Practice Essentials
Epidermoid cysts (also called epidermoid tumors) are benign congenital lesions of ectodermal origin. They account for approximately 1% of all intracranial tumors. Although these lesions are congenital, patients are usually not symptomatic until they are 20-40 years of age. The usual locations of epidermoid cysts are the parasellar region and cerebellopontine angle, and it is less commonly located in sylvian fissure, suprasellar region, cerebral and cerebellar hemispheres, and lateral and fourth ventricles. Epidermoid cysts located in the posterior fossa usually arise in the lateral subarachnoid cisterns, and they are rarely located in the brain stem. [1, 2, 3, 4, 5]
Epidermoid tumors are generally slow-growing tumors and are thought to develop between the third and fifth weeks of gestation from ectodermal remnants during neural tube formation in embryogenesis. Because they grow slowly, they are typically moderately large when discovered. Patients with epidermoid cysts become symptomatic when the lesions compress the brainstem or stimulate cranial nerves. [2, 3]
Computed tomography (CT) scanning and magnetic resonance imaging (MRI) are both helpful in diagnosing epidermoids. [6, 7, 8] Although CT findings may be nonspecific, MRI findings are reliable in diagnosis and have a high degree of confidence. With CT scans, the differentiation between arachnoid cyst and epidermoid cyst may be difficult. [2, 9] Epidermoids can occur within the diploic space. On skull radiographs, these most commonly appear as lytic lesions with well-defined sclerotic borders.
On T1-weighted images, epidermoid cysts are generally slightly hyperintense or isointense relative to gray matter. More specifically, the T1-weighted signal intensity tends to vary with the lipid content, with the signal intensity being increased in lesions with a high lipid content and decreased in those with a low lipid content. [2, 10, 11, 12]
(See the image below.)
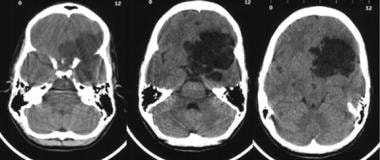 Computed tomography scans show a large mass with predominantly decreased attenuation, located in the middle cranial fossa with extension into the suprasellar cistern. Note the areas of heterogeneity within the mass.
Computed tomography scans show a large mass with predominantly decreased attenuation, located in the middle cranial fossa with extension into the suprasellar cistern. Note the areas of heterogeneity within the mass.
Computed Tomography
On CT scans, epidermoid lesions with decreased attenuation are most often extradural. They usually have the same attenuation as that of cerebrospinal fluid (CSF); this characteristic makes their differentiation from arachnoid cysts difficult on CT scans, but they are easily differentiated by MRI. Enhancement is rare but can sometimes be seen around the margin of the tumor. Calcification occurs in only 15-20% of cases. [2]
Rarely, epidermoids can appear hyperdense on CT scans secondary to high protein content. They are usually cystic and, in addition to their high protein content, usually have a high lipid content with mixed triglycerides containing polyunsaturated fatty acids.These atypical "white" epidermoids constitute only 3% of all epidermoids. They are sometimes called white epidermoids because they are are white or hyperintense on T1-weighted images. [13]
Epidermoids rarely occur in the parenchyma or the ventricle.
(A CT scan of an epidermoid is provided below.)
Computed tomography scans show a large mass with predominantly decreased attenuation, located in the middle cranial fossa with extension into the suprasellar cistern. Note the areas of heterogeneity within the mass.
Magnetic Resonance Imaging
MRI findings allow diagnosis of epidermoids with a high degree of confidence. In addition, the extent of disease is well depicted, which facilitates surgical planning. On T1-weighted images, these lesions are generally slightly hyperintense or isointense relative to gray matter. More specifically, the T1-weighted signal intensity tends to vary with the lipid content, with the signal intensity being increased in lesions with a high lipid content and decreased in those with a low lipid content. The lesions are usually isointense relative to CSF on T2-weighted images, but they may be slightly hyperintense. The center of the epidermoids usually has an internal architecture with areas of heterogeneity. [14, 15] Enhancement of portions of the rim may be seen after the administration of contrast material. The remainder of the lesion does not enhance. [2]
(See the MRI image below.)
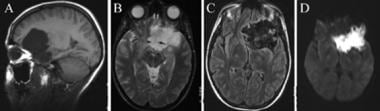 A: Sagittal T1-weighted magnetic resonance image (MRI) shows a low-signal-intensity mass that compresses the adjacent frontal and temporal lobes. B: The mass has very high signal intensity on this T2-weighted MRI. Note how it insinuates around the middle cerebral artery. C: On this fluid-attenuated inversion recovery (FLAIR) MRI, signal heterogeneity within the center of the mass is appreciated. D: The mass has extremely high signal intensity on this diffusion-weighted image.
A: Sagittal T1-weighted magnetic resonance image (MRI) shows a low-signal-intensity mass that compresses the adjacent frontal and temporal lobes. B: The mass has very high signal intensity on this T2-weighted MRI. Note how it insinuates around the middle cerebral artery. C: On this fluid-attenuated inversion recovery (FLAIR) MRI, signal heterogeneity within the center of the mass is appreciated. D: The mass has extremely high signal intensity on this diffusion-weighted image.
Proton density-weighted and then fluid-attenuated inversion recovery (FLAIR) images were first used to differentiate epidermoids from arachnoid cysts. These sequences demonstrate epidermoids as being hyperintense relative to CSF. Diffusion-weighted imaging can now be used to differentiate these entities, because epidermoids have markedly restricted diffusion and, therefore, high signal intensity on the diffusion-weighted trace images. The free water in arachnoid cysts has low signal intensity. Diffusion-weighted images are helpful in assessing residual epidermoid tumors after surgical resection. [16]
In a study by Hu et al, magnetic resonance diffusion-weighted imaging (MR DWI) sequences were found to facilitate diagnosis, with all intraparenchymal epidermoid cysts (6 cases) showing high hyperintensity on DWI and isointensity or slight hypointensity on apparent diffusion coefficient (ADC) maps. [17] Three of the cases were diagnosed with conventional MRI, but in the other 3 cases, the correct diagnosis could be made only with DWI. [17]
In rare cases, epidermoids with high protein content can appear hyperintense on T1-weighted images and hypointense on T2-weighted images. Epidermoids can also occur in unusual locations, such as the parenchyma or ventricle.
-
Computed tomography scans show a large mass with predominantly decreased attenuation, located in the middle cranial fossa with extension into the suprasellar cistern. Note the areas of heterogeneity within the mass.
-
A: Sagittal T1-weighted magnetic resonance image (MRI) shows a low-signal-intensity mass that compresses the adjacent frontal and temporal lobes. B: The mass has very high signal intensity on this T2-weighted MRI. Note how it insinuates around the middle cerebral artery. C: On this fluid-attenuated inversion recovery (FLAIR) MRI, signal heterogeneity within the center of the mass is appreciated. D: The mass has extremely high signal intensity on this diffusion-weighted image.






