Practice Essentials
Ectopic pregnancy occurs when the fetus develops outside of the uterine cavity, with the most common site of ectopic pregnancy (over 90%) being the fallopian tube. [1] Implantation may also occur in the abdomen, cervix, ovary, or cesarean scar. Women with clinical signs and physical symptoms of a ruptured ectopic pregnancy, such as hemodynamic instability or an acute abdomen, should be evaluated and treated urgently. Early diagnosis is aided by a high index of suspicion. [1] The incidence of ectopic pregnancy is 1-2% and the the most common cause of pregnancy-related death in the first trimester, accounting for about 10% of all pregnancy-related deaths. [2, 3, 4]
To diagnose an ectopic pregnancy, beta-HCG tests are required. A negative beta-HCG result effectively excludes the diagnosis of an ectopic or intrauterine pregnancy. In unstable patients, surgical evaluation and/or laparoscopy should be performed with or without culdocentesis. In patients with a stable clinical condition, transabdominal (TA) and endovaginal (EV) ultrasonography are performed. [5] The demonstration of an intrauterine gestational sac effectively excludes the diagnosis of an ectopic pregnancy. A search for a possible ectopic pregnancy as part of a heterotopic pregnancy should be attempted.
TA and EV ultrasonography are recommended in all studies. In a patient in stable condition, a full bladder should be present as a proper TA ultrasonography window. In unstable patients in whom an expeditious diagnosis is needed, the time delay for the bladder to fill may be undesirable. TA and/or EV ultrasonography may be performed in these patients with an empty bladder. [6, 7, 8, 9, 10, 11]
Both TA and EV examinations should still be performed with the acknowledgment of the limited, yet important, aspects of the TA portion of the examination. TA examination enables better evaluation of the superior uterus and superiorly positioned adnexa. It may aid detection of free peritoneal fluid and/or hemorrhage beyond the cul-de-sac. [12]
Transvaginal examination provides a detailed evaluation of the endometrial cavity and ovaries, but the high-frequency transducer that allows improved near-field resolution compared with TA examinations suffers from limited sound penetration (far-field imaging).
Medical management is often associated with follow-up imaging. [13, 14] Follow-up ultrasonography, along with follow-up beta-HCG levels, can be helpful if the diagnosis is unclear. A normal intrauterine pregnancy should demonstrate a 48-hour beta-HCG doubling time. [15] Magnetic resonance imaging (MRI) has been used as a problem-solving tool in patients in stable condition and with special circumstances. [5, 16, 17, 18, 19, 6]
MRI examination is time consuming and costly. Computed tomography (CT) scan findings are nonspecific in ectopic pregnancies and pose a hazard of ionizing radiation, which may be harmful to normal pregnancies.
Active research continues in an attempt to elucidate an ectopic-specific serum marker. Multiple markers show some diagnostic benefit in attempting to discriminate an ectopic pregnancy from a normal intrauterine gestation; however, their use is still widely in the investigative stage. Some of the many markers investigated include progesterone, cancer antigen-125 (CA-125), pregnancy-associated plasma protein A (PAPP-A), and activin A. [20, 21]
Guidelines
The American College of Obstetricians and Gynecologists (ACOG) recommends a transvaginal ultrasound (TVU) evaluation and confirmation of pregnancy by serum hCG level measurement for the evaluation of a suspected ectopic pregnancy. The guidelines note that serial evaluation with transvaginal ultrasonography, or serum hCG level measurement, or both, often is required to confirm the diagnosis. Every sexually active, reproductive-aged woman who presents with abdominal pain or vaginal bleeding should be screened for pregnancy, regardless of whether she is currently using contraception. Women who become pregnant and have known significant risk factors should be evaluated for possible ectopic pregnancy even in the absence of symptoms. [1]
The Royal College of Obstetricians and Gynaecologists (RCOG) also recommends TVU as the diagnostic tool of choice for tubal ectopic pregnancy. Tubal ectopic pregnancies are positively identified by visualizing an adnexal mass that moves separate to the ovary. [22]
According to the National Institute for Health and Care Excellence (NICE), when performing a transvaginal ultrasound scan in early pregnancy, look for the following signs indicating a tubal ectopic pregnancy: (1) an adnexal mass, moving separate to the ovary, comprising a gestational sac containing a yolk sac or (2) an adnexal mass, moving separately to the ovary, comprising a gestational sac and fetal pole (with or without fetal heartbeat). [23]
Magnetic Resonance Imaging
MRI findings that can suggest an ectopic pregnancy include the presence of (1) a tubal gestational sac; (2) a tubal hematoma, which is a hematoma suggested by the ring sign (peripheral hyperintensity) on T1-weighted images; (3) tubal wall enhancement; and (4) an adnexal mass with hemorrhagic fluid in the peritoneum. Blood is suggested by the presence of high-signal-intensity fluid on T1-weighted images. [24, 25, 26, 27, 28, 29, 18, 19]
The MRI characteristics of an ectopic pregnancy and its rupture are seen in the T2-weighted images below.
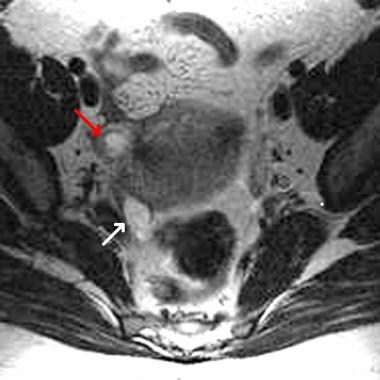 Axial T2-weighted fast spin-echo magnetic resonance image of the pelvis. This image shows an abnormal fluid-containing fallopian tube (red arrow) on the right side. A simple right ovarian cyst (white arrow) is also present.
Axial T2-weighted fast spin-echo magnetic resonance image of the pelvis. This image shows an abnormal fluid-containing fallopian tube (red arrow) on the right side. A simple right ovarian cyst (white arrow) is also present.
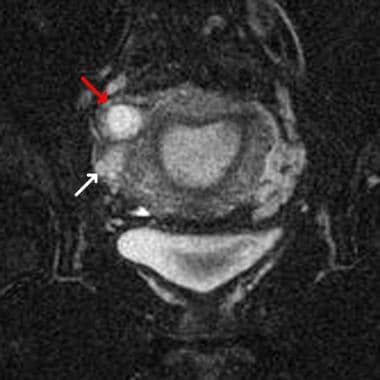 Coronal T2-weighted fat-saturated magnetic resonance image of the pelvis (same patient as in the previous image). This image shows an abnormal fluid-containing fallopian tube (red arrow) on the right side. A simple ovarian cyst (white arrow) is also present on the right.
Coronal T2-weighted fat-saturated magnetic resonance image of the pelvis (same patient as in the previous image). This image shows an abnormal fluid-containing fallopian tube (red arrow) on the right side. A simple ovarian cyst (white arrow) is also present on the right.
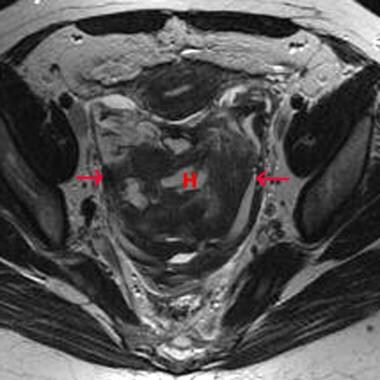 Axial T2-weighted fast spin echo magnetic resonance image of the pelvis (same patient as in the previous 2 images). After 1 week of conservative therapy, the ectopic pregnancy viewed in the previous 2 images ruptured. A large, mixed-signal-intensity hematoma is now present in the rectouterine pouch (noted by the H and arrows).
Axial T2-weighted fast spin echo magnetic resonance image of the pelvis (same patient as in the previous 2 images). After 1 week of conservative therapy, the ectopic pregnancy viewed in the previous 2 images ruptured. A large, mixed-signal-intensity hematoma is now present in the rectouterine pouch (noted by the H and arrows).
 Axial T2-weighted gradient-echo magnetic resonance image of the pelvis (same patient as in the previous 3 images). After 1 week of conservative therapy, the ectopic pregnancy viewed in the previous 3 images ruptured. A large mixed-signal-intensity hematoma is now present in the rectouterine pouch (noted by the H and arrows).
Axial T2-weighted gradient-echo magnetic resonance image of the pelvis (same patient as in the previous 3 images). After 1 week of conservative therapy, the ectopic pregnancy viewed in the previous 3 images ruptured. A large mixed-signal-intensity hematoma is now present in the rectouterine pouch (noted by the H and arrows).
MRI should be used only as a problem-solving tool in the patient who is in stable condition. This imaging modality is accurate in the characterization of tissue and in the detection and age determination of blood products. On MRI, high T1 signal intensity fluid in a fallopian tube is abnormal. [30] With a positive beta-HCG result, this finding suggests an ectopic pregnancy. Subacute blood products associated with an adnexal mass are also indicative of an ectopic pregnancy. MRI can additionally delineate confounding adnexal findings seen on ultrasonography, such as follicular or corpus luteum cysts.
Early intrauterine pregnancy or a missed abortion may be associated with normal MRI findings and thus falsely suggest an ectopic pregnancy. However, this scenario is not likely because of the high sensitivity of MRI in detecting associated fluid and blood products with true ectopic pregnancies.
The appearance of an adnexal mass is not necessarily specific on MRI. Corpus luteum cysts and other masses may be confused with ruptured or unruptured ectopic pregnancy. False-positive results can be caused by abnormal tubal fluid or enhancement, as seen with pelvic inflammatory disease and simple hydrosalpinx; however, these findings should be correlated with a positive beta-HCG.
Ultrasonography
Findings of an extrauterine ectopic pregnancy on ultrasonography include the following [6, 31, 32, 7, 8, 9, 10, 11] :
-
Live, extrauterine embryo
-
Absence of an intrauterine gestational sac
-
Free fluid (particularly hemorrhagic) in the pelvis or peritoneum
-
Adnexal mass [7]
-
Hematosalpinx
-
Adnexal ring sign and a "ring-of-fire" sign on color Doppler ultrasonographic images [33]
-
Absence of low-resistance endometrial arterial flow, which is an endometrial color Doppler ultrasonographic finding that is highly suggestive of intrauterine pregnancy
(See the images below.)
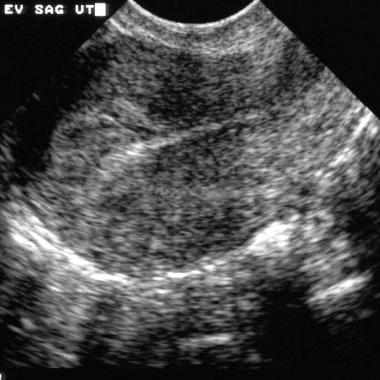 Sagittal endovaginal sonogram of the uterus. This image shows no evident intrauterine pregnancy.
Sagittal endovaginal sonogram of the uterus. This image shows no evident intrauterine pregnancy.
 Endovaginal sonogram (same patient as in the previous image). This image shows a coronal view of the adnexa. Hypoechoic fluid surrounds the fallopian tube.
Endovaginal sonogram (same patient as in the previous image). This image shows a coronal view of the adnexa. Hypoechoic fluid surrounds the fallopian tube.
 Endovaginal sonogram (same patient as in the previous 2 images). This image shows the tubal ring sign as well as diffuse thickening of the fallopian tube wall with minimal surrounding free fluid.
Endovaginal sonogram (same patient as in the previous 2 images). This image shows the tubal ring sign as well as diffuse thickening of the fallopian tube wall with minimal surrounding free fluid.
Findings of an interstitial ectopic pregnancy include the following:
-
Eccentric location of the gestational sac
-
Thinning or the absence of myometrium surrounding the sac
-
Interstitial-line sign, or a hyperechoic line extending from the central endometrial cavity to the peripheral interstitial pregnancy, which is created by the interstitial portion of the endometrium or fallopian tube
When correlating beta-HCG levels with ultrasonographic findings, it is important to take into account the standard of measurement. Both the 2IS and IRP systems are used to report beta-HCG values. An IRP value is approximately twice the corresponding 2IS value.
With a positive beta-HCG level greater than 1000 IU/mL (2IS standard) or 2000 IU/mL (IRP standard), a gestational sac should be identifiable within the uterus on transvaginal sonograms. [7, 8, 9] For TA scanning, a higher threshold of 1800 IU/mL (2IS standard) or 3600 IU/mL (IRP standard) should be used. An intrauterine pregnancy can be definitely diagnosed by the double-decidual-sac sign or by the demonstration of an embryo with a positive heartbeat. Cardiac activity should be identifiable in a fetus when it is found within a gestational sac during transvaginal ultrasonography with a mean diameter of 16 mm or a crown-rump length of 5 mm. [34]
If an intrauterine gestational sac is not found, an ectopic pregnancy must be considered. If the patient's beta-HCG concentration is below the threshold level and if the only finding is the lack of an intrauterine gestational sac, serial follow-up examinations and beta-HCG determinations are required. A normal intrauterine pregnancy should demonstrate a beta-HCG doubling time of 48 hours. [15] Below the threshold level, ultrasonography does not aid in differentiating an early intrauterine pregnancy, a missed abortion, and an ectopic pregnancy.
The double decidual sac found with an early intrauterine pregnancy can be difficult to distinguish from the pseudogestational sac, which is seen in 20-50% of ectopic pregnancies. The double decidual sac is 2 concentric hyperechoic rings created by hypoechoic fluid between the decidua parietalis and the decidua capsularis. This sign is in distinct contrast to a single hyperechoic layer found with a pseudogestational sac (see the images below). The lack of a yolk sac, the more-irregular contours, and the more-central location within the endometrial cavity also help in delineating a pseudogestational sac from an early intrauterine pregnancy.
 Endovaginal sonogram. This image shows a sagittal view of the uterus with a pseudogestational sac. Reactive changes secondary to an ectopic pregnancy are seen as hypoechoic material within the endometrial canal, which is outlined by a single hyperechoic rim. This should be contrasted with the dual hyperechoic lines that represent the dual decidual sac, an indicator of a normal intrauterine pregnancy.
Endovaginal sonogram (same patient as in the previous image). This image shows a coronal view of the adnexa. Hypoechoic fluid surrounds the fallopian tube.
Endovaginal sonogram. This image shows a sagittal view of the uterus with a pseudogestational sac. Reactive changes secondary to an ectopic pregnancy are seen as hypoechoic material within the endometrial canal, which is outlined by a single hyperechoic rim. This should be contrasted with the dual hyperechoic lines that represent the dual decidual sac, an indicator of a normal intrauterine pregnancy.
Endovaginal sonogram (same patient as in the previous image). This image shows a coronal view of the adnexa. Hypoechoic fluid surrounds the fallopian tube.
Further support of a pseudogestational sac can be demonstrated by the absence of low-resistance endometrial arterial flow on color Doppler ultrasonographic evaluation. The low pulsatility and the low-resistance flow are highly suggestive of an intrauterine pregnancy. This low-resistance flow should have a resistive index less than 0.6 or a peak systolic frequency of 0.8 kHz or greater. [35, 36]
The combination of the Doppler and ultrasonographic findings should be used to differentiate the early intrauterine pregnancy from a pseudogestational sac. However, Doppler ultrasonographic evaluation has not been shown to be of value when attempting to delineate an adnexal ectopic pregnancy from a corpus luteum cyst, particularly as corpus luteum cysts can demonstrate marked peripheral color Doppler ultrasonographic signal, simulating the ring-of-fire sign (see the image below). The intraovarian location is the main factor in distinguishing a corpus luteum cyst.
Endovaginal sonogram. This image shows a sagittal view of the uterus with a pseudogestational sac. Reactive changes secondary to an ectopic pregnancy are seen as hypoechoic material within the endometrial canal, which is outlined by a single hyperechoic rim. This should be contrasted with the dual hyperechoic lines that represent the dual decidual sac, an indicator of a normal intrauterine pregnancy.
The only specific sign of an ectopic pregnancy is the presence of a live extrauterine gestation. Free fluid is nonspecific and may present as anechoic or echogenic and in varying amounts. Simple free fluid and an empty uterus have a sensitivity of only 63% and a specificity of only 69%. [34] However, hyperechoic fluid and/or large amounts of free fluid are more suggestive of an ectopic pregnancy. [15, 37]
The remaining signs seen in ectopic pregnancy lack sufficient sensitivity and specificity to be used as sole indicators. Because of the variety of ultrasonographic findings, these must be correlated with the clinical presentation and further evaluated to differentiate a possible ectopic pregnancy from an alternate diagnosis.
There are no clear guidelines regarding if or when follow-up sonograms should be obtained. Follow-up examinations should be performed on an individual case basis, in coordination with patient's the clinical scenario and the beta-HCG levels.
False positives/negatives
False-positive ultrasonographic findings may be due to a missed abortion or an early normal intrauterine pregnancy (< 4.5 wk), without or with secondary findings of an adnexal mass. The latter scenario may include an intrauterine pregnancy with a hemorrhagic corpus luteum cyst or an intrauterine pregnancy with an adnexal mass, as can be found with concurrent appendicitis.
False-negative findings may be due to an intrauterine decidual reaction pseudosac that simulates an early intrauterine pregnancy. Approximately 8% of proven ectopic pregnancies are ultrasonographically normal on retrospective evaluation. [35] A concomitant intrauterine pregnancy and ectopic pregnancy (particularly in infertility patients) are other causes of false-negative findings for ectopic pregnancy.
As a note of caution, the limited far field of transvaginal ultrasonography can occasionally miss an ectopic pregnancy that is in a high position. Analysis of the patient's symptoms and placing a transducer on the area of maximal pain may aid the examination. The TA probe can help with this and provide a more global view of the pelvis and its contents.
-
Axial T2-weighted fast spin-echo magnetic resonance image of the pelvis. This image shows an abnormal fluid-containing fallopian tube (red arrow) on the right side. A simple right ovarian cyst (white arrow) is also present.
-
Coronal T2-weighted fat-saturated magnetic resonance image of the pelvis (same patient as in the previous image). This image shows an abnormal fluid-containing fallopian tube (red arrow) on the right side. A simple ovarian cyst (white arrow) is also present on the right.
-
Axial T2-weighted fast spin echo magnetic resonance image of the pelvis (same patient as in the previous 2 images). After 1 week of conservative therapy, the ectopic pregnancy viewed in the previous 2 images ruptured. A large, mixed-signal-intensity hematoma is now present in the rectouterine pouch (noted by the H and arrows).
-
Axial T2-weighted gradient-echo magnetic resonance image of the pelvis (same patient as in the previous 3 images). After 1 week of conservative therapy, the ectopic pregnancy viewed in the previous 3 images ruptured. A large mixed-signal-intensity hematoma is now present in the rectouterine pouch (noted by the H and arrows).
-
Sagittal endovaginal sonogram of the uterus. This image shows no evident intrauterine pregnancy.
-
Endovaginal sonogram (same patient as in the previous image). This image shows a coronal view of the adnexa. Hypoechoic fluid surrounds the fallopian tube.
-
Endovaginal sonogram (same patient as in the previous 2 images). This image shows the tubal ring sign as well as diffuse thickening of the fallopian tube wall with minimal surrounding free fluid.
-
Endovaginal sonogram. This image shows a coronal view of the pelvis. Moderate hypoechoic free fluid is associated with a large, heterogeneous, right adnexal mass.
-
Endovaginal sonogram (same patient as in the previous image). This image shows a coronal view of a right adnexal mass. An ectopic embryo is present within the heterogeneous right adnexal mass. The cursors denote the crown-rump length.
-
Endovaginal sonogram. This image shows a sagittal view of the uterus with a pseudogestational sac. Reactive changes secondary to an ectopic pregnancy are seen as hypoechoic material within the endometrial canal, which is outlined by a single hyperechoic rim. This should be contrasted with the dual hyperechoic lines that represent the dual decidual sac, an indicator of a normal intrauterine pregnancy.
-
Endovaginal sonogram (same patient as in the previous image). This image shows a coronal view of the right ovary. A corpus luteum cyst mimics an ectopic pregnancy. The cursors denote a hyperechoic clot within the cyst.
-
Endovaginal sonogram (same patient as in the previous 2 images). This image shows a sagittal view of the right ovary. A corpus luteum cyst mimics an ectopic pregnancy. The cursors denote a hyperechoic clot within the cyst. Note the thin rim of ovarian tissue surrounding the cyst.
-
Endovaginal sonogram (same patient as in the previous 3 images). This image shows a coronal view of the right adnexa. In this patient, the true ectopic pregnancy is identified as a large, heterogeneous adnexal mass surrounded by free fluid.
-
Endovaginal sonogram. This view shows a color Doppler image of the adnexa with the ring-of-fire sign. Marked hyperemia is present throughout the wall of an enlarged fallopian tube.







