Practice Essentials
Cryptococcus neoformans is a yeast that most commonly infects the central nervous system (CNS). [1] Most initial cryptococcal infections occur through inhalation of the yeast from the environment. Cryptococci have large polysaccharide capsules that strongly resist phagocytosis; the inflammatory reaction to the inhaled organisms produces a primary pulmonary–lymph node complex, which usually limits spread of the yeast from this site. C neoformans spreads from the lung and intrathoracic lymph nodes to circulate in the blood, especially if the host is immunocompromised. Approximately 95% of cryptococcal infections are caused by C neoformans (serotype A) strains, and 4-5% are caused by C neoformans (serotype D) or C gattii (serotypes B/C strains). [2] Signs and symptoms at onset may be nonspecific and include headache, fever, malaise, nausea, vomiting, and cranial nerve abnormalities. [3] Even among patients receiving antifungal therapy, mortality is more than 30%. [4]
Dissemination may occur during primary infection or during reactivation of the infection years later. The most commonly involved site is the CNS. Although the prevalence of cryptococcosis has decreased among HIV-infected patients, it still accounts for over 600,000 deaths each year globally, mainly in areas with less access to antiviral treatments. [4] In addition, the incidence has been increasing in other immunosuppressed populations. A multicenter, longitudinal cohort study of 145 HIV-negative immunocompromised patients with cryptococcosis found 49% had CNS involvement. Among those with CNS disease, high and recurrent neurologic morbidities were recorded, and mortality risk increased as compared to patients without CNS disease. [5]
In cases of cryptococcal meningoencephalitis that are not associated with HIV infection, the cryptococcal infection is often confined to the subarachnoid and perivascular Virchow-Robin spaces (see the image below). [6, 7]
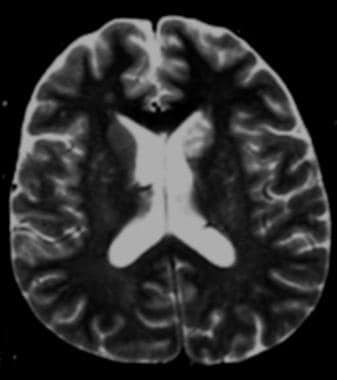 Axial T2-weighted magnetic resonance image shows clustered hyperintensities in the left caudate; these are consistent with enlarged Virchow-Robin spaces caused by small cryptococcomas.
Axial T2-weighted magnetic resonance image shows clustered hyperintensities in the left caudate; these are consistent with enlarged Virchow-Robin spaces caused by small cryptococcomas.
Imaging modalities
Although the diagnosis of CNS cryptococcosis is made on the basis of a series of microbiologic investigations, computed tomography (CT) scanning and magnetic resonance imaging (MRI) are important diagnostic techniques in any patient with HIV infection or a patient with acquired immunodeficiency syndrome (AIDS) and neurologic dysfunction. Several studies have shown that MRI is superior to CT in detecting abnormalities in patients with CNS cryptococcosis, [8] but with both imaging modalities, the number of lesions revealed is fewer than the number seen on pathologic examination [9] Normal MRI findings do not exclude CNS cryptococcosis, because the typical features of this infection occur in only 40% of patients. [10, 11, 12, 13, 14]
Computed Tomography
CT scan findings are often nonspecific for CNS cryptococcosis. In a retrospective study, CT scans of 35 patients with intracranial cryptococcal infection demonstrated unremarkable findings in 43% of the patients. [15] However, positive findings included diffuse atrophy (34%), cryptococcomas (11%), hydrocephalus (9%), and diffuse cerebral edema (3%).
Cryptococcomas appear as round, hypoattenuating or isoattenuating lesions that occur less commonly as gelatinous pseudocysts (rather than as granulomas or abscesses). In immunologically intact hosts, the cryptococci usually induce a chronic granulomatous reaction; on CT scans, these cerebral cryptococcal granulomas appear as hypoattenuating or isoattenuating lesions, with or without enhancement.
Intracranial mass lesions occur frequently in patients with AIDS. The most common mass lesions detected by CT scanning or MRI are abscesses from toxoplasmosis, although lymphoma and less common infectious processes, such as cryptococcomas, must also be considered. [16]
Magnetic Resonance Imaging
Cryptococcal meningitis is the most common CNS manifestation of cryptococcosis; the disease often has an insidious course (see the image below). In cases of AIDS-related cryptococcal meningitis, leptomeningeal enhancement is not always seen on CT scans or MRIs. [9, 10, 17, 18, 19]
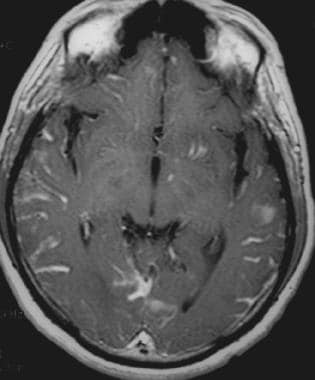 Axial contrast-enhanced T1-weighted magnetic resonance image shows diffuse, gyriform leptomeningeal enhancement. Enhancing lesions in the left basal ganglia, left temporal lobe, and left occipital lobe correspond to intraparenchymal cryptococcosis.
Axial contrast-enhanced T1-weighted magnetic resonance image shows diffuse, gyriform leptomeningeal enhancement. Enhancing lesions in the left basal ganglia, left temporal lobe, and left occipital lobe correspond to intraparenchymal cryptococcosis.
The cryptococcal organism is surrounded by a polysaccharide capsule, which may protect it from the host inflammatory response even in immunocompetent patients. In response to the attack on the organisms by the host's immune system, the cryptococci produce a mucoid material. In a study by Arnder et al of 3 patients who were diagnosed with cryptococcal meningitis, 2 patients demonstrated thick enhancing subarachnoid spaces on postcontrast MRIs. [20] The diagnoses were confirmed at autopsy. In the postmortem MRI and pathologic examinations of the third patient, these areas of enhancement corresponded to the abundant mucoid material secreted by the organisms. [20]
Cryptococcal organisms spread from the basal cisterns through the Virchow-Robin spaces to the basal ganglia (as shown in the images below), internal capsule, thalamus, and brainstem. [7] The perivascular spaces may be enlarged as a result of the production of voluminous mucoid material. MRI is more sensitive than CT scanning in demonstrating abnormalities such as dilated perivascular spaces. These manifest on T2-weighted MRIs as punctate, hyperintense, round or oval lesions that are usually smaller than 3 mm. Enlarged perivascular spaces are not always a consequence of cryptococcosis; they may be the result of age-related changes or HIV-related atrophy.
Axial contrast-enhanced T1-weighted magnetic resonance image shows diffuse, gyriform leptomeningeal enhancement. Enhancing lesions in the left basal ganglia, left temporal lobe, and left occipital lobe correspond to intraparenchymal cryptococcosis.
 T1-weighted magnetic resonance image demonstrates dilated perivascular spaces in the bilateral basal ganglia.
T1-weighted magnetic resonance image demonstrates dilated perivascular spaces in the bilateral basal ganglia.
Generalized atrophy is common in patients with AIDS; however, the observation of punctate hyperintensities is suggestive of cryptococcal disease, especially if other signs of diffuse atrophy (eg, ventricular and sulcal enlargement) are not present or if the patient has clinical signs or symptoms of meningitis.
By definition, cryptococcomas represent a collection of organisms, inflammatory cells, and gelatinous mucoid material in the brain parenchyma. Cryptococcomas may develop when organisms have extended directly from perivascular spaces into the parenchyma (see the following images) or, possibly, when they have invaded the parenchyma from other meningeal or ependymal surfaces.
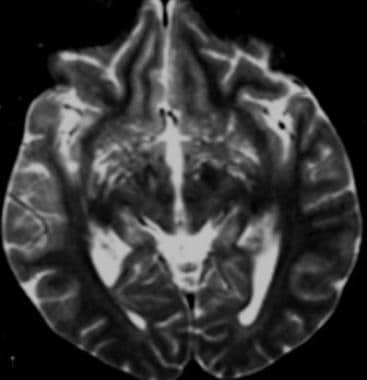 T2-weighted axial magnetic resonance image demonstrates linear and punctate hyperintensities in the basal ganglia; these represent dilated perivascular spaces caused by small cryptococcomas. Cryptococcomas vary in size from several millimeters to several centimeters.
Axial T2-weighted magnetic resonance image shows clustered hyperintensities in the left caudate; these are consistent with enlarged Virchow-Robin spaces caused by small cryptococcomas.
T2-weighted axial magnetic resonance image demonstrates linear and punctate hyperintensities in the basal ganglia; these represent dilated perivascular spaces caused by small cryptococcomas. Cryptococcomas vary in size from several millimeters to several centimeters.
Axial T2-weighted magnetic resonance image shows clustered hyperintensities in the left caudate; these are consistent with enlarged Virchow-Robin spaces caused by small cryptococcomas.
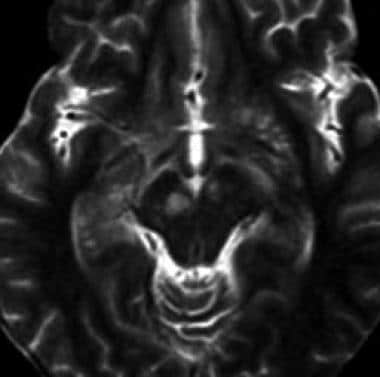 T2-weighted axial magnetic resonance image demonstrates hyperintense cryptococcomas in the midbrain.
T2-weighted axial magnetic resonance image demonstrates hyperintense cryptococcomas in the midbrain.
Cryptococcomas are hyperintense on T2-weighted images. Although contrast enhancement of cryptococcomas is uncommon in cases of AIDS-related CNS cryptococcosis, [9] it has been reported. [20] The cryptococcal organism is surrounded by a polysaccharide capsule, which may protect it from the host inflammatory response, even in immunocompetent patients.
In immunologically intact hosts, the organisms usually induce a chronic granulomatous reaction. On MRI, the most common findings are punctate masses that demonstrate low signal intensity on T1-weighted images and high signal intensity on T2-weighted images, without surrounding edema.
Choroid plexitis of the brain is a pathologic presentation of cryptococcosis. MRI demonstrates unilateral or bilateral enlargement and dense enhancement of the choroid plexus in the lateral and fourth ventricles. [21] These findings occur in association with clinical findings of leptomeningitis. The lesion may appear as an enhancing, intraventricular mass.
Unilateral cystic dilatation of the temporal horn of the lateral ventricle has also been described. [21] Cho et al believed this dilatation may be the result of entrapment of the temporal horn by inflamed choroid plexus, as well as extensive edema around the ipsilateral ventricle. [21]
Although MRI is useful as part of the initial investigation protocol for patients with suspected cryptococcal meningitis, serial imaging probably has a minimal role in monitoring response to therapy. However, magnetic resonance spectroscopy may detect changes in the metabolites that are related to inflammatory activity.
-
Axial T2-weighted magnetic resonance image shows clustered hyperintensities in the left caudate; these are consistent with enlarged Virchow-Robin spaces caused by small cryptococcomas.
-
Axial contrast-enhanced T1-weighted magnetic resonance image shows diffuse, gyriform leptomeningeal enhancement. Enhancing lesions in the left basal ganglia, left temporal lobe, and left occipital lobe correspond to intraparenchymal cryptococcosis.
-
T1-weighted magnetic resonance image demonstrates dilated perivascular spaces in the bilateral basal ganglia.
-
T2-weighted axial magnetic resonance image demonstrates linear and punctate hyperintensities in the basal ganglia; these represent dilated perivascular spaces caused by small cryptococcomas. Cryptococcomas vary in size from several millimeters to several centimeters.
-
T2-weighted axial magnetic resonance image demonstrates hyperintense cryptococcomas in the midbrain.








