Practice Essentials
Angiomyolipoma (AML) is a benign renal neoplasm composed of fat, vascular, and smooth muscle. Two types are described: isolated angiomyolipoma and angiomyolipoma that is associated with tuberous sclerosis (see the images below). AML that is associated with tuberous sclerosis accounts for 20% of angiomyolipomas. The lesions are typically larger than isolated angiomyolipomas, and they are often bilateral and multiple. Angiomyolipomas occur in 80% of patients with tuberous sclerosis. [1, 2, 3, 4, 5, 6, 7]
Renal AML can be classified according to amount of fat as fat rich, fat poor, or fat invisible. [3, 4, 5] Angiomyolipoma that is fat invisible should undergo biopsy. If it is difficult to differentiate fat-poor AML from renal cell carcinoma with CT or MRI, percutaneous biopsy may be necessary. Contrast is occasionally needed for better definition of angiomyolipomas and the differential diagnosis between fat-poor angiomyolipomas and other renal tumors. [2, 3, 4, 8, 6]
The male-to-female sex distributions of angiomyolipoma in patients with tuberous sclerosis are nearly equal, but the prevalence is higher in women. Angiomyolipomas occur in young women with lymphangiomyomatosis without other stigmata of tuberous sclerosis. Angiomyolipomas and lymphangiomyomatosis are sometimes considered the forme fruste of tuberous sclerosis. Although angiomyolipomas are considered benign, rare cases that are possibly related to multicentric disease have been reported regarding extension into the renal vein, the inferior vena cava (IVC), or both; deposits in the regional lymph nodes have also been reported. [9, 10]
Most small AML lesions are asymptomatic and are found incidentally on imaging studies. As many as 40% are symptomatic; these may manifest themselves as a palpable abdominal mass, and they may cause hematuria or flank pain. Solitary sporadic tumors may cause an acute abdomen and shock as a result of spontaneous hemorrhage in the tumor. The demonstration of fatty attenuation in renal tumor on CT scanning studies is virtually diagnostic of angiomyolipomas. [1, 9, 10, 2, 3, 4]
Preferred examination
CT scanning: CT scanning is highly accurate in the characterization and diagnosis of angiomyolipoma lesions. When negative attenuation values of less than 20 HU are recorded in renal tumors, angiomyolipomas may be reliably diagnosed in the appropriate clinical setting, and the diagnosis of a renal cell carcinoma can generally be ruled out. AML without visible fat are typically homogeneously hyperdense on unenhanced CT without calcification or hemorrhage. Unenhanced CT pixel analysis is not useful for diagnosis. AML without visible fat commonly shows avid early enhancement with washout kinetics on contrast-enhanced CT and MRI. [2, 3, 4, 11, 8, 12, 13, 14]
MRI: The characteristic appearances of angiomyolipomas with MRI include variable areas of high signal intensity within the tumor on both T1-weighted and T2-weighted images. On a nonenhanced T1-weighted image, high signal intensity is present because of the fat content. On T2-weighted images, the signal remains isointense relative to that of perinephric fat. [2, 15, 16, 17, 18, 19]
Ultrasonography: The most characteristic ultrasonographic feature of an angiomyolipoma is its echogenicity; however, angiomyolipomas may also cause acoustic shadowing. [20] The echogenic appearance of the tumor is thought to be related to its fat content and the presence of multiple tissue interfaces within it. Fat-rich angiomyolipomas are almost always hyperechoic on gray-scale ultrasound, and the lesion echogenicity is the same as or greater than that of renal sinus. As the amount of fat decreases, the lesion echogenicity also decreases. [2, 7]
Plain abdominal radiography: Angiomyolipomas of sufficient size may be appreciated on a plain abdominal radiograph or an IV urogram (see the images below). A large, extrarenal, exophytic component is present in 25% of cases; it may be visualized with both a plain abdominal radiograph and an IV urogram.
Nuclear imaging: The role of nuclear imaging is restricted to isotope renography with technetium-99m (99mTc) mercaptoacetythiglycine (MAG3) to assess relative renal function before nephron-sparing surgery. Tc-99m DMSA scanning may be used to assess differential renal function. It may be more useful in differentiating true masses and pseudomasses in cases in which other imaging findings are equivocal.
 Renal ultrasonogram obtained in a 12-year-old boy with known tuberous sclerosis. Note the multiple echogenic tumors of varying sizes in both kidneys. This oblique sagittal scan through the left kidney shows a 4-cm echogenic mass (arrow) on the inferior aspect of the kidney that anteriorly displaces the renal sinus (S).
Renal ultrasonogram obtained in a 12-year-old boy with known tuberous sclerosis. Note the multiple echogenic tumors of varying sizes in both kidneys. This oblique sagittal scan through the left kidney shows a 4-cm echogenic mass (arrow) on the inferior aspect of the kidney that anteriorly displaces the renal sinus (S).
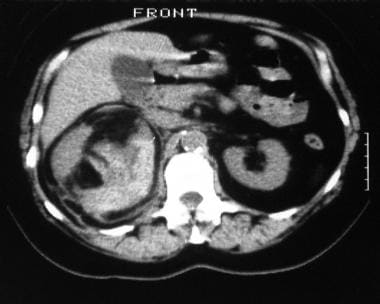
 Computed tomography scan obtained in a 15-year-old boy with tuberous sclerosis (under surveillance). The image shows rapid growth in a right renal lesion with mixed attenuation. The final diagnosis was tuberous sclerosis–associated angiomyolipoma.
Computed tomography scan obtained in a 15-year-old boy with tuberous sclerosis (under surveillance). The image shows rapid growth in a right renal lesion with mixed attenuation. The final diagnosis was tuberous sclerosis–associated angiomyolipoma.
Isolated AML occurs sporadically (see the image below). It is often solitary and accounts for 80% of the angiomyolipomas. [1] The mean age at presentation of patients with isolated angiomyolipoma is 43 years; this neoplasm is about 4 times more common in women than in men. [21] Interestingly, 80% of the cases involve the right kidney. [1]
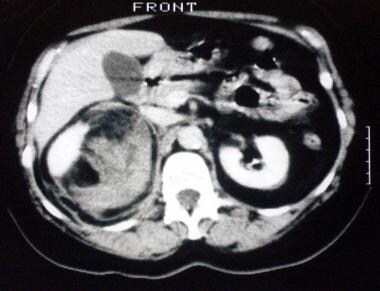
 Nonenhanced axial computed tomography scan through the kidneys. The image shows a space-occupying lesion of mixed attenuation interspersed with areas of fat attenuation. The final diagnosis was sporadic angiomyolipoma.
Nonenhanced axial computed tomography scan through the kidneys. The image shows a space-occupying lesion of mixed attenuation interspersed with areas of fat attenuation. The final diagnosis was sporadic angiomyolipoma.
Although routine follow-up seems reasonable for all patients with tuberous sclerosis, more intensive follow-up is necessary to establish the need for diagnostic resection for patients with tuberous sclerosis who have small masses (< 3 cm in diameter) that are radiologically atypical of angiomyolipomas. Apart from this group with tuberous sclerosis, follow-up may be reasonably restricted to patients with sporadic tumors greater than 4 cm in diameter, in whom the incidence of hemorrhagic complications is higher.
With developments in abdominal ultrasonography, CT scanning, and MRI, the incidental detection of asymptomatic angiomyolipomas has increased. Imaging experience shows that the presence of renal angiomyolipomas is more common than previously reported. With advances in cross-sectional imaging, the diagnosis of renal angiomyolipoma can usually be established without surgery; most of these tumors can be managed conservatively, particularly if they are asymptomatic.
Classification
Song et al described a radiologic classification of angiomyolipomas based on CT and MRI findings, classifying renal angiomyolipomas into fat-rich, fat-poor, and fat-invisible by using CT and MRI measurements, as follows [2, 4, 5, 22, 23] :
-
Fat-rich is a lesion with CT attenuation of –10 HU or less.
-
Fat-poor is a lesion with CT attenuation of more than –10 HU but with an MRI tumor-to-spleen ratio < 0.71 or a signal intensity index >16.5%.
-
Fat-invisible is defined as a lesion with CT attenuation greater than –10 HU and a tumor- to-spleen ratio of 0.71 or greater and a signal intensity index of 16.5% or less.
Radiography
Angiomyolipomas of sufficient size may be appreciated on a plain abdominal radiograph or an IV urogram (see the images below). A large, extrarenal, exophytic component is present in 25% of cases; it may be visualized with both a plain abdominal radiograph and an IV urogram.
Renal ultrasonogram obtained in a 12-year-old boy with known tuberous sclerosis. Note the multiple echogenic tumors of varying sizes in both kidneys. This oblique sagittal scan through the left kidney shows a 4-cm echogenic mass (arrow) on the inferior aspect of the kidney that anteriorly displaces the renal sinus (S).
 Renal ultrasonogram depicting many tumors in the right kidney. The arrow marks an echogenic 1-cm lesion (same patient as in the previous image).
Renal ultrasonogram depicting many tumors in the right kidney. The arrow marks an echogenic 1-cm lesion (same patient as in the previous image).
 Selective right renal angiogram showing multiple avascular tumors. The tumors are small (same patient as in the previous image).
Selective right renal angiogram showing multiple avascular tumors. The tumors are small (same patient as in the previous image).
 Selective left renal angiogram showing 2 tumors, which are larger than those in the previous image (same patient as in the previous image). The final diagnosis was multiple renal angiomyolipomas in a patient with tuberous sclerosis.
Selective left renal angiogram showing 2 tumors, which are larger than those in the previous image (same patient as in the previous image). The final diagnosis was multiple renal angiomyolipomas in a patient with tuberous sclerosis.
 Ultrasonogram obtained in a 48-year-old man who presented with dyspepsia and right upper quadrant discomfort. The patient was referred for a gallbladder ultrasonogram. The gallbladder was normal, but a solid 18-mm mass was present in the upper pole of the right kidney; it was isoechoic relative to the renal sinus.
Ultrasonogram obtained in a 48-year-old man who presented with dyspepsia and right upper quadrant discomfort. The patient was referred for a gallbladder ultrasonogram. The gallbladder was normal, but a solid 18-mm mass was present in the upper pole of the right kidney; it was isoechoic relative to the renal sinus.
 Part of an intravenous urogram series obtained in the same patient as in the previous image. The radiograph shows a hypoattenuating exophytic mass (arrow).
Part of an intravenous urogram series obtained in the same patient as in the previous image. The radiograph shows a hypoattenuating exophytic mass (arrow).
If planar tomographic images are obtained before the administration of IV contrast material and if a large quantity of fat is present within the tumor, radiolucency may be evident. This finding suggests the diagnosis of angiomyolipoma; it is seen in more than 10% of cases. With multiple large angiomyolipomas, particularly those in patients with tuberous sclerosis, an IV urogram may demonstrate distortion of the renal collecting system that is indistinguishable from polycystic renal disease. On CT scans, calcification is apparent within the tumor in as many as 6% of cases.
Plain radiography and IV urography are not useful in the diagnosis of angiomyolipoma, because neither modality has enough sensitivity to demonstrate fat within the tumor. Moreover, there are other causes of the occurrence of fat within renal masses, although such cases are rare. Multiple angiomyolipomas that distort the collecting system may be indistinguishable from polycystic disease. A false-positive diagnosis may occur in cases involving other renal tumors containing fatty tissue. Only larger angiomyolipomas contain a sufficient amount of fat to be visible on plain radiographs.
Computed Tomography
Unenhanced CT clearly depicts a hypoattenuating area (≤–10 HU) suggesting fat in fat-rich angiomyolipomas. Unenhanced CT cannot show a hypoattenuating area measuring less than –10 HU in a fat-poor angiomyolipoma because the amount of fat is very small. Contrast-enhanced CT is not necessary for diagnosing fat-rich angiomyolipoma, but it should be performed when there is potential for tumor bleeding. Large fat-rich angiomyolipomas often contain many tortuous or dilated vessels, which are susceptible to bleeding. The characterization of angiomyolipomas with CT is dependent on spatial resolution and accurate determination of attenuation values; newer spiral scanners meet these criteria. As a result, CT scanning is highly accurate in the characterization and diagnosis of angiomyolipoma lesions. [22, 23]
When negative attenuation values of less than 20 HU are recorded in renal tumors, angiomyolipomas may be reliably diagnosed in the appropriate clinical setting, and the diagnosis of a renal cell carcinoma can generally be ruled out. However, isolated reports of renal cell carcinoma with demonstrable fat content have appeared in the literature. These renal carcinomas may entrap surrounding perinephric fat or undergo fatty change because of metaplasia. Intratumoral fat is also reported in Wilms tumors, oncocytoma, xanthogranulomatous pyelonephritis, renal and retroperitoneal liposarcoma, and teratoma. A false-negative diagnosis is made in the 5% of patients with angiomyolipomas that contain only microscopically visible fat. [24, 11, 8, 12, 13, 25, 26]
Angiomyolipomas are usually well-marginated, cortical heterogeneous tumors with predominantly fatty attenuation; rarely, higher attenuation is seen in patients who have tumors with minimal fat content. The average attenuation depends on the relative proportions of fat and other soft tissue in the angiomyolipoma. In small masses, fat may be averaged out with region-of-interest (ROI) circles, and pixel maps may be useful. Attenuations of less than –20 HU are widely accepted as confirming the presence of fat; this finding virtually confirms the diagnosis of angiomyolipoma. Nonfatty angiomyolipomas are rare, but renal cell carcinoma may engulf fat. Angiomyolipomas may calcify and cause the HU value to increase out of the range for fat. However, this effect is rare; significant calcification should prompt the reconsideration of angiomyolipoma as a diagnosis. [24, 11, 8, 12, 13, 25, 26]
The widespread availability of spiral and multisection CT scanning has made the characterization of angiomyolipoma tumors more accurate (see the images below). [27] Nonenhanced spiral CT scanning with 5-mm collimation and a pitch of 1.5 that is followed by nephrographic contrast-enhanced phase imaging (120-180 s after injection) is ideal for characterization. It is important to review the nonenhanced images for fat because contrast enhancement averages out the appearance of fat. In small tumors, thin reconstructions may be necessary to optimize fat sensitivity.
Computed tomography scan obtained in a 15-year-old boy with tuberous sclerosis (under surveillance). The image shows rapid growth in a right renal lesion with mixed attenuation. The final diagnosis was tuberous sclerosis–associated angiomyolipoma.
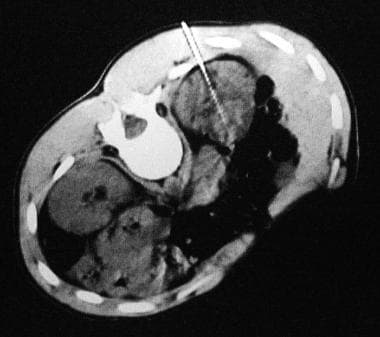 Computed tomography (CT) scan obtained in the same patient as in the previous image. The image shows the technique of CT scanning-guided biopsy with a Tru-cut needle.
Nonenhanced axial computed tomography scan through the kidneys. The image shows a space-occupying lesion of mixed attenuation interspersed with areas of fat attenuation. The final diagnosis was sporadic angiomyolipoma.
Computed tomography (CT) scan obtained in the same patient as in the previous image. The image shows the technique of CT scanning-guided biopsy with a Tru-cut needle.
Nonenhanced axial computed tomography scan through the kidneys. The image shows a space-occupying lesion of mixed attenuation interspersed with areas of fat attenuation. The final diagnosis was sporadic angiomyolipoma.
 Contrast-enhanced axial computed tomography scan obtained through the kidneys in the same patient as in the previous image. The image shows patchy tumor enhancement, with displacement of part of the normal lateral aspect of the renal cortex.
Contrast-enhanced axial computed tomography scan obtained through the kidneys in the same patient as in the previous image. The image shows patchy tumor enhancement, with displacement of part of the normal lateral aspect of the renal cortex.
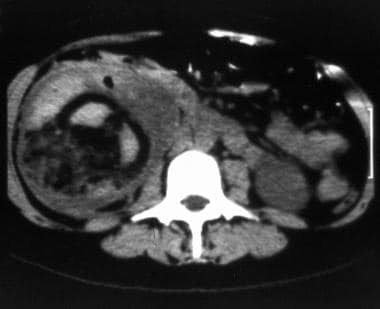 Nonenhanced computed tomography (CT) scan obtained in a 28-year-old pregnant woman (at 26 weeks' gestation) who presented with sudden-onset right upper quadrant abdominal pain and hypotension. An ultrasonogram (not shown) depicted a complex mass that replaced the right kidney; this finding was suggestive of a tumor that had ruptured into the perinephric space and retroperitoneum. This CT scan, obtained through the mid portions of the kidneys, shows a mixed-attenuation mass interspersed with areas of low attenuation (fat) and areas of high attenuation (blood).
Nonenhanced computed tomography (CT) scan obtained in a 28-year-old pregnant woman (at 26 weeks' gestation) who presented with sudden-onset right upper quadrant abdominal pain and hypotension. An ultrasonogram (not shown) depicted a complex mass that replaced the right kidney; this finding was suggestive of a tumor that had ruptured into the perinephric space and retroperitoneum. This CT scan, obtained through the mid portions of the kidneys, shows a mixed-attenuation mass interspersed with areas of low attenuation (fat) and areas of high attenuation (blood).
 Enhanced computed tomography scan obtained in the same patient as in the previous image. The image shows patchy renal cortical enhancement around the tumor. Note the retroperitoneal stranding behind the tumor. The final diagnosis was spontaneous rupture of an angiomyolipoma.
Enhanced computed tomography scan obtained in the same patient as in the previous image. The image shows patchy renal cortical enhancement around the tumor. Note the retroperitoneal stranding behind the tumor. The final diagnosis was spontaneous rupture of an angiomyolipoma.
In older, nonspiral CT scanners, contiguous 5-mm transaxial sections, imaged both before and after contrast enhancement, are used in the typical examination. [28] In smaller lesions, even thinner sections (1.5- or 3.0-mm sections) may be required to improve fat sensitivity. Achieving good fat sensitivity is more difficult with slower scanning times; sensitivity is further limited by breath-hold techniques.
Spiral CT scanning enables continuous scanning of complete anatomic volumes, which is particularly important for the characterization of small angiomyolipomas. Enhancement varies because of the vascular and muscle components. Hemorrhagic, necrotic, and cystic areas, as well as distorted or dilated calyces, contribute to the heterogeneity of these lesions. With CT scanning, particularly spiral and multisection CT scanning, optimal visualization of blood vessels and aneurysms in the vascular phase of the bolus of injected contrast agent may be achieved.
Patel et al studied the radiologic characteristics of renal masses in 12 individuals with tuberous sclerosis complex (TSC). [29] Using serial CT scans to examine how renal cell carcinoma may be differentiated from other masses, the authors measured the CT scanning density of all masses and categorized the masses as simple cysts, complex cysts, angiomyolipomas, or indeterminate solid masses. Subjects underwent regular follow-up with repeat CT scans or MRIs and interval renal ultrasonography. Rapidly growing indeterminate masses were considered suspicious for renal cell carcinoma; biopsy or nephrectomy of the masses followed. A median of 4 years of comparative data were available. [29]
In the Patel study, of the solid masses, 133 were typical angiomyolipomas and 52 were indeterminate. On follow-up, 3 indeterminate masses showed rapid growth (>0.5 cm/yr), 1 of which proved to be a renal cell carcinoma on biopsy. The remaining 2 indeterminate masses were found to be minimal-fat angiomyolipomas; the remainder of the masses showed either no growth or slow growth. The authors concluded that many renal masses associated with TSC are radiologically indeterminate. A growth threshold of >0.5 cm/yr identified the only renal cell carcinoma in the study (0.5% of all masses). Patel et al recommended that individuals with TSC have annual radiologic follow-up of indeterminate renal masses. [29]
Angiomyolipoma with minimal fat: differentiation from renal cell carcinoma at biphasic helical CT
Differentiating angiomyolipoma with minimal fat from a renal cell carcinoma on biphasic CT scanning may be problematic. Kim et al classified the renal tumor enhancement patterns following the administration of iodinated contrast. [30]
An early washout pattern was considered to be present when a tumor showed peak enhancement in the corticomedullary phase and then demonstrated a washout of at least 20 HU in the early excretory phase; a gradual enhancement pattern was considered to be present when the tumor attenuation value in the early excretory phase was at least 20 HU greater than it was in the corticomedullary phase; and a prolonged enhancement pattern was considered to be present when the difference in tumor attenuation between the corticomedullary and early excretory phases ranged from -20 to 20 HU. The authors found that the most significant predictors of angiomyolipoma with minimal fat were homogeneous enhancement and a prolonged enhancement pattern.
The positive and negative predictive values of homogeneous enhancement for differentiating angiomyolipoma with minimal fat from renal cell carcinoma were 83% and 94%, respectively. For the prolonged enhancement pattern, the positive and negative predictive values were 65% and 88%, respectively. Kim et al concluded that biphasic helical CT scanning is useful in the differentiation of angiomyolipoma with minimal fat from renal cell carcinoma. [30] Homogeneity of tumor enhancement and a prolonged enhancement pattern are the most valuable CT scan findings for differentiating between angiomyolipoma with minimal fat and renal cell carcinoma. Other findings, including tumor attenuation on unenhanced scans, amount of tumor enhancement, intratumoral calcification, and patient sex, provide supplementary information.
Chaudhry et al retrospectively studied small solid renal masses to determine whether minimal-fat renal angiomyolipoma can be differentiated from clear-cell or papillary renal cell carcinoma using attenuation measurement histogram analysis with unenhanced CT scanning. The authors concluded that attenuation measurement histogram analysis cannot reliably differentiate minimal-fat renal angiomyolipoma from renal cell carcinoma. [31]
Magnetic Resonance Imaging
On T2-weighted MR images, fat-rich angiomyolipomas are usually hyperintense as compared to renal parenchyma, but signal intensities vary according to the amount of fat. Angiomyolipomas with a large amount of fat are hyperintense because of lengthening T2 relaxation time. The lesion has hyperintense foci within the hypointense background because small fat foci are scattered among muscles, vessels, or both. Fat-suppressed T2-weighted imaging is useful for identifying fat-rich AML because fat signal intensity is suppressed. On T2-weighted images, fat-poor AML is slightly hypointense compared with renal parenchyma. [2, 22, 23]
The characteristic appearances of angiomyolipomas with MRI include variable areas of high signal intensity within the tumor on both T1-weighted and T2-weighted images. On a nonenhanced T1-weighted image, high signal intensity is present because of the fat content. On T2-weighted images, the signal remains isointense relative to that of perinephric fat. However, areas of high signal intensity on T1-weighted images are not pathognomonic of fat, and blood and pockets of fluid of high protein content may have a similar appearance. Intratumoral fat is best demonstrated with fat-suppression techniques. The in-phase and out-of-phase T1-weighted imaging technique is extremely sensitive to small quantities of fat. [32] MRI studies may show the rare complication of regional lymph node involvement and invasion of the renal vein and IVC.
On MRI, changes in signal intensity that occur as a result of the intrinsic differences in the resonant frequencies of precessing protons are known as the chemical shift phenomenon. [33, 15] This phenomenon has been used as a diagnostic tool; by demonstrating the inherent differences in resonant frequencies of fatty tissue and water, lipid-containing tumors may be identified. Although some success has been achieved in the diagnosis of fatty tumors such as angiomyolipomas, chemical shift (in-phase and out-of-phase imaging) probably is less likely to depict fat in an angiomyolipoma, because fat is macroscopic; chemical shift imaging is more likely to demonstrate microscopic fat, such as that in a renal cell carcinoma. A standard chemically selective fat-saturated technique better depicts the signal-intensity dropout of fat in an angiomyolipoma because this technique better depicts macroscopic fat. [16, 17, 34]
Traditionally, angiomyolipoma has been diagnosed by comparing T1-weighted images incorporating frequency-selective fat suppression with T1-weighted images without frequency-selective fat suppression. Angiomyolipomas may also be diagnosed using opposed-phase chemical shift artifact. Israel et al investigated the use of opposed-phase chemical shift MRI in the diagnosis of renal angiomyolipoma. [18]
Two types of edge artifacts have been described with chemical shift MRI: the chemical shift artifact and the India ink artifact. The chemical shift artifact is dependent on the receiver bandwidth and the shape and orientation of the fat–water interface. The India ink artifact is caused by the presence of fat and water protons within the same imaging voxel; this results in signal loss. The India ink artifact may be recognized on opposed-phase MRIs as a characteristic sharp black line at fat–water interfaces. Because the India ink artifact is a result of fat- and water-proton phase cancellation in all directions, the artifact occurs along the entire border of fat–water interface, not only in the frequency-encoding direction.
In addition, because most angiomyolipomas contain macroscopic fat, the India ink artifact appears at all interfaces of the tumor with the kidney or at the interfaces of the fatty and nonfatty portions of the mass. Other renal masses do not contain macroscopic fat; for that reason, the India ink artifact appears at the interface of the renal mass with perinephric fat when the mass is exophytic. Thus, the diagnosis of angiomyolipoma is indicated when the India ink artifact is present at a renal mass–kidney interface or within a renal mass.
Hindman et al concluded that the diagnostic accuracy of opposed-phase and in-phase gradient echo MR imaging for the differentiation of minimal-fat angiomyolipoma and clear cell renal cell carcinoma is poor. [19]
Scialpi et al found quantitative analysis of signal intensity variations during dynamic contrast-enhanced MRI with fat suppression useful in the characterization of small renal lesions. [35] Angiomyolipomas had an early peak mean percentage of enhancement at 30 s, even though the tumors remained hypointense in comparison to the renal cortex. This finding was caused by the shift from low signal intensity on baseline fat-suppressed sequences to high signal intensity for lesion vascularity as soon as the contrast material (gadolinium) was injected. Subsequently, a vascular washout of gadolinium demonstrated a decline in the percentage of enhancement to values similar to that of hypovascular renal cell carcinomas from 90 to 210 s.
Ultrasonography
The most characteristic ultrasonographic feature of an angiomyolipoma is its echogenicity; however, angiomyolipomas may also cause acoustic shadowing. [20] The echogenic appearance of the tumor is thought to be related to its fat content and the presence of multiple tissue interfaces within it. However, this appearance in a mass is not pathognomonic for angiomyolipomas; renal cell carcinoma has the same appearance. (See the images below.) Angiomyolipomas are round or oval cortical tumors; they tend to be well circumscribed, with an echogenicity similar to that of the echogenic renal sinus. Because of their intense echogenicity, angiomyolipomas as small as a few millimeters in diameter may be identified. Less echogenic areas within the tumor are related to hemorrhage, necrosis, or dilated calyces. A reduction of echogenicity in angiomyolipomas is thought to be related to a decrease in the quantity of fat and to an increase in the prominence of myogenic components. Doppler ultrasonography may be used to confirm the rare complication of extension into the renal vein and the IVC. [2, 22, 23, 7]
Renal ultrasonogram obtained in a 12-year-old boy with known tuberous sclerosis. Note the multiple echogenic tumors of varying sizes in both kidneys. This oblique sagittal scan through the left kidney shows a 4-cm echogenic mass (arrow) on the inferior aspect of the kidney that anteriorly displaces the renal sinus (S).
Renal ultrasonogram depicting many tumors in the right kidney. The arrow marks an echogenic 1-cm lesion (same patient as in the previous image).
Ultrasonogram obtained in a 48-year-old man who presented with dyspepsia and right upper quadrant discomfort. The patient was referred for a gallbladder ultrasonogram. The gallbladder was normal, but a solid 18-mm mass was present in the upper pole of the right kidney; it was isoechoic relative to the renal sinus.
In a case series with pathologically proven renal cell carcinomas, 32% of tumors with a diameter of 3 cm or less were echogenic. [36] Not all angiomyolipomas are hyperechoic because the tumor constituents vary, and the fat content may be low. Hemorrhage, necrosis, and dilated calyces also may alter the echogenicity of the tumor. [37]
In a mass with typical ultrasonographic features, fatty attenuation on plain abdominal radiographs, planar tomograms, and CT scans is virtually diagnostic of angiomyolipomas. However, an angiomyolipoma is not the only renal tumor that may contain fat. Rarely, but most importantly, fat may be found in a renal cell carcinoma because of the invasion of perinephric fat or metaplasia in the tumor. Intratumoral fat has also been found in renal lipomas, liposarcomas, Wilms tumors, teratomas, xanthogranulomatous pyelonephritis, and oncocytomas (engulfing of renal sinus fat).
If fat cannot be ultrasonographically demonstrated within a renal mass in a patient with tuberous sclerosis, a diagnosis of renal cell carcinoma must be considered. Rapidly enlarging lesions or dystrophic calcification within a mass may suggest the diagnosis of angiomyolipoma. Although the natural history of renal cell carcinoma in tuberous sclerosis is not well known, the risk of metastases likely increases with the size of the tumor; the risk is probably very low in tumors that are less than 3 cm in diameter. Therefore, consideration of nephron-sparing surgery may be reasonable in patients with tuberous sclerosis who have lesions without demonstrable fat that are enlarging and are close to or greater than 3 cm in diameter.
Marked echogenicity in a renal mass is not pathognomonic of angiomyolipomas. Other tumors, including renal cell carcinoma, may be hyperechoic. Tumors that are echogenic on ultrasonograms should be further investigated with CT scans, and the fat content of the tumor should be assessed.
A false-negative diagnosis may occur in cases involving a hemorrhagic or infarcted tumor, as well as in cases involving a tumor that has little fat. Also, a scar in the periphery of the kidney may be filled with intraperitoneal or omental fat; such a scar may have ultrasonographic features typical of an angiomyolipoma.
Angiography
Before the advent of ultrasonography, CT scanning, and MRI, much effort went into identifying angiographic characteristics that allow angiomyolipomas to be distinguished from renal cell carcinoma. Among radiologists, there is controversy regarding the reliability of angiography in the differentiation of these tumors.
About 95% of angiomyolipomas are hypervascular, with enlarged interlobar and interlobular arteries. The intratumoral arteries are tortuous, irregular, and aneurysmal. Venous pooling has a sunburst, whorled, and onion-peel appearance. Usually, no arteriovenous (AV) shunting is present. The following findings suggest an angiomyolipoma: the presence of multisacculated pseudoaneurysms; a sunburst appearance on the capillary nephrogram; an onion-skin appearance of the peripheral vessels in the venous phase; and the absence of AV shunting.
CT scanning has superseded angiography as a diagnostic tool; CT scanning is noninvasive, its results are more reproducible, and it is less dependent on operator technique and interpretation. Currently, angiography is reserved for use in transcatheter embolization to control bleeding caused by angiomyolipomas.
A significant finding in cases of angiomyolipoma is the lack of AV shunting on angiograms. However, AV shunting has been reported in cases of angiomyolipoma; therefore, it cannot be used to distinguish an angiomyolipoma from renal cell carcinoma. A reduction in the blood flow of a mass in response to epinephrine is characteristic of a benign lesion. The absence of this reduction in response to epinephrine was thought to be specific for malignant tumors, but such reduction in blood flow has been demonstrated to occur in cases of angiomyolipoma.
Questions & Answers
Overview
What is kidney angiomyolipoma?
What are the preferred imaging modalities for kidney angiomyolipoma?
What is the prevalence of kidney angiomyolipomas?
Which patients require routine follow-up after detection of a kidney angiomyolipoma?
How are kidney angiomyolipomas detected?
Which findings on radiography or IV urography are characteristic of kidney angiomyolipoma?
Which findings on CT scan are characteristic of kidney angiomyolipoma?
Which MRI findings are characteristic of kidney angiomyolipoma?
Which ultrasonography findings are characteristic of kidney angiomyolipoma?
What is the role of nuclear imaging in the management of kidney angiomyolipoma?
What is the role of angiography in the diagnosis of kidney angiomyolipoma?
-
Renal ultrasonogram obtained in a 12-year-old boy with known tuberous sclerosis. Note the multiple echogenic tumors of varying sizes in both kidneys. This oblique sagittal scan through the left kidney shows a 4-cm echogenic mass (arrow) on the inferior aspect of the kidney that anteriorly displaces the renal sinus (S).
-
Renal ultrasonogram depicting many tumors in the right kidney. The arrow marks an echogenic 1-cm lesion (same patient as in the previous image).
-
Selective right renal angiogram showing multiple avascular tumors. The tumors are small (same patient as in the previous image).
-
Selective left renal angiogram showing 2 tumors, which are larger than those in the previous image (same patient as in the previous image). The final diagnosis was multiple renal angiomyolipomas in a patient with tuberous sclerosis.
-
Computed tomography scan obtained in a 15-year-old boy with tuberous sclerosis (under surveillance). The image shows rapid growth in a right renal lesion with mixed attenuation. The final diagnosis was tuberous sclerosis–associated angiomyolipoma.
-
Computed tomography (CT) scan obtained in the same patient as in the previous image. The image shows the technique of CT scanning-guided biopsy with a Tru-cut needle.
-
Nonenhanced axial computed tomography scan through the kidneys. The image shows a space-occupying lesion of mixed attenuation interspersed with areas of fat attenuation. The final diagnosis was sporadic angiomyolipoma.
-
Contrast-enhanced axial computed tomography scan obtained through the kidneys in the same patient as in the previous image. The image shows patchy tumor enhancement, with displacement of part of the normal lateral aspect of the renal cortex.
-
Nonenhanced computed tomography (CT) scan obtained in a 28-year-old pregnant woman (at 26 weeks' gestation) who presented with sudden-onset right upper quadrant abdominal pain and hypotension. An ultrasonogram (not shown) depicted a complex mass that replaced the right kidney; this finding was suggestive of a tumor that had ruptured into the perinephric space and retroperitoneum. This CT scan, obtained through the mid portions of the kidneys, shows a mixed-attenuation mass interspersed with areas of low attenuation (fat) and areas of high attenuation (blood).
-
Enhanced computed tomography scan obtained in the same patient as in the previous image. The image shows patchy renal cortical enhancement around the tumor. Note the retroperitoneal stranding behind the tumor. The final diagnosis was spontaneous rupture of an angiomyolipoma.
-
Ultrasonogram obtained in a 48-year-old man who presented with dyspepsia and right upper quadrant discomfort. The patient was referred for a gallbladder ultrasonogram. The gallbladder was normal, but a solid 18-mm mass was present in the upper pole of the right kidney; it was isoechoic relative to the renal sinus.
-
Part of an intravenous urogram series obtained in the same patient as in the previous image. The radiograph shows a hypoattenuating exophytic mass (arrow).
-
Nonenhanced axial computed tomography scan obtained through the upper pole of the kidneys in the same patient as in the previous image. Image shows a hypoattenuating (15 HU) exophytic mass (arrow).
-
Axial fat-suppressed magnetic resonance image obtained through the upper poles of the kidneys in the same patient as in the previous image. Image shows a lesion of high signal intensity with tiny areas of intratumoral fat (which had low signal intensity on fat-suppressed images). The final diagnosis was renal cell carcinoma with fatty metamorphosis.







