Practice Essentials
Fibromuscular dysplasia (FMD) is a noninflammatory, nonatherosclerotic arterial disease of the medium-sized arteries throughout the body, which could lead to arterial stenosis, occlusion, aneurysm, and dissection. [1] Tortuosity or redundancy of the arteries, particularly the internal carotid arteries, has been reported in association with FMD. [2]
FMD predominantly affects women 20 to 60 years of age, although men and children can also be affected. In the US Registry for FMD, 93.5% of patients are women. [3] Patients 65 years or older at the time of diagnosis of FMD appear to have a more benign phenotype and fewer symptoms. [4]
The disease typically affects the renal and extracranial carotid arteries, but it has also been noted in most medium-sized arteries throughout the body, most commonly the mesenteric, external iliac, and brachial arteries. [2] Disease manifestations depend on the arterial bed involved: most often, the extracranial carotid or vertebral arteries are associated with headache (generally migraine-type), pulsatile tinnitus, neck pain, or dizziness, whereas the renal arteries are often associated with hypertension. More severe symptoms such as transient ischemic attack (TIA), stroke, ruptured aneurysm, or a carotid or vertebral artery dissection can develop in patients with cerebrovascular FMD. [1, 3] The diagnosis of FMD is made by imaging studies; there is no blood test for FMD. and biopsies are not performed.
Although the pathophysiology of FMD)is not known, smoking has been implicated as a potential contributing factor and portends a worse prognosis. A study from the US FMD Registry found that smokers with FMD had significantly higher rates of claudication and need for therapeutic intervention. Smokers with FMD were more likely to experience major vascular events such as stroke or heart attack, as compared to patients who had never smoked. Smoking also appears to increase the risk for aneurysms in patients with FMD, a population in which the risk for aneurysmal disease is already significant. [5] The American Heart Association (AHA) recommends that all patients with FMD in any location be screened for intracranial aneurysms by CT angiography (CTA) or MR angiography (MRA). [6]
There are 2 types of FMD: multifocal and focal. Multifocal FMD is by far the more common type, affecting 90% or more of FMD patients. The hallmark of multifocal FMD is the "string of beads" appearance of the artery (see the image below). This finding is present when areas of artery narrowing due to fibrous tissue and webs alternate with areas of artery enlargement or dilation. Less common imaging findings include vascular loops, fusiform vascular ectasia, arterial dissection, aneurysm, and subarachnoid hemorrhage. [7] Focal FMD usually consists of a single, smoother narrowing in an artery. The focal type is more common in children and teenagers. [3]
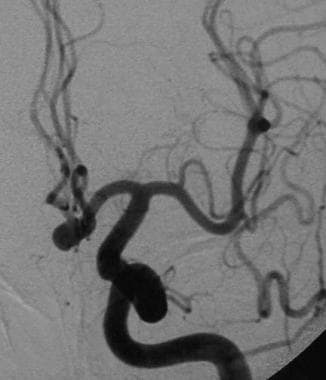
 Angiogram of type 1 fibromuscular dysplasia in a 43-year-old female patient with multiple transient ischemic attacks. Note the multiple saccular dilatations of the internal carotid artery between the first and second cervical vertebrae.
Angiogram of type 1 fibromuscular dysplasia in a 43-year-old female patient with multiple transient ischemic attacks. Note the multiple saccular dilatations of the internal carotid artery between the first and second cervical vertebrae.
Preferred Examination
Catheter-based (invasive) angiography remains the gold standard test for diagnosing FMD. However, this method is not used to diagnose FMD in routine clinical practice, given its invasive nature, expense, and use of both radiation and iodine-based contrast dye. Instead, angiography is used to diagnose FMD only if other imaging studies have been unclear or if a procedure is needed (such as angioplasty). [6] Although the technical standard of diagnostic imaging is catheter angiography, Doppler ultrasonography, CTA, and MRA are more commonly used to diagnose and monitor the disease. [2] Features of FMD that can be identified with Doppler ultrasound include beading, turbulent blood flow and abnormally high speed (velocity) blood flow, and tortuosity or S-shaped arteries. In some cases, although beading can be seen with duplex ultrasound, it is better appreciated by other types of imaging studies, such as catheter angiography, CTA, or MRA. Both CTA and MRA can be used to create detailed reconstructions of the anatomy of the arteries and are accurate in visualizing aneurysms, dissections, and areas of beading. [3]
Deciding which type of imaging to use for diagnosis or follow-up of FMD depends on the vessels that need to be imaged, patient factors (such as allergy to contrast dye or kidney problems), and local availability and expertise. Once FMD is diagnosed, the AHA recommends that patients undergo comprehensive one-time imaging of the arteries from head to pelvis to determine which areas are affected and to check for any aneurysms or dissections of arteries. Subsequent follow-up may be limited to imaging of the areas of the body that are involved with FMD and, in some cases, may be as simple as periodic duplex ultrasound studies. The frequency of repeating surveillance imaging studies is customized for each patient. [1, 6]
Because of the low-risk (ie, no iodinated contrast and no radiation) and low-cost nature of Doppler ultrasound, it is a preferred modality for surveillance of carotid artery FMD. Although there are no evidence-based algorithms for surveillance of carotid artery involvement, the AHA suggests a program of duplex ultrasound surveillance every 6 or 12 months initially and then annually. [6]
Computed Tomography
Although conventional computed tomography (CT) scanning has no role in the diagnosis of fibromuscular dysplasia, it is essential for assessing the intracranial consequences of the disease. CT angiography (CTA) may be used as a noninvasive means of diagnosing the vascular changes of FMD. CTA may display the pathognomonic string of beads appearance of the internal carotid artery. It is recommended that CTA findings be confirmed with carotid angiography.
Current resolution (voxel sizes) of CT may limit the usefulness of this modality in the diagnosis of subtle cases. As this technique improves, its negative predictive value may increase, so as to make it useful in excluding FMD from the differential diagnosis.
Signal/noise artifacts or reconstruction artifacts that occur with CTA occasionally may mimic the contour irregularity of FMD.
Magnetic Resonance Imaging
Magnetic resonance angiography (MRA) may display the pathognomonic string of beads appearance of the internal carotid artery. MRA may have the benefit of detecting FMD-associated dissections when T1 fat-saturated images are acquired simultaneously with time-of-flight or gadolinium-enhanced images. Advantages of MR-based technology are the lack of radiation and the lack of iodinated contrast agents, which may make it a reasonable screening tool in younger patients. [6]
Like CTA, MRA may be used as a noninvasive means of diagnosing the vascular changes associated with FMD. Although MRA does not require the use of contrast, intravenous administration of a gadolinium contrast agent often yields superior imaging results. Confirmation of the findings through the use of carotid angiography is recommended before endovascular or surgical interventions are considered.
Gadolinium-based contrast agents have been linked to the development of nephrogenic systemic fibrosis (NSF) or nephrogenic fibrosing dermopathy (NFD). For more information, see Nephrogenic Systemic Fibrosis. NSF/NFD has occurred in patients with moderate to end-stage renal disease after being given a gadolinium-based contrast agent to enhance MRI or MRA scans. NSF/NFD is a debilitating and sometimes fatal disease. Characteristics include red or dark patches on the skin; burning, itching, swelling, hardening, and tightening of the skin; yellow spots on the whites of the eyes; joint stiffness with trouble moving or straightening the arms, hands, legs, or feet; pain deep in the hip bones or ribs; and muscle weakness. For more information, see Medscape.
Current resolution (voxel sizes) of MRA may limit the usefulness of this modality in the diagnosis of subtle cases. MRI is sensitive to motion and metallic artifacts. MRI images may appear artifactually beaded as a result of the patient's swallowing during the examination. The presence of a ferrous metal object may cause the contour of the vessels to be distorted. Signal/noise artifacts or reconstruction artifacts that occur with CTA or MRA occasionally may mimic the contour irregularity of FMD.
Ultrasonography
Doppler ultrasound findings consistent with carotid FMD include the identification of velocity shifts in the mid to distal cervical internal carotid artery and the vertebral arteries with associated turbulence of color flow or the spectral Doppler signal. These findings are in contrast to atherosclerotic disease, in which significant plaque is generally visualized at or just beyond the carotid bifurcation associated with velocity shift and turbulent flow in the origin or proximal segment of the internal carotid artery at or immediately beyond the plaque. Because of the more distal location of FMD findings on the ultrasound examination, interrogation of the entire internal carotid artery, not just the segments at or immediately distal to the carotid bulb, is essential. Some patients, particularly elderly patients, may present with findings of both atherosclerosis and FMD on carotid ultrasound. In addition to velocity shifts and turbulent flow, beading of the vessel (string of beads) in the mid or distal cervical internal carotid artery may be identified, although this is a less common finding. [6]
Given that the pathology of FMD involves the distal cervical segment of the extracranial internal carotid and vertebral arteries, carotid ultrasonography may provide suboptimal views and potentially may not be able to visualize the areas of involvement.
Because of the nature of FMD, which manifests with areas of narrowing and dilatation in tandem (string of beads), standard criteria for stenosis resulting from atherosclerosis at the vessel origin do not apply. In less experienced vascular laboratories, the finding of FMD may be misinterpreted as representing an atherosclerotic lesion and a percentage stenosis erroneously ascribed. [6]
Angiography
Angiography is the criterion standard for diagnosing fibromuscular dysplasia. [8] The string of beads appearance is considered pathognomonic for medial fibroplasia on diagnostic angiography. The classic string of beads contour is characterized by a long-segment tubular stenosis or ovoid-shaped outpouchings.
When the carotid arteries are involved, the cervical segment C1-C2 is most often affected. Intracranial disease is rare; when it does occur, the beaded appearance may extend to the supraclinoid segment of the internal carotid artery or to the middle cerebral artery. A diagnosis of intracranial FMD should not be considered in the absence of cervical carotid disease.
(See the images below.)
Angiogram of type 1 fibromuscular dysplasia in a 43-year-old female patient with multiple transient ischemic attacks. Note the multiple saccular dilatations of the internal carotid artery between the first and second cervical vertebrae.
 Subtracted digital angiogram demonstrating multiple saccular dilations and stenosing webs. Increased turbulence and foci of stasis predispose the patient to thrombus formation.
Subtracted digital angiogram demonstrating multiple saccular dilations and stenosing webs. Increased turbulence and foci of stasis predispose the patient to thrombus formation.
 Anterior communicating artery aneurysm. An increased association of aneurysm formation is seen in patients with fibromuscular dysplasia.
Anterior communicating artery aneurysm. An increased association of aneurysm formation is seen in patients with fibromuscular dysplasia.
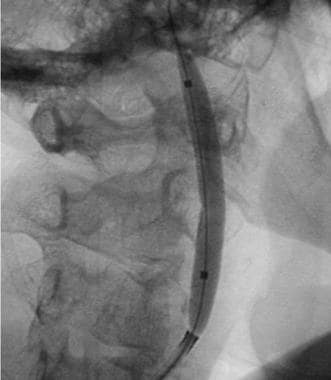 Balloon angioplasty offers a minimally invasive means to improve the arterial flow dynamics in fibromuscular dysplasia.
Balloon angioplasty offers a minimally invasive means to improve the arterial flow dynamics in fibromuscular dysplasia.
 Postangioplasty angiogram demonstrating improved luminal diameter of the internal carotid artery. Stenting may provide a more normal luminal contour, further decreasing thrombogenicity.
Postangioplasty angiogram demonstrating improved luminal diameter of the internal carotid artery. Stenting may provide a more normal luminal contour, further decreasing thrombogenicity.
Patients with carotid FMD may also have renal artery FMD and, less commonly, FMD of the lumbar, mesenteric, celiac, hepatic, and iliac arteries. Therefore, peripheral angiography should be considered for those patients manifesting symptoms of arterial stenosis or thromboembolic disease. Conversely, if fibromuscular dysplasia is encountered anywhere in the peripheral circulation, the carotid arteries should be evaluated.
A carotid web is a shelflike linear filling defect in the posterior aspect of the internal carotid artery bulb and thought to represent an intimal variant of FMD. This entity has been increasingly recognized as a cause of recurrent stroke. The diagnosis of carotid webs has historically relied on conventional angiography. In a series of 24 patients with carotid web who underwent catheter-based angiography, contrast stagnation rostral to the bulb, with pooling of contrast persisting into the angiogram’s venous phase, was a consistent finding. The relatively common finding of superimposed thrombus along the rostral surface of the web supported the etiologic plausibility of webs causing blood flow stagnation, predisposing to thromboembolism. [9]
-
Diagram representing the 3 major characteristic angiographic patterns seen in fibromuscular dysplasia of the internal carotid artery. Courtesy of Neuroradiology Test and Syllabus, Part 2.
-
Angiogram of type 1 fibromuscular dysplasia in a 43-year-old female patient with multiple transient ischemic attacks. Note the multiple saccular dilatations of the internal carotid artery between the first and second cervical vertebrae.
-
Subtracted digital angiogram demonstrating multiple saccular dilations and stenosing webs. Increased turbulence and foci of stasis predispose the patient to thrombus formation.
-
Anterior communicating artery aneurysm. An increased association of aneurysm formation is seen in patients with fibromuscular dysplasia.
-
Balloon angioplasty offers a minimally invasive means to improve the arterial flow dynamics in fibromuscular dysplasia.
-
Postangioplasty angiogram demonstrating improved luminal diameter of the internal carotid artery. Stenting may provide a more normal luminal contour, further decreasing thrombogenicity.




