Practice Essentials
Cryptorchidism is defined as failure of the testis to descend from its intra-abdominal location into the scrotum. About 3% of full-term and 30% of premature male infants are born with one or both testicles undescended, but approximately 80% of cryptorchid testes will descend by the third month of life. The undescended testicle can usually be palpated in the inguinal canal, but in a minority of cases, it may be located in the abdomen or may be nonexistent. [1, 2, 3]
The exact etiology of cryptorchidism is not known. In one third of patients, the condition is bilateral. If the testis does not descend by 6 months of age, surgical correction should be considered. Infertility will occur in up to 10% of patients with a unilateral undescended testis. If orchiopexy is done before puberty, the risk of testicular cancer is about 3 times that of the general population, but it is 5 to 6 times higher if performed after puberty. [1, 2, 3]
According to the Canadian Urological Association-Pediatric Urologists of Canada (CUA-PUC), imaging for cryptorchidism is not cost-effective and may delay referral and surgical treatment; however, imaging may help direct the best initial approach, such as scrotal, inguinal, or laparoscopic. Physical examination is the cornerstone of cryptorchidism evaluation, with more than 70% of cryptorchid testes being palpable. If the testicle is not palpable on preoperative physical evaluation, examination under anesthesia should be conducted at the beginning of surgical exploration. [1, 2, 3]
Orchiopexy is the treatment of choice and usually is performed in patients aged 2-10 years. A cryptorchid testis, shown in the image below, is 20-48 times more likely to undergo malignant degeneration than a normal testis. Orchiopexy does not alter the risk of malignant transformation. The incidence of malignant transformation also is increased in the unaffected testis. Consider hormone treatment with either human chorionic gonadotropin or gonadotropin-releasing hormone analogues for palpable high-scrotal position of the testis; however, efficacy is less than 20%. Surgical treatment is most effective and reliable. [4, 5, 6]
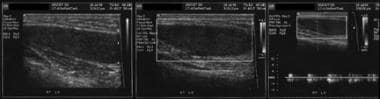 Longitudinal sonogram of the right cryptorchid testis at the level of the inguinal canal. Intratesticular spectral Doppler waveform demonstrates normal low-resistance pattern of flow.
Longitudinal sonogram of the right cryptorchid testis at the level of the inguinal canal. Intratesticular spectral Doppler waveform demonstrates normal low-resistance pattern of flow.
No radiologic intervention exists. [7, 8] Ultrasonography is the first imaging modality performed on a cryptorchid testis. Of cryptorchid testes, 72% are in the inguinal canal. [9] The American Urological Association (AUA) recommends that a scrotal ultrasound not be performed in the preoperative management of cryptorchidism. The sensitivity and specificity of ultrasound to localize nonpalpable testes have been estimated to be 45% and 78%, respectively. Surgical intervention for cryptorchidism should be completed by 12 to 18 months of age; however, successful scrotal repositioning of the testis may reduce but not prevent infertility and testicular cancer. [10, 11, 12]
In a study of 58 patients in whom one or both testes were not palpable preoperatively or under general anesthesia, the addition of US to clinical examination increased the sensitivity to correctly predict an inguinal incision from 29% to 71% and increased specificity slightly from 88% to 92%. [13]
If US cannot identify the testis (US effectively detects cryptorchid testis below the level of the internal inguinal ring), MRI and CT scanning are the subsequent modalities of choice. Both can detect an abdominal testis. [14, 15] Laparoscopy is performed if MRI and CT cannot localize the testis, [16] but it is invasive and expensive.
US cannot detect an intra-abdominal testis, and CT scanning uses radiation and does not have multiplanar capability. MRI has better soft-tissue contrast and multiplanar capability; however, when the testis is higher in the abdomen, the presence of bowel loops lowers the sensitivity for detecting the cryptorchid testis.
Computed Tomography
Cryptorchid testis is seen as an oval soft-tissue mass along the expected course of testicular descent. Uniform enhancement is seen with intravenous (IV) radiographic contrast. CT is almost as accurate as US in detecting an undescended testis in the inguinal region. CT and MRI are much better than US in detecting an undescended testis that is located abdominally. In one study evaluating an undescended testis, CT scan and ultrasonographic accuracy were 96% and 91%, respectively. A lymph node can be differentiated readily by the presence of fatty hilum and its characteristic location.
Magnetic Resonance Imaging
Perform MRI from the level of the kidneys to the level of the pelvic outlet. The pulse sequences used are T1, T2, and postgadolinium T1-weighted images in the axial and coronal planes. An oval mass that appears as low signal on T1-weighted images and high signal on T2-weighted images is characteristic of an undescended testis. Identification of the mediastinum testis is helpful. [17] MRI detects the malignant degeneration in cryptorchid testis well. [18]
Gadolinium-based contrast agents have been linked to the development of nephrogenic systemic fibrosis (NSF) or nephrogenic fibrosing dermopathy (NFD). The disease has occurred in patients with moderate to end-stage renal disease after being given a gadolinium-based contrast agent to enhance MRI or MRA scans. NSF/NFD is a debilitating and sometimes fatal disease. Characteristics include red or dark patches on the skin; burning, itching, swelling, hardening, and tightening of the skin; yellow spots on the whites of the eyes; joint stiffness with trouble moving or straightening the arms, hands, legs, or feet; pain deep in the hip bones or ribs; and muscle weakness.
Occasionally, bowel loops and lymph nodes can mimic the undescended testis. CT scanning is much better at differentiating the undescended testis from the bowel loop.
Ultrasonography
Ultrasonography is the most frequently used imaging study for the testicle. On US, prepubertal testes are of low- to medium-level echogenicity. The American Urological Association (AUA) recommends that a scrotal ultrasound not be performed in the preoperative management of cryptorchidism. The sensitivity and specificity of ultrasound to localize nonpalpable testes have been estimated to be 45% and 78%, respectively. Surgical intervention for cryptorchidism should be completed by 12 to 18 months of age; however, successful scrotal repositioning of the testis may reduce but not prevent infertility and testicular cancer. [10, 11, 12]
A normal adult testis has medium-level echoes and measures 5 × 3 × 2 cm. The tunica albuginea is the fibrous covering of the testicle. Septa extend from the tunica albuginea into the testicle, dividing the testes into lobules. The posterior surface of the tunica albuginea is reflected into the interior of the gland, forming the incomplete septum termed the mediastinum of the testis. Sonographically, this is seen as an echogenic band running across the testis. [19, 20, 21]
The most common location of cryptorchid testis is the inguinal canal (72%), followed by prescrotal (20%) and abdominal (8%) locations. The presence of an oval mass in the inguinal canal (relatively hypoechoic in echo texture with echogenic mediastinum) is diagnostic. [22]
(See the image below.)
Longitudinal sonogram of the right cryptorchid testis at the level of the inguinal canal. Intratesticular spectral Doppler waveform demonstrates normal low-resistance pattern of flow.
Rarely, an undescended testis can be confused with an inguinal hernia; real time peristalsis confirms the presence of bowel.
Persistence of pars infravaginalis gubernaculi has been mistaken for the testis. The presence of an echogenic band (mediastinum testis) identifies the maldescended testis.
Angiography
Testicular venography has fallen out of favor because of the availability of noninvasive tests. The following findings are diagnostic:
-
Demonstrated presence of the pampiniform plexus
-
Visualization of testicular parenchyma
-
A blind-ending testicular vein (usually indicates absent testis)
Angiography is accurate but invasive; thus, it is not preferred. Gadolinium infusion MR venography is an alternative, noninvasive method of evaluating the undescended testis, especially the vanishing testis. It is superior to MRI alone.
-
Longitudinal sonogram of the right cryptorchid testis at the level of the inguinal canal. Intratesticular spectral Doppler waveform demonstrates normal low-resistance pattern of flow.


