Practice Essentials
Cystic fibrosis (CF) is a multisystemic, autosomal recessive disorder that predominantly affects infants, children, and young adults. [1, 2, 3] CF is a monogenic disease caused by mutations in the CFTR gene on chromosome 7, affecting the airways, pancreas, male genital system, intestine, liver, bone, and kidney. The lack of CFTR or the impairment of its function results in fat malabsorption and chronic pulmonary infections, which lead to bronchiectasis and progressive lung damage. [4] CF is the most common life-limiting genetic disorder in whites, with an incidence of 1 case per 3200-3300 newborns in the United States. Anderson first described the disease comprehensively in 1938. The term cystic fibrosis was coined because of the microscopic appearance of the pancreas.
CF is characterized by abnormal transport of chloride and sodium across the epithelium in all exocrine tissues, leading to thick viscous secretions in the lungs, pancreas, liver, intestine, and reproductive tract and to an increased salt content in sweat gland secretions. [5, 6]
Manifestations of CF involve the lung and gastrointestinal tract, including the pancreas. [7] CF lung disease is characterized by chronic airway inflammation and infection, leading to early structural changes of the airways, such as airway wall thickening and mucus plugging. These changes are thought to lead to the development of bronchiectasis, which is defined as an irreversible widening of the airway. [8]
Neurologic complications, although rare, have also been reporte. Causes of CNS impairment in patients with CF may include hypoxia, vitamin E or vitamin K deficiency, antibiotic adverse effects, fluid depletion or imbalance, use of psychotropic agents, and stroke from paradoxical emboli. . [9]
(See the cystic fibrosis images below.)
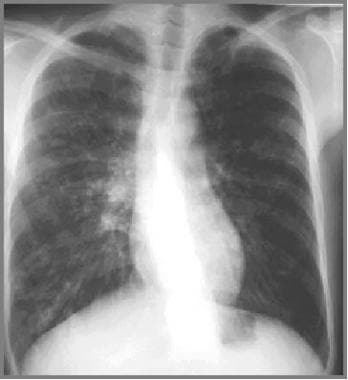
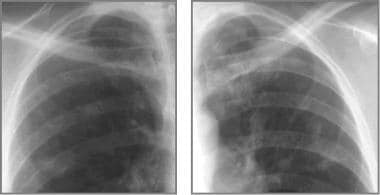
 Cystic fibrosis, thoracic. Young man with a history of cystic fibrosis has hyperinflation and predominantly upper lobe bronchiectasis.
Cystic fibrosis, thoracic. Young man with a history of cystic fibrosis has hyperinflation and predominantly upper lobe bronchiectasis.
 Cystic fibrosis, thoracic. Patient with a history of cystic fibrosis has complete right lung atelectasis with extreme bronchiectasis. Marked hyperinflation of the left lung is noted.
Cystic fibrosis, thoracic. Patient with a history of cystic fibrosis has complete right lung atelectasis with extreme bronchiectasis. Marked hyperinflation of the left lung is noted.
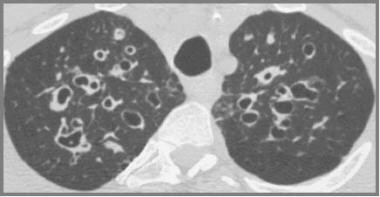
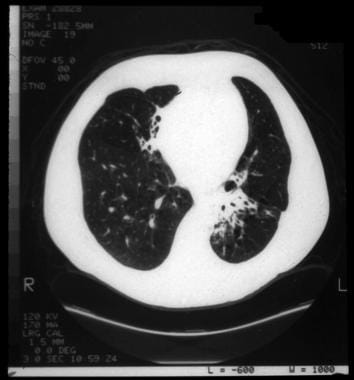
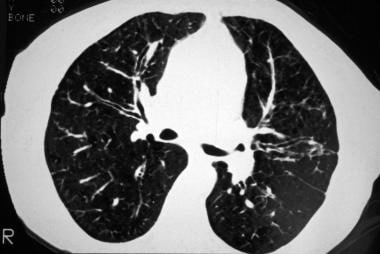 Cystic fibrosis, thoracic. High-resolution CT image shows bronchial wall thickening (tram lines), predominantly in the upper lobes.
Cystic fibrosis, thoracic. High-resolution CT image shows bronchial wall thickening (tram lines), predominantly in the upper lobes.
 Cystic fibrosis, thoracic. String-of-pearls sign in the left lower lobe in a patient with cystic fibrosis. The soft tissue surrounding each "pearl" indicates focal atelectatic, fibrotic lung.
Cystic fibrosis, thoracic. String-of-pearls sign in the left lower lobe in a patient with cystic fibrosis. The soft tissue surrounding each "pearl" indicates focal atelectatic, fibrotic lung.
The diagnosis of cystic fibrosis is based on compatible clinical findings, with biochemical or genetic confirmation. So far, the sweat chloride test is the mainstay of laboratory confirmation. However, CF is a complex syndrome, and the clinical manifestations are sometimes subtle. Also, the family history is not always straightforward. Therefore, a battery of clinical or genetic tests and a high index of suspicion are often required to establish the diagnosis, especially in adolescents and young adults. [10]
Radiologic modalities used to diagnose or follow up thoracic CF invariably include chest radiography and CT of the thorax. [11, 12, 13] CT of the sinuses or abdomen is occasionally used, as are nuclear medicine studies, ultrasonography, and angiography. [14, 15, 16, 17, 18, 19, 20]
Sweat chloride test
The sweat chloride test remains the criterion standard for the diagnosis of cystic fibrosis. Most diagnostic laboratories in the US screen for 20-30% of the most common mutations, identifying approximately 90% of chromosomes affected in CF. The remaining 10% of affected chromosomes comprise more than 400 different pathologic mutations of CFTR. As a result, more-extensive screening is impractical. A sweat chloride value greater than 60 mEq/L distinguishes CF from other forms of chronic pulmonary disease. However, normal sweat chloride concentrations may be observed in approximately 1% of patients with CF, who have unusual genotypes (ie, 3849+10kb CT or poly T defects).
The test is performed by collecting sweat with pilocarpine iontophoresis on 2 or more occasions and by chemically determining the chloride concentration. Conditions other than CF that are associated with elevated sweat electrolyte concentrations include adrenal insufficiency, anorexia nervosa, celiac disease, malnutrition, hypothyroidism, and congenital metabolic diseases. [21]
The incidence of erroneous sweat test results is probably in the range of 10-15%, and most errors represent false-positive results. Most errors are caused by the use of unreliable methodology, inadequate sweat collection, technical mistakes, and misinterpretation of results; therefore, the test should be performed in a laboratory that regularly uses extreme care with assays. False-negative results can be seen in hypoproteinemic edema and with the concurrent administration of steroids.
Nasal potential-difference measurements
Abnormalities in epithelial chloride secretions can be demonstrated in most patients with CF by evaluating the nasal transepithelial potential difference in the basal state. This test is performed after nasal perfusion with amiloride and after nasal perfusion with a chloride-free solution.
Three features distinguish cystic fibrosis:
-
Increased basal potential difference, which reflects enhanced Na+ transport across a relatively chloride-impermeable barrier.
-
Greater inhibition of potential difference after nasal perfusion with the Na+ channel inhibitor amiloride, which reflects inhibition of accelerated Na+ transport.
-
Little or no change in potential difference in response to perfusion of the nasal epithelial surface with a chloride-free solution in conjunction with isoproterenol, which reflects an absence of CFTR-mediated chloride secretion.
An increased (ie, more negative) basal nasal potential difference is strong evidence of CF. The presence of nasal polyps or inflamed mucosa may yield a false-negative result. The presence of a large response to chloride-free perfusion is strong evidence against CF. The test should be performed only by experienced CF centers because standardization of the location of measurement is critical.
Immunoreactive trypsin test
Infants with CF have elevated blood levels of immunoreactive trypsin (IRT), which can be quantitated by means of radioimmunoassay or enzyme-linked immunoassay. A negative result is not informative in patients older than 8 weeks. The test may be particularly useful for small or malnourished infants in whom the sweat chloride test cannot be performed successfully. Overall, false-positive and false-negative rates are relatively high.
Stool fecal fat and pancreatic-enzyme secretion tests
Stool fecal fat and pancreatic-enzyme secretion can be measured by collecting duodenal fluids after simulation with secretin and pancreatozymin. Decreased levels of pancreatic enzymes or elevated stool fat are expressed as the percentage of ingested fat in a 72-hour stool collection and can be indicative of CF, respectively.
Molecular diagnostic tests
The molecular diagnosis is usually based on a direct mutation analysis. [22] A variety of techniques are used to identify specific known mutations in the nuclear type sequence of the CFTR gene. These technologies enable clinicians to identify and confirm the diagnosis, especially in patients with an atypical presentation. For example, patients may have borderline or normal sweat chloride concentrations in the presence of several characteristic phenotypic manifestations, or the suspicion may be high in the absence of clinical features. Other circumstances, such as in prenatal screening, may also warrant these tests. [23]
Early diagnosis is important because early aggressive therapeutic intervention is associated with improved nutritional status, decreased morbidity, and decreased deterioration in lung function. However, screening programs have not been adopted widely.
A 5-year randomized study in Wisconsin did not identify any clear health benefits from routine screening. [24] Nevertheless, the identification of patients with CF in the newborn period provides a population for studying the mechanism of early lung injury and the effectiveness of no therapeutic delay in preventing the onset of lung damage.
Radiography
Chest radiography is not considered an essential technique to use in the diagnosis of cystic fibrosis; however, it may play a strong corroborative role in diagnosis of the disease. [25] Chest radiography has also been the mainstay in the longitudinal assessment of patients with CF. [26, 27, 28]
Chest radiographic findings are not specific or diagnostic because they overlap with other disorders, particularly those characterized by inflammatory or destructive changes of the airways. Early in the course of disease, chest radiographs may be normal, or they may show minor manifestations such as mild hyperinflation and minimal bronchial thickening.
Normal chest radiographic findings may be seen in infancy and even in older children with mild pulmonary involvement, though this is uncommon. The usefulness of a chest radiograph during an exacerbation of CF in adult patients is also debated. Some study results support the lack of a precise correlation between the radiographic picture and the clinical manifestations of exacerbation, with a reported sensitivity and specificity of 56% and 78%, respectively. Chest radiography is predominantly used to exclude pneumothorax or airspace disease such as pneumonia or atelectasis.
Thoracic CT scanning
High-resolution CT (HRCT) improves spatial resolution, and it may be useful in the evaluation of minimally affected individuals. Multiple studies have shown that CT is more sensitive and specific than chest radiography in demonstrating bronchiectasis and other abnormalities in patients with normal chest radiographic results. [29, 30, 31, 32] HRCT can demonstrate bronchiectasis and mucous plugging to the level of the fifth- or sixth-order bronchi. With expiratory imaging, focal areas of air trapping can be identified as an indication of small-airway disease. [33, 34, 35, 36, 37, 38]
The sensitivity and specificity of regular CT (with 10-mm sections) for bronchiectasis is 60-80% and 90-100%, respectively. Use of 1.5- to 5-mm resolution improves the sensitivity and specificity to 87% and 90%, respectively.
Santamaria et al addressed the role of HRCT in assessing CF, comparing HRCT scores, chest radiographic findings, pulmonary function test (PFT) results, and clinical scores. [39] They found that HRCT of the chest is most useful in the identification of early lung abnormalities in patients with CF with mild respiratory symptoms, whereas in established disease, chest radiography is still the first-line imaging technique. In patients with advanced disease, HRCT may be useful in the evaluation of specific lung changes, when more aggressive treatment, such as chest surgical interventions, is indicated.
HRCT of the chest is useful and sensitive in studying responses to therapy in patients with CF lung disease, even in patients younger than 5 years. [40, 41, 42] The clinical utility and practicality of this technique is unclear, but HRCT could be used to assess the effectiveness of the therapeutic modality, and its results could be a useful outcome surrogate in CF. [43]
Compared with other findings, total reversible HRCT scores are better correlated with PFT results and acute changes in clinical scores during exacerbations of CF. The greatest change is seen in the mucous-plugging subcomponent of the HRCT score and then in the peribronchial thickening.
Serial CT scans allow assessment of the evolution of pulmonary abnormalities in CF patients. Helbich et al suggest that CT seems to have advantages over PFT and clinical scoring in the evaluation of pulmonary changes over time. [44] Therefore, some have suggested that HRCT scoring may provide a sensitive method of monitoring pulmonary disease status; this could possibly be helpful in follow-up of small children who are too young to cooperate with spirometry. Some studies have also found a correlation of CT findings and scores with serum immunoglobulin levels, but no relationship to genotypes has been observed.
Characteristic CT findings occasionally suggest a specific diagnosis, which may not have been under clinical consideration in the differential diagnosis of CF. The pattern and distribution of abnormalities revealed by HRCT in patients with bronchiectasis are influenced by the underlying cause. For example, bilateral bronchiectasis predominantly in the upper lobe is most common in patients with CF and allergic bronchopulmonary aspergillosis (ABPA); unilateral upper-lobe predominance is seen in patients with tuberculosis; and lower-lobe predominance is seen in patients after a childhood viral infection. [45]
Adult CF and ABPA involve disease that is more extensive than idiopathic bronchiectasis, independent of other CT features (5 or 6 lobes involved). Central bronchiectasis is more commonly reported with ABPA, although the sensitivity of this finding as a diagnostic feature is only 37%. In syndromes with impaired mucociliary clearance, a lower-lobe involvement is more predominant, and bronchiectasis in hypogammaglobulinemia is characterized by less dilatation of the bronchial lumen as compared to that seen in idiopathic bronchiectasis.
CT of the thorax can also greatly facilitate the diagnosis and management of pneumothorax in patients with complex cystic disease.
Regardless of the radiologic findings, CF is less commonly considered in the adult patient, because of the traditional belief that CF is a childhood disease. Amorosa et al reviewed radiographs in pediatric and adult cases that showed disease of similar extent and severity. [46] They found that radiologists made the correct diagnosis in 40% of the pediatric cases, compared to 14% in the adult cases.
Despite the capabilities of HRCT, clear guidelines for its use in the care of children with CF are still lacking. The advantage of detecting early changes on CT images awaits additional confirmation. Whether the early introduction of therapeutic interventions significantly affects the final outcome of the disease is yet to be demonstrated.
HRCT does not provide sufficient additional information to justify the additional cost and radiation exposure in routine follow-up. With the advent of new therapies and with gene treatment raising the possibility of a cure, the need for a detailed evaluation of the lungs is great, and outcome measures for the new interventions and HRCT scanning should be considered. The value of HRCT in following up patients with CF is not yet clarified.
With regard to its value as a diagnostic tool, CT findings are of limited value in discriminating between bronchiectasis of CF and other causes in individual patients. However, differences in the distribution and morphology of bronchiectasis may be seen on CT scans in groups of patients with bronchiectasis due to different causes. Generally, the causes of bronchiectasis cannot be reliably identified on the basis of CT appearances alone.
Other radiologic modalities
The role of MRI in the evaluation of patients with CF is still being defined. [47, 48, 49] Pulmonary MRI can provide high-resolution images that are sensitive to early CF and specific to inflammation in CF lung disease. Contrast perfusion MRI can be used to identify changes in pulmonary and bronchial circulation that routinely occur in CF lung disease. Hyperpolarized-gas MRI is becoming more widespread and has been shown to have high sensitivity to early airway obstruction in CF via ventilation MRI. [50] In the depiction of bronchial wall thickening, bronchial dilatation, and mucous plugging, the resolution of MRI does not compare favorably with that of CT. [51]
Abdominal ultrasonography is commonly used to diagnose the complications of CF and its pancreatic and hepatobiliary manifestations. [52, 53]
The usefulness of lung scintigraphy is limited. The main problem is the correct clinical use of a test with such a high sensitivity and a high percentage of false-positive results. Hepatobiliary scans may have a role in evaluating hepatobiliary disease in neonates and children. [54]
Decreased bone density is common among patients with CF; this finding usually reflects a lack of control of the illness, and it often remains unfound with the usual investigations. If possible, dual x-ray absorptiometry should be part of the investigations in these patients. [55, 56]
Angiography
Bronchial arteriography is the preferred diagnostic and therapeutic examination in patients with CF and significant hemoptysis. [57]
Bronchial arteriography has a role in detecting the bleeding site. It is also useful in subsequent embolotherapy in patients with advanced CF and major or persistent and significant hemoptysis
Although hemoptysis is correlated with bronchial artery hypertrophy and a bronchopulmonary anastomosis within the bronchial walls, the role of prophylactic angiography for further interventions has not been studied. Angiography is invasive and usually performed in the setting of acute significant hemoptysis.
Radiologic intervention
Possible radiologic interventions in pulmonary cystic fibrosis include bronchial artery embolization (BAE), treatment with glycerin and amphotericin B, and bronchography.
BAE is a relatively safe and effective treatment of significant hemoptysis in patients with CF. [58]
Brinson et al reviewed a 10-year experience in the treatment of hemoptysis in 18 patients with CF. [59] The treatment included 36 BAE procedures for the control of hemoptysis. Most patients had severe lung disease (FEV1< 35%) with a high incidence of infection with multidrug-resistant bacteria. The overall effectiveness of BAE for the initial control of hemoptysis was 75% after 1 session, 89% after 2 sessions, and 93% after 3 sessions.
The patients in the Brinson et al study were followed up for a mean of approximately 22 months after BAE. The overall recurrence rate per episode was 46%, with a mean time for recurrence of approximately 12 months. The incidence of bleeding from nonbronchial systemic collateral vessels was high in patients who had undergone previous BAE. [59] Frazer et al reported 2 deaths associated with massive hemoptysis despite BAE and 3 patients with transient neurologic deficits during BAE (transverse myelitis). [60]
The direct intracavitary percutaneous instillation of glycerin and amphotericin B with CT guidance has shown promise in the treatment of symptomatic patients with mycetoma (aspergilloma) as a complication of a preexisting cavity with extensive bronchiectasis. In a study of 15 patients with bronchiectasis, the palliation of hemoptysis and sputum production occurred, with the diminishment or disappearance in serum precipitins. [38]
As the criterion standard as a diagnostic tool for bronchiectasis, bronchography has been almost completely replaced by HRCT. Indications for bronchography may still exist in select surgical candidates in whom CT shows predominant segmental or unilateral involvement. [61]
Moran et al compared noninvasive ventilation (NIV) with no NIV in patients with cystic fibrosis. In a meta-analysis of randomized, controlled trials that compared a pressure preset or volume preset NIV with no NIV in cystic fibrosis patients with respiratory failure, the authors found that airway clearance may be easier with NIV and that patients with CF may have a preference for it. They concluded that NIV may be a useful adjunctive therapy to other airway-clearance approaches. In addition, in patients with moderate to severe disease, NIV used along with oxygen may improve gas exchange, as compared with oxygen therapy alone, while such patients are sleeping. [62]
Radiography
Chest radiographs may be normal in patients with cystic fibrosis who have mild lung disease.
Hyperinflation is the earliest discernible change, which is initially reversible with treatment but which later becomes persistent. Hyperinflation is caused by mucus plugging of small bronchioles. It may be the sole manifestation of the disease in childhood, but in some milder cases, it is the only radiologic finding even in adults. Hyperinflation is readily identified through the classic sign of flattening of the diaphragm, anterior bowing of the infant sternum, increased retrosternal air space, and generalized pulmonary overinflation. Air trapping in the older patient may not be recognizable on plain images, but it is readily identified by using HRCT performed in the expiratory phase. [63]
(See the radiographic images below of cystic fibrosis.)
Cystic fibrosis, thoracic. Young man with a history of cystic fibrosis has hyperinflation and predominantly upper lobe bronchiectasis.
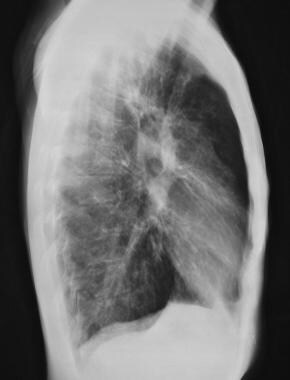 Cystic fibrosis, thoracic. Lateral chest radiograph shows flattened hemidiaphragms, increased retrosternal clear space (overaeration).
Cystic fibrosis, thoracic. Lateral chest radiograph shows flattened hemidiaphragms, increased retrosternal clear space (overaeration).
 Cystic fibrosis, thoracic. Patient with history of cystic fibrosis has bilateral bronchiectasis, most pronounced in the upper lobes along with left upper lung atelectasis.
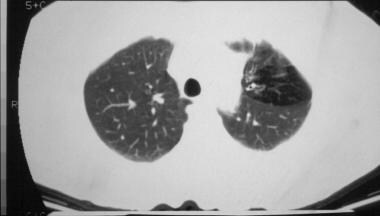
Cystic fibrosis, thoracic. Patient with a history of cystic fibrosis has complete right lung atelectasis with extreme bronchiectasis. Marked hyperinflation of the left lung is noted.
Cystic fibrosis, thoracic. Patient with history of cystic fibrosis has bilateral bronchiectasis, most pronounced in the upper lobes along with left upper lung atelectasis.
Cystic fibrosis, thoracic. Patient with a history of cystic fibrosis has complete right lung atelectasis with extreme bronchiectasis. Marked hyperinflation of the left lung is noted.
 Cystic fibrosis, thoracic. Image in a 27-year-old tennis player with a history of cystic fibrosis and only minimal symptoms exhibits bronchial wall thickening, bilateral small nodular opacities, and scoliosis.
Cystic fibrosis, thoracic. Image in a 27-year-old tennis player with a history of cystic fibrosis and only minimal symptoms exhibits bronchial wall thickening, bilateral small nodular opacities, and scoliosis.
Bronchial cuffing and/or bronchial-wall thickening are very frequent findings. This is caused by infiltration of submucosa by acute and chronic inflammatory cells.
Findings in moderate or advanced disease
Linear streaking and scattered nodules (nodular or reticular nodular appearance) result from the obstruction of small airways by mucus. Mucoid impaction of the bronchi appears as areas of increased opacity that follow the course of dilated bronchi.
Atelectasis may be observed. Segmental, patchy, or lobular atelectasis results from mucus plugging. This complication is more common in children than in adults. In children (not adults), it is associated with a worse prognosis. A characteristic location is in the right upper lobe.
Bronchiectasis is characterized by parallel, thick, line markings radiating from hila (line tracks) in cylindrical bronchiectasis. Ring shadows represent dilated thick-wall bronchi seen in longitudinal section or on-end or dilated bronchi in varicose bronchiectasis. Also seen are clusters of cysts in cystic bronchiectasis and air-fluid levels within cysts representing airway suppuration. These radiographic changes are most common in the upper lobes and are partly related to the effects of gravity and hyperinflation. [64, 65] Thin-walled cysts in the upper lobes may appear to extend to the lung surface. Some of the cysts represent emphysematous or interstitial air cysts.
Multiple nodular densities represent mucus plugging and occasionally appear with a finger-in-glove shape or as a combination of V- or Y-shaped branching and bandlike shadows.
Consolidative pneumonia is rare despite persistent bacterial infection. Even with acute clinical exacerbation of disease, chest radiographic findings may not change.
Pleural effusions are not common in CF despite chronic infection. Pleural thickening is better appreciated on CT scans than on other images.
Pneumothorax may be seen.
Hilar enlargement can result from either hilar lymphadenopathy, which is commonly seen as reaction to chronic infection in CF or from enlarged pulmonary arteries. [66] The heart generally appears small because of hyperinflation. An acute increase in the size of the heart from severe cor pulmonale exacerbation is an ominous, often life-threatening, sign.
Scoring systems
Multiple scoring systems can be used to categorize the chest radiographic findings in CF and to assess the severity of disease. [67, 68, 69] Although these systems are useful in assessing epidemiology [70] and natural history, they have not been proven helpful in defining acute clinical exacerbations. The systems are reproducible, and the grades are correlated with the results of PFTs.
In the US, a commonly used system is the Brasfield system, which is also called the Birmingham system. [68]
The systems are used to assess 5 elements, including the following:
-
Airtrapping
-
Linear markings
-
Nodular cystic lesions
-
General severity
-
Large lesions (eg, atelectasis or consolidation)
The first 4 elements are scored 0-4, where 0 is used if the finding is not present, and 4 is used if the finding is severe. The points are totaled then subtracted from 25. A normal chest radiographic finding receives a score of 25. The minimum score for the most severe changes in CF is 3.
Abdominal findings
Dilated multiple loops of the small bowel are seen in neonatal meconium ileus and in meconium ileus–equivalent condition, or distal intestinal obstruction syndrome (DIOS), in older individuals. In neonatal meconium ileus, air-fluid levels are usually absent on horizontal beam views because of the tenacious character of the meconium. Instead, a bubbly appearance can often be noted upon a background of distal bowel obstruction and an absence of rectal air.
Contrast enema examination shows filling defects in the ileocecal region in both entities. The absence of reflux into the terminal ileum also may suggest DIOS in the older person. In neonates, a microcolon of disuse is initially seen, and reflux back across the ileocecal valve finds a string of meconium pellets leading to a long snakelike obstructing ileal filling defect of gelatinous meconium. An attempt is usually made to reflux a water-soluble contrast material proximally into the dilated loops of the ileum to cleanse the bowel of the obstructing meconium. Wetting agents in the contrast agent and the relatively hypertonic fluid may play a role in disimpaction. Serial enema studies over several days may be needed for successful resolution of the meconium ileus.
Colonic mucosa may also appear hyperplastic and redundant, especially in evaluation after a contrast enema. This finding is known as jejunization of the colon and, on plain films, may mimic fecal retention despite a relatively empty colon. Pneumatosis coli has also been reported and, typically, patients with this condition are asymptomatic.
Contrast enema findings in fibrosing colonopathy include nodularity of the colonic wall, focal or long-segment narrowing, and longitudinal shortening of the colon.
Intussusception can be seen in older children. A tenacious stool in the distal ileum usually is present as the lead point, and dilated fluid-filled small bowel loops are likely to be seen. Contrast or air enemas performed in the setting of intussusception are diagnostic and may be therapeutic.
Within the neonatal abdominal cavity or the scrotum, calcifications are evidence of meconium peritonitis resulting from an in utero perforation. Twisted bowel loops associated with acquired atresia and necrosis of bowel may become matted and appear as a mass or pseudocyst. Pancreatic calcifications can be seen.
Duodenal abnormalities are seen in 80% of patients with cystic fibrosis and are most prominent in the first and second parts of the duodenum. Findings include thickening of the mucosal folds, nodular indentations, smudging or poor definition of the mucosal-fold pattern, and redundant and distorted duodenal loops. Remaining small-bowel involvement is less common and primarily involves thickened folds in the proximal jejunum and, occasionally, jejunal dilatation.
Sinus findings
Maldevelopment of the sinuses and pansinus opacification on the radiograph are common findings. Occasionally a mucocele results from osteal obstruction.
Skeletal findings
Hypertrophic osteoarthropathy (HBOA) is characterized by periosteal new bone formation. Periostitis is seen in the diaphyses of the tubular bones, and it may involve single or multiple layers or a solid cloaking of the bone. Osteopenia may also be found.
Kyphosis is found in 8.7% of patients, as assessed with chest radiographs. Compared with younger persons, patients older than 20 years have a greater degree of kyphosis, which is associated with worsening lung disease. Bone deformities are important in the development of kyphosis and vertebral fractures. Wedging is seen on chest radiographs in 74% of patients with CF, and 15% of wedges are greater than 20%, which is the usual definition for a vertebral compression fracture. Osteoporosis may play a role in the development of these abnormalities. [71]
False positives/negatives
Hyperinflation and peribronchial cuffing may be confused with asthma or bronchiolitis due to other pulmonary infections, particularly measles, pertussis, adenoviral infection, or obliterative bronchiolitis. Linear streaking and scattered nodules may be present in granulomatoses, fungal disease, or sarcoid. Air-fluid levels in large cystic bronchiectasis can be confused with lung abscess. Normal chest radiographic findings cannot completely exclude the presence of bronchiectasis. In one study, 7.1% of chest radiographs were normal in patients with proven CF.
Computed Tomography
Several authors have proposed grading systems by using high-resolution CT (HRCT) findings. The most popular scoring system is the Bhalla system. [72, 31, 32] This is a 25-point merit system, and the scores can be interchanged with a Brasfield score in clinical classification systems. The presence, extent, and severity of bronchiectasis, peribronchial thickening, mucous plugging, atelectasis or consolidation, and emphysema are recorded. Despite the replacement of the nonspecific descriptors of the Brasfield system with a more accurately defined and quantified morphologic HRCT system, whether this new system will have practical use in the assessment of patients and therapeutic interventions is unclear. [17, 20]
Air trapping
Air trapping is readily identified on HRCT scans obtained in the expiratory phase. Affected areas appear more lucent, and the change in attenuation is less than the attenuation in the normal lung. On expiratory HRCT scans, air trapping in the absence of inspiratory scan abnormalities could be the earliest sign of small-airway disease. This has been proven for bronchiolitis obliterans and asthma; patients with cystic fibrosis usually have some abnormalities on the inspiratory HRCT scans. Emphysematous bullae and subpleural blebs frequently develop. Overinflation is found in approximately 81% of patients.
(See the image below.)
 Cystic fibrosis, thoracic. Focal overaeration in the left upper lobe of a patient with cystic fibrosis. Thick-walled bronchi in the affected area are seen. The focal overaeration probably indicates air-trapping and bronchiolitis obliterans.
Cystic fibrosis, thoracic. Focal overaeration in the left upper lobe of a patient with cystic fibrosis. Thick-walled bronchi in the affected area are seen. The focal overaeration probably indicates air-trapping and bronchiolitis obliterans.
Mosaic perfusion
Mosaic perfusion is the second sign of small-airway abnormalities on HRCT scans and is seen in approximately 64% of patients. Geographic areas of decreased perfusion present in areas that hypoventilated and appear as patches of relatively low attenuation that alternate with more-normal lung. Expiratory HRCT may be necessary to differentiate among different causes of mosaic patterns of lung attenuation.
Minimal intensity projection images of thin-section scans help in demonstrating a mosaic pattern of lung attenuation caused by small-airway disease. In healthy persons, as much as 25% of the cross-sectional area of 1 section of lung can demonstrate airtrapping, whereas this rate can increase to 60-70% in patients with CF.
In patients with suspected small-airway disease, a 5-mm-thick minimal intensity projection image is advantageous because patients with dyspnea can perform a 5-second breath hold easier than a 10-second breath hold. Also, the use of 5-mm-thick minimal intensity projections reduces the radiation dose, as compared to the dose needed for 10-mm minimal intensity projections. [73]
Bronchial wall thickening
CT scanning allows visualization of the airways in the periphery beyond the level of segmental bronchi. Bronchial wall thickening is seen in approximately 48-76% of patients.
(See the images below.)
 Cystic fibrosis, thoracic. Coned-down views of each upper lobe in a 26-year-old mother of 2 children with history of cystic fibrosis and mild symptoms demonstrates nodular opacities, which presumably represent ectatic bronchi and mucus plugging.
Cystic fibrosis, thoracic. Coned-down views of each upper lobe in a 26-year-old mother of 2 children with history of cystic fibrosis and mild symptoms demonstrates nodular opacities, which presumably represent ectatic bronchi and mucus plugging.
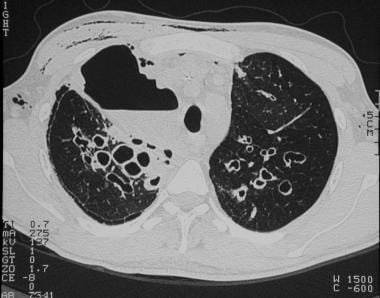
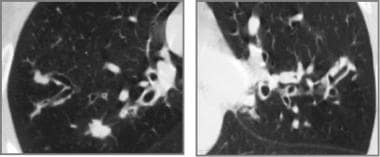 Cystic fibrosis, thoracic. High-resolution CT scan of each upper lobe in the same patient as in the previous image confirms thick bronchial walls, bronchiectasis, and inspissated mucus in ectatic bronchi.
Cystic fibrosis, thoracic. High-resolution CT scan of each upper lobe in the same patient as in the previous image confirms thick bronchial walls, bronchiectasis, and inspissated mucus in ectatic bronchi.
Bronchiectasis
Bronchiectasis is the most common individual CT abnormality and is seen in approximately 80% of patients. Three forms of bronchiectasis may also be visualized, as in other causes of bronchiectasis: cylindrical, varicose, and cystic or saccular.
Cylindrical bronchiectasis is the most common pattern in CF. Bronchi retain their regular outline but are mildly dilated and fail to taper. Instead, they terminate abruptly with square ends. The most distal bronchi and bronchioles are plugged with secretions, but pathologically, the number of bronchial subdivisions is normal. Mucous plugging is seen in approximately 30-51% of patients.
Signs of bronchiectasis include the tubular shadows; tram tracks (see the image below), or horizontally oriented bronchi; and the signet-ring sign, which is a vertically oriented bronchus with a luminal airway diameter that is 1.5 times the diameter of the adjacent pulmonary arterial branch.
Cystic fibrosis, thoracic. High-resolution CT image shows bronchial wall thickening (tram lines), predominantly in the upper lobes.
Varicose bronchiectasis is marked by a greater degree of dilation combined with local ballooning of the airway. Bronchi have an irregular outline, and the number of patent airway divisions is reduced from the normal number, which is as many as 20, to about 6 or 7. Varicose bronchiectasis can appear as a string of pearls (a horizontally oriented bronchus) (see the image below).
Cystic fibrosis, thoracic. String-of-pearls sign in the left lower lobe in a patient with cystic fibrosis. The soft tissue surrounding each "pearl" indicates focal atelectatic, fibrotic lung.
Cystic or saccular bronchiectasis is seen as the disease progresses. This condition may include bronchial dilation over the lung periphery, and dilation of only 4-5 generations can appear as a cluster of cysts (especially with atelectasis) or with a honeycomb appearance. These cystic changes are in contrast to the blebs of emphysema, which are thinner walled and not accompanied by proximal airway abnormalities.
Some of the cysts may contain fluid, which indicates airway suppuration. In adults with CF, air-fluid levels in bronchiectatic cavities are the only parenchymal findings shown on HRCT scans. [74] This is limited to the acute exacerbation of CF; however this finding is fairly rare. Mucous plugging, centrilobular nodules, and peribronchial thickening are also potentially reversible findings in symptomatic patients.
In adults with newly diagnosed CF, bronchiectasis is predominantly central and also seen peripherally, with the most-severe bronchial dilatation in the upper lobes. A nodular or reticular-nodular pattern is characterized by a cluster of ill-defined nodules corresponding to the branching terminal airways filled with secretions. A centrilobular nodule or a tree-in-bud appearance can occur. A ground-glass pattern (see the image below) is a nonspecific sign of pneumonitis and/or bleeding. Parenchymal abnormalities are recognized in approximately 58% of patients; alveolar consolidation is more common than destructive changes. Hilar enlargement due to adenopathy or pulmonary hypertension may occur.
 Cystic fibrosis, thoracic. CT image shows a peribronchial ground glass opacity and hyperinflation in a patient with cystic fibrosis during an acute febrile illness, which responded to antibiotics. This pattern is an example of acute pneumonia.
Cystic fibrosis, thoracic. CT image shows a peribronchial ground glass opacity and hyperinflation in a patient with cystic fibrosis during an acute febrile illness, which responded to antibiotics. This pattern is an example of acute pneumonia.
Overall, the severity and profusion of bronchial lesions and parenchymal destructive changes are unevenly distributed among the different regions, the upper parts of the lungs being more heavily involved than the lower parts, particularly on the right.
Previous investigators concluded that the HRCT pattern and distribution of abnormalities seen in patients with bronchiectasis are influenced by the underlying cause. Bilateral bronchiectasis that predominantly affects the upper lobes is most common in patients with CF and allergic bronchopulmonary aspergillosis (ABPA). Central bronchiectasis is a characteristic but not sensitive CT finding in patients with ABPA. Because ABPA can complicate the course of CF in about 10-15% of patients, differentiating these 2 diseases may be difficult with HRCT.
Generally, CF causes bilateral symmetric involvement, whereas ABPA is most commonly associated with bilateral and asymmetric involvement. Although a predilection for the middle lobe has been reported in the immotile cilia syndrome and in hypogammaglobulinemia, this finding alone is not sufficiently characteristic to differentiate these 2 diseases from CF. A unilateral upper-lobe predominance suggests tuberculosis, whereas a lower-lobe predominance suggests bronchiectasis after a childhood viral infection. Most importantly, the HRCT findings must be interpreted in the clinical context.
A multicenter trial by Lynch et al included 261 patients with symptomatic and physiologically significant bronchiectasis. [75] The study showed that the degree of morphologic abnormalities on CT scans and the extent of physiologic impairment are weakly but significantly correlated. In a study of patients with CF, Helbich et al showed that serial CT scans allowed the assessment of the evolution of pulmonary abnormalities in a more sensitive way, as compared to pulmonary function tests (PFTs) and clinical scoring, with a window of 6-18 months. [76] However, the clinical effectiveness of CT in the follow-up of patients with CF has not been confirmed.
(See the additional images below displaying bronchiectasis on CT scanning.)
 Cystic fibrosis, thoracic. High-resolution CT scan shows moderately extensive bronchiectasis at the level of the upper lobes.
Cystic fibrosis, thoracic. High-resolution CT scan shows moderately extensive bronchiectasis at the level of the upper lobes.
 Cystic fibrosis, thoracic. Bronchiectatic changes with segmental right middle lobe and left lower lobe atelectasis in a patient with cystic fibrosis.
Cystic fibrosis, thoracic. Bronchiectatic changes with segmental right middle lobe and left lower lobe atelectasis in a patient with cystic fibrosis.
 Cystic fibrosis, thoracic. High-resolution CT image in a patient with a history of cystic fibrosis and acute chest pain shows cystic and cylindrical bronchiectasis, as well as a large air space with an air-fluid level in the right upper lobe and subcutaneous emphysema. Extrapulmonary air, including pneumothorax, is a common complication in the presence of large air pockets (cysts).
Cystic fibrosis, thoracic. High-resolution CT image in a patient with a history of cystic fibrosis and acute chest pain shows cystic and cylindrical bronchiectasis, as well as a large air space with an air-fluid level in the right upper lobe and subcutaneous emphysema. Extrapulmonary air, including pneumothorax, is a common complication in the presence of large air pockets (cysts).
Pancreatic abnormalities
In the advanced stages of CF, the exocrine tissues of the pancreas are often completely replaced by fat. On CT scans, the pancreas is composed purely of fat, which is isoattenuating relative to the adjacent retroperitoneal fat. (This finding is in contrast to the fatty replacement in aged and obese individuals in whom a recognizable pancreatic parenchyma is present.)
Pancreatic fat replacement is the most common pattern in older patients with CF and is correlated with pancreatic exocrine dysfunction. The pancreas may become hypertrophied, or it may appear smaller than normal, although the shape of the pancreas is maintained. Other less-common CT findings in advanced CF include pancreatic cysts or calcifications, atrophy of the normal pancreatic tissue with less degrees of fatty replacement, and marked atrophy without fatty replacement. When cysts are present, they are typically 1-3 mm and rarely larger than 1 cm. Pancreatic cystosis occurs rarely. Despite the relatively common presence of pancreatic calcification, clinical pancreatitis in patients with CF is less common.
Hepatobiliary abnormalities
Images may show fatty infiltration of the liver or findings of liver cirrhosis. Gallbladder abnormalities are described elsewhere.
Colonic disease
Pickhardt et al performed a retrospective review of 26 patients with CF who underwent abdominal CT, mostly for the assessment of abdominal pain. [77] They identified colonic abnormalities in 10 patients. Proximal thickening of the colon wall (mean thickness, 6.4 mm) without stricture was identified in all patients. Mural striation was found in 50% of patients. Pericolonic mesenteric fatty proliferation with involvement of the ascending colon was found in 60%. Soft tissue infiltration of the paracolonic fat was identified in all patients. No association was found between enzyme replacement therapy and colonic wall thickening. The sigmoid and ascending colon was involved in all patients with decreasing frequency of involvement of the transverse and descending colon. No skip lesions were seen in the small bowel or large bowel.
Meconium ileus
CT findings of meconium ileus include diffuse colonic thickening and no paracolonic changes. The frequency of Crohn disease has been reported to be increased in children and adults with CF. However, in many cases, the diagnosis is based on radiologic findings without histopathologic proof. Increased wall thickness, mural striation, and fatty mesenteric proliferation are associated with both diseases.
Generally, the mean wall thickness in Crohn colitis is about 11 mm, which is thicker than that observed in patients with CF. Small-bowel involvement is also more common (60%) in Crohn disease, in contrast with CF. Colonic involvement in Crohn disease may be right, left sided, or bilateral, whereas in CF, colonic disease is usually right sided, with a variable distal extent. Colonic involvement in CF lacks also other specific findings of Crohn disease such as sinus tracts, fistulas, and abscesses.
Other possible causes of colonic wall thickening in patients with CF include edema, lymphedema, and chronic inflammation.
Paranasal sinuses
Previous studies have shown 2 patterns of sinus disease in patients with CF: chronic sinusitis (headaches being the major complaint) and polyposis (patients have mostly nasal obstruction).
In a study of 116 patients with CF who were grouped according to the number of confirmed mutations, Eggesbo et al found that patients with genetically verified CF had less-developed sinuses, they lacked pneumatization variance, and they more commonly had anatomic variants that predisposed them to complications during function endoscopic sinus surgery. [14] The same group reported that hypoplasia of the sphenoid sinuses is a characteristic finding in patients with CF. They suggested that if pneumatization of the bases of sphenoid is present, the existing CF diagnosis should be questioned.
Overall, CT scans of CF patients are generally characterized by uncinate process demineralization, frequent frontal sinus agenesis, maxilloethmoid sinus opacification, and medial displacement of the lateral nasal wall in the middle meatus. Interestingly, the size of maxillary sinuses increases with advancing age in control subjects and in patients with chronic sinusitis, but not in patients with CF.
The main strength of CT of the sinuses in patients with CF is its ability to clarify the extent and localization of disease. This information can direct the surgeon to specific areas. Some studies emphasize that CT offers a more-precise evaluation of the extent of disease than nasal endoscopy. In other studies, however, nasal sinus endoscopy offered additional information when compared to CT, because CT cannot be used to differentiate mucosal thickening and infectious material.
On CT scans, all the soft tissue masses appear homogeneous both before and after the injection of contrast material. Contrast enhancement of the soft tissue masses has not been demonstrated in previous studies, even if this phenomenon is said to be an indication of infection, including that caused by recurrent sinusitis and pyomucocele. Therefore, the diagnosis of an infectious process in the paranasal sinuses (eg, pyocele) may be difficult if CT secondary changes (eg, expansion or erosion of the bone) are lacking. An air-fluid level is not common during CT imaging of the paranasal sinuses in patients with CF.
False positives/negatives
Except for the previously mentioned causes of bronchiectasis that can mimic the HRCT manifestations of CF, interstitial diseases with fibrosis and traction bronchiectasis can create a similar honeycomb picture.
Inadequate collimation and motion artifacts are common pitfalls. Differentiating between cylindrical bronchiectasis and reversible bronchial dilation after pneumonia or atelectasis (ie, reversible or pseudobronchiectasis) is different. Mucoid impaction is seen as a tubular opacity and is occasionally confused with vessels.
Emphysematous cysts with peribronchial inflammation, which may be seen in the course of severe chronic obstructive pulmonary disease (COPD), can also cause cystic spaces and may present similar CT findings; their age distributions are different, however.
Magnetic Resonance Imaging
Initial reports suggested that MRI could be useful in the assessment of cystic fibrosis because of its ability to depict early mucus plugs and differentiate mucoid impaction from atelectasis or shadows caused by flowing blood. Subsequent studies showed that chest radiography is superior to MRI in assessing air-containing structures and hyperinflation. MRI can also be used to differentiate between hilar enlargement due to large nodes and enlargement due to large pulmonary arteries.
Techniques in functional ventilation imaging include the use of inhaled aerosols, oxygen, and hyperpolarized noble gases (helium-3, xenon-129, fluorinated gases). [78] Images demonstrating homogeneity of ventilation and those helpful in determining ventilated lung volumes can be obtained. Furthermore, image-derived functional parameters such as airspace size, regional oxygen partial pressure, ventilation distributions, and ventilation/perfusion ratios can be measured.
The MRI technique applied to patients with airway diseases, such as patients with CF, may yield better sensitivity in the detection of ventilation defects when findings from ventilation scintigraphy, chest CT or standard PFTs are not helpful. [19, 20]
Magnetic resonance cholangiography
Magnetic resonance cholangiopancreatography (MRCP) has also been reported to be a useful technique in the study of hepatobiliary disease in CF. MRCP depicts anomalies in all CF patients with the diagnosis of liver disease and reveals ductal lesions not revealed with other noninvasive techniques.
Perez-Aguilar et al found the following conditions in 10 of 15 adult patients with CF and no other liver disease: beaded contour of the hepatic ducts or common bile duct; stenosis of the common hepatic duct with rigidity of the intrahepatic ducts and irregularities in the caliber of the intrahepatic ducts without dilatation; and/or suspicious findings of intrahepatic lithiasis. [79]
Especially because it is noninvasive, this technique can be useful in differentiating primary sclerosing cholangitis from bile duct involvement due to CF.
MRI of the paranasal sinuses
MRI is superior to CT in differentiating soft tissue masses in the paranasal sinuses in patients with CF. These masses in the paranasal sinuses and middle meatus demonstrate heterogeneous signal intensity with all sequences. Contrast-enhanced T1-weighted images show contrast enhancement of the thickened mucosa in the sinuses and soft tissue masses; however, short-tau inversion recovery (STIR) images are superior in differentiating mucosal thickening from other material. Pseudomonas aeruginosa is frequently cultured from the areas with signal void on the STIR images; this signal void is known as the black-hole sign.
One study included 62 patients with CF and ethmomaxillary sinus disease (as seen at CT) who underwent MRI of the paranasal sinuses. In these patients, 3 major types of maxillary sinuses were distinguished: an air-filled sinus lumen, an oval-shaped pus-filled sinus lumen, and streaky-shaped pus-filled sinus lumen. For air-filled maxillary sinuses with mucosal thickening, CT and MR imaging were diagnostically equivalent. When CT showed homogeneous opacification of the maxillary sinuses, MRI findings differentiated thickening mucosa and pus-filled areas. Patients who had undergone functional endoscopic sinus surgery (FESS) most commonly had an air-filled or streaky-shaped pus-filled maxillary sinus lumen. In patients who did not undergo surgery, an oval-shaped pus-filled sinus lumen was most common and could occur without ethmoid disease. [15]
Because MRI of the paranasal sinuses can be used to differentiate infectious material and thickening mucosa, it could be used to select patients in whom pus-filled areas might be eradicated with FESS.
Ultrasonography
Dietrich et al have reported the use of high-resolution mediastinal ultrasonography in assessing the total lymph node volume in the paratracheal region and in using the aortopulmonary window as a marker of inflammatory disease activity in cystic fibrosis patients. [80, 18]
Pancreatic abnormalities
The pancreas is usually echogenic as a result of fatty replacement and fibrosis of the exocrine portion of the gland. It is typically smaller than normal; however, at times, it may be enlarged. Ductal ectasia, cysts, or multiple foci of calcification may also be seen.
Hepatobiliary abnormalities
Fatty infiltration of the liver is commonly seen, and gallbladder abnormalities are found during ultrasonographic examination of approximately one third of patients with CF. A microgallbladder may be seen; this is caused by atresia or obstruction of the cystic duct resulting from mucosal hyperplasia or inspissated mucous.
Cholelithiasis, choledocholithiasis, thickening of the gallbladder wall, and gallbladder sludge may be found, singly or in combination. Abnormalities of the intrahepatic biliary tree, which resemble those of sclerosing cholangitis, may also be seen in patients with CF-related liver disease. Occasionally, abdominal ultrasonography helps in the diagnosis of appendicular mucocele. [81]
Doppler echocardiography
Doppler echocardiography imaging has been used in the assessment of severe CF. This technique can show common subclinical right ventricular dysfunction, which is correlated with the severity of lung disease, with impairment of both systolic and diastolic right ventricular functions. In one study, no specific left ventricular function abnormalities were detected. [82] Two-dimensional echo Doppler imaging is also useful in the preoperative assessment of patients who are candidates for lung transplantation. [83, 84]
Prenatal ultrasonography
Prenatal ultrasonographic findings include a hyperechoic fetal bowel pattern with an echogenicity similar to or greater than that of the fetal bone. This finding is suggestive of intestinal obstruction. It can appear as a benign variant, usually before the third trimester, followed in that case by spontaneous resolution. CF has been detected in 5% of cases with fetal hyperechogenic bowel. [85] The differential diagnosis also includes Down syndrome and other chromosomal abnormalities, influenza infection, and amniotic fluid in the blood.
Nuclear Imaging
The role of lung scintigraphy in patients with cystic fibrosis is not clear. A normal chest image and a normal technetium-99m perfusion scan essentially rule out bronchiectasis. In children with recurrent respiratory problems, lung scintigraphy frequently shows regional abnormalities, even in the absence of radiologic signs. The main problem is the correct clinical use of a test with such a high sensitivity and the high percentage of false-positive results.
In patients with CF, nuclear scanning has been reported to be a useful diagnostic modality in infants with prolonged jaundice, in those unresponsive to choleretics, and in those with known dilated bile ducts in the gallbladder (as shown on ultrasonograms). In a study by Greenholz et al, the absence of biliary excretion on nuclear scans was used to identify neonates with microscopically normal bile ducts but an inspissated bile syndrome produced by cholestasis secondary to plugging. [86] In such neonates, surgical exploration is warranted. Technetium-99m mebrofenin scintigraphy of the liver has also been used successfully in CF patients to rule out hepatobiliary disease. [87]
Other applications include dual-energy x-ray absorptiometry as a tool of determining bone mineral density (BMD). Elkin et al examined 107 patients with CF by using dual-energy x-ray absorptiometry of the lumbar spine and hip, as well as radiology of the spine and biochemical studies. [71] The study was performed to determine the prevalence of low BMD and vertebral deformities in adults with CF. They found that 38% had a Z score of less than -1, with 13% having Z scores of less than -2. Of the patients, 17% had evidence of a vertebral deformity on radiographs; the deformities were mostly in the thoracic spine. In addition, 35% reported past fractures. The investigators found that the number of courses of intravenous antibiotics that the patients received in the previous 5 years was negatively related to BMD. They concluded that fragility fractures are common in adults with CF.
Low BMD occurs in patients with more-severe disease and is significantly related to FEV1, infective exacerbations, and the daily energy expended in physical activity. Total BMD is also decreased in prepubertal children with mild lung disease and bears no relationship to the degree of lung disease, the degree of fat malabsorption, the level of physical activity, and the dietary energy intake.
The short and narrow bones are the main reasons for reduced BMD and for a reduced bone mineral content in patients younger than 19 years. This finding indicates that the treatment to prevent osteoporosis in younger patients should be directed at increasing bone size, whereas conventional treatment with calcium and vitamin D supplementation might not be as effective. The significant decrease in BMD and bone mineral content (BMC) in young adult patients raises the concern that these patients will develop premature osteoporotic fractures.
In a study by Cremaschi et al, the effects of bronchial artery embolization (BAE) were reviewed in a group of 209 patients, 16% of whom had CF. [88] They reported that all of the cases of hemoptysis were controlled in the first 48 hours; 16% of the relapses occurred within the first year. These authors underline the value of selective digital angiography in reducing the catheterization time, the mean quantity of contrast material administered, and the number of adverse effects.
-
Cystic fibrosis, thoracic. Young man with a history of cystic fibrosis has hyperinflation and predominantly upper lobe bronchiectasis.
-
Cystic fibrosis, thoracic. Lateral chest radiograph shows flattened hemidiaphragms, increased retrosternal clear space (overaeration).
-
Cystic fibrosis, thoracic. Patient with history of cystic fibrosis has bilateral bronchiectasis, most pronounced in the upper lobes along with left upper lung atelectasis.
-
Cystic fibrosis, thoracic. Patient with a history of cystic fibrosis has complete right lung atelectasis with extreme bronchiectasis. Marked hyperinflation of the left lung is noted.
-
Cystic fibrosis, thoracic. Image in a 27-year-old tennis player with a history of cystic fibrosis and only minimal symptoms exhibits bronchial wall thickening, bilateral small nodular opacities, and scoliosis.
-
Cystic fibrosis, thoracic. High-resolution CT scan shows moderately extensive bronchiectasis at the level of the upper lobes.
-
Cystic fibrosis, thoracic. Coned-down views of each upper lobe in a 26-year-old mother of 2 children with history of cystic fibrosis and mild symptoms demonstrates nodular opacities, which presumably represent ectatic bronchi and mucus plugging.
-
Cystic fibrosis, thoracic. High-resolution CT scan of each upper lobe in the same patient as in the previous image confirms thick bronchial walls, bronchiectasis, and inspissated mucus in ectatic bronchi.
-
Cystic fibrosis, thoracic. Erect abdominal radiograph shows multiple, small intestinal fluid levels in association with localized bubbly fecal material in the right lower quadrant. These were due to distal intestinal obstruction syndrome in a patient with cystic fibrosis.
-
Cystic fibrosis, thoracic. High-resolution CT image shows bronchial wall thickening (tram lines), predominantly in the upper lobes.
-
Cystic fibrosis, thoracic. Focal overaeration in the left upper lobe of a patient with cystic fibrosis. Thick-walled bronchi in the affected area are seen. The focal overaeration probably indicates air-trapping and bronchiolitis obliterans.
-
Cystic fibrosis, thoracic. Bronchiectatic changes with segmental right middle lobe and left lower lobe atelectasis in a patient with cystic fibrosis.
-
Cystic fibrosis, thoracic. String-of-pearls sign in the left lower lobe in a patient with cystic fibrosis. The soft tissue surrounding each "pearl" indicates focal atelectatic, fibrotic lung.
-
Cystic fibrosis, thoracic. Dilated bronchi with thickened wall are depicted bilaterally. Mucoid impaction is the cause of the soft tissue density within the ectatic bronchi in the left lower lobe.
-
Cystic fibrosis, thoracic. In this patient with cystic fibrosis, bronchiolar mucous plugging is noted in the left upper lobe.
-
Cystic fibrosis, thoracic. CT image shows a peribronchial ground glass opacity and hyperinflation in a patient with cystic fibrosis during an acute febrile illness, which responded to antibiotics. This pattern is an example of acute pneumonia.
-
Cystic fibrosis, thoracic. High-resolution CT image in a patient with a history of cystic fibrosis and acute chest pain shows cystic and cylindrical bronchiectasis, as well as a large air space with an air-fluid level in the right upper lobe and subcutaneous emphysema. Extrapulmonary air, including pneumothorax, is a common complication in the presence of large air pockets (cysts).