs involved by fibrous dysplasia that mimics pleural masses.
-
Axial bone-window CT scan shows a bony mass that expands the ethmoidal sinuses; this finding is consistent with fibrous dysplasia. Note the relative homogeneous attenuation of the lesion.
-
Image shows focal areas of calcification in craniofacial fibrous dysplasia.
-
Coronal image shows craniofacial fibrous dysplasia extending posteriorly into the sphenoidal sinus.
-
Coronal CT scan shows craniofacial fibrous dysplasia with expansion of paranasal sinuses caused by a homogeneous mass. The inferior part of the vestibule of the nasal cavity has a soft-tissue component.
-
An area of low signal on T1-weighted MR scan, within the proximal shaft of the right femur. Note the narrow zone of transition from lesion to normal marrow.
-
T1-weighted axial MR scan showing low signal within the shaft of right femur in a patient with fibrous dysplasia.
-
T2-weighted axial image showing a heterogeneous high signal within a fibrous dysplasia in the proximal shaft of the right femur.
-
Sagittal T2-weighted image of fibrous dysplasia lesion in the shaft of the femur. Note there is some degree of expansion of the bone.








