Practice Essentials
Crohn disease (CD) is a chronic idiopathic inflammatory disorder that can affect all sections of the gastrointestinal tract, but only a small minority of patients (6-14%) will have a change in disease location over time. The cardinal symptoms are abdominal pain, diarrhea, and fatigue. Other signs and symptoms include weight loss, fever, growth failure (in pediatric patients), anemia, recurrent fistulas, and extraintestinal manifestations. [1]
The diagnosis of Crohn disease is confirmed by clinical evaluation and a combination of endoscopic, histologic, radiologic, and biochemical investigations. [1, 2] CT scanning provides cross-sectional images for assessing mural and extramural involvement; endoscopy enables direct visualization of the mucosa and provides the ability to obtain a biopsy specimen for histopathologic correlation; and ultrasonography and MRI are adjuncts that provide alternative cross-sectional images in populations in whom radiation exposure is a concern.
Crohn disease is characterized by cycles of remission and exacerbation. The chronic and recurrent disease course requires repeated endoscopic, biochemical, and imaging examinations to determine the most appropriate treatment and the prognosis. The American College of Gastroenterology (ACG) guidelines for the management of Crohn disease note that symptoms do not correlate well with the presence of active inflammation and, therefore, should not be the sole guide for therapy. Thus, it is recommended that objective periodic evaluation by endoscopic or cross-sectional imaging be performed to avoid undertreatment or overtreatment. [1] (See Guidelines, below.)
Preferred examination
Cross-sectional CT and MR enterography are the preferred imaging tests for the initial diagnosis, evaluation of acute flare, and surveillance of patients with suspected and known Crohn disease. (See the images below.) For the initial examination in an adult patient with suspected Crohn disease, CT enterography is preferred because it is much less dependent on bowel and respiratory motion. In a severely ill or young patient, the ability to perform any of these examinations may be impacted. High-quality MR enterography (MRE) provides the opportunity to eliminate radiation exposure for children, young adults, and nonacutely ill adults while maintaining a sensitivity similar to that of CT enterography (CTE).ref3}
The small bowel is one of the most common areas affected by inflammation in Crohn disease, and much of the inflammation is beyond the reach of standard endoscopic evaluation. In up to 50% of patients with active small bowel disease, inflammation may skip the terminal ileum or may be intramural and, therefore, may not be detected by ileocolonoscopy. [3] ACG guidelines recommend performing small bowel imaging as part of the initial diagnostic workup for patients with suspected Crohn’s disease. The selection of small bowel imaging study should be based on the expertise of the institution and the clinical presentation of the patient. [1]
Traditionally, MRI was limited in the evaluation of the abdomen and pelvis because of motion artifact. With stronger gradients, breath-hold imaging, and faster sequences, MRI of the abdomen and pelvis can be readily performed in most patients. It is currently actively used in routine assessment of pelvis fistulae and sinus tracts. In many medical centers, MRI enterography and enteroclysis are actively used in surveillance of small bowel disease and extraluminal mesenteric disease. MRI is an attractive alternative to traditional fluoroscopy and CT scanning, especially in pediatric patients for whom long-term radiation exposure is a concern. [4, 5, 6] The ACG prefers magnetic resonance enterography (MRE) in patients younger than 35 years and in patients undergoing serial imaging. [1]
Transabdominal ultrasound can be an effective option in the initial diagnosis of Crohn disease; however, accuracy depends on the skill of the opperator. In addition, with expert operator skill, ultrasound can detect complications of Crohn disease in ranges similar to those of other cross-sectional imaging modalities. Sensitivities for fistulas have been reported to be in the range of 71 to 82%, with abscess detection at 80%. Detection of abscesses is likely decreased as compared to CT, because some areas are difficult to visualize related to the stomach or sigmoid/rectum. In cases of suspected bowel perforation, detection of free intraperitoneal air is poor unless it is present in large amounts. [7]
Fluoroscopic examinations (small-bowel series and barium enema) are infrequently performed, but they may still be helpful for preoperative planning. Nuclear medicine examinations may be helpful in certain cases, but they are not widely used. [7]
(Examples of Crohn disease are provided in the images below.)
 Crohn disease. Aphthous ulcers. Double-contrast barium enema examination in Crohn colitis demonstrates numerous aphthous ulcers.
Crohn disease. Aphthous ulcers. Double-contrast barium enema examination in Crohn colitis demonstrates numerous aphthous ulcers.
 Crohn disease of the terminal ileum with CT and sonographic correlation. Small-bowel follow-through study demonstrates the string sign in the terminal ileum. Also note pseudodiverticula of the antimesenteric wall of the terminal ileum, secondary to greater distensibility of this less-involved segment of the wall.
Crohn disease of the terminal ileum with CT and sonographic correlation. Small-bowel follow-through study demonstrates the string sign in the terminal ileum. Also note pseudodiverticula of the antimesenteric wall of the terminal ileum, secondary to greater distensibility of this less-involved segment of the wall.
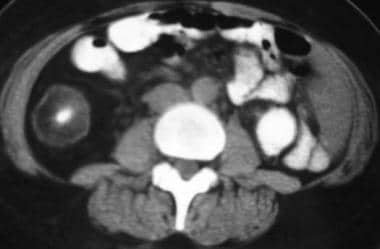
 Crohn disease of the terminal ileum with CT and sonographic correlation. Note terminal ileal-wall thickening and adjacent mesenteric inflammatory stranding.
Crohn disease of the terminal ileum with CT and sonographic correlation. Note terminal ileal-wall thickening and adjacent mesenteric inflammatory stranding.
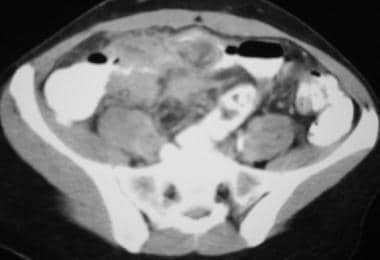 Crohn disease. Mesenteric inflammation. CT scan demonstrates inflammatory mass in the right lower quadrant associated with thickening of the wall and narrowing of the lumen of the terminal ileum.
Crohn disease. Mesenteric inflammation. CT scan demonstrates inflammatory mass in the right lower quadrant associated with thickening of the wall and narrowing of the lumen of the terminal ileum.
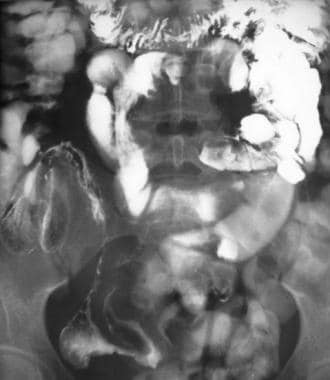
 Crohn disease. Crohn colitis. Double-contrast barium enema study demonstrates marked ulceration, inflammatory changes, and narrowing of the right colon.
Crohn disease. Crohn colitis. Double-contrast barium enema study demonstrates marked ulceration, inflammatory changes, and narrowing of the right colon.
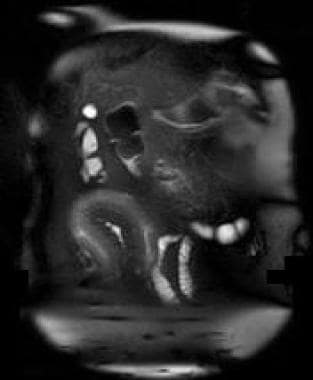
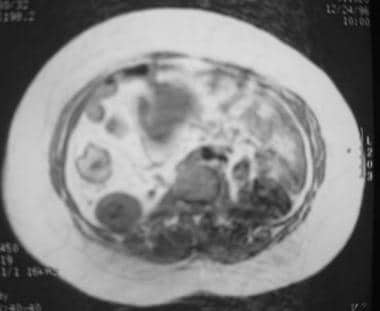 Crohn disease. MRI with CT correlation. MRI demonstrates thickening of the wall of the right colon with intramural increased signal on a T1-weighted image. This was believed to represent intramural fat deposition.
Crohn disease. MRI with CT correlation. MRI demonstrates thickening of the wall of the right colon with intramural increased signal on a T1-weighted image. This was believed to represent intramural fat deposition.
Guidelines
An expert panel of members from the Society of Abdominal Radiology Crohn’s Disease–Focused Panel, the Society of Pediatric Radiology, and the American Gastroenterological Association issued the following guidelines on the use of computed tomography enterography (CTE) and magnetic resonance enterography (MRE) in patients with small bowel Crohn disease [8, 9] :
-
The number of involved bowel segments and their location, as well as the length and degree of upstream dilatation of Crohn strictures, should be reported by radiologists to help gastroenterologists and surgeons determine the best therapeutic plan.
-
Radiologists should state if mural inflammation is present when describing areas with stricture or penetrating disease.
-
Cross-sectional enterography should be performed at Crohn disease diagnosis.
-
Consider cross-sectional enterography for disease monitoring in patients with small bowel disease or penetrating complications.
-
While a dedicated pelvic magnetic resonance (MR) study is needed in patients with perianal disease, all CTEs and MREs should also include imaging of the anus.
-
Radiologists should comment on and describe intramural T2 hyperintensity, restricted diffusion, perienteric stranding, wall thickness, and mural ulcerations seen on imaging, because they typically correlate with disease severity.
-
MRE is preferred over CTE to estimate response to medical treatment in patients with asymptomatic disease.
-
Noncontrast MRE with T2-weighted and diffusion-weighted imaging is an “acceptable alternative” when intravenous contrast agents cannot be used.
-
Radiologists should evaluate CTE and MRE examinations for signs of mesenteric venous thrombosis, occlusions, or small bowel varices.
CT-guided therapy
CT has become the procedure of choice not only in diagnosing Crohn disease but also in managing abscesses. A growing body of literature shows that CT-guided percutaneous abscess drainage may obviate surgery. CT percutaneous abscess drainage has shown great success either as a temporizing measure or as definitive therapy with a decreased rate of recurrence, as compared with that of surgery. Because about 70-90% of patients with regional enteritis eventually require surgery, avoiding an operation to treat an abscess is a tangible benefit of CT. [10]
Complications and contraindications
The oral administration of contrast material is to be avoided when moderate- or high-grade colonic obstruction is present. Double-contrast (air contrast) barium enema examination is contraindicated in patients with severe colitis, because injection of air with contrast agent may precipitate toxic megacolon or colonic perforation. Barium studies are contraindicated when there are signs and symptoms of peritonitis or when there are radiographic signs of gas in the bowel wall or pneumoperitoneum. [11]
The intravenous injection of contrast material for CT studies should be avoided when chronic renal insufficiency is present, when there is continued use of Glucophage, or when there are signs and symptoms of acute renal failure. CT and barium studies use ionizing radiation, which may result in considerable radiation burden. This exposure is a relative contraindication in pregnancy and childhood. Sonography and MRI may prove to be useful alternative imaging modalities.
Pathophysiology
The etiology of Crohn disease is largely unknown. Genetic, infectious, immunologic, and psychological factors have all been implicated in influencing the development of the disease. The disease is characterized by chronic inflammation extending through all layers of the intestinal wall and involving mesentery as well as regional lymph nodes.
Early mucosal involvement consists of longitudinal and transverse aphthous ulcerations, which are responsible for a cobblestone appearance. As the disease progresses, deep fissures, sinuses, and fistulae develop. Eventually, communication between diseased bowel segments, the abdominal wall, retroperitoneal structures, and the urinary tract occurs.
Because of the transmural nature of the disease, mesenteric and perianal manifestations are fairly common. Because of the inflammation, strictures resulting from edema, inflammation, and, ultimately, fibrosis and scarirng are frequent. Crohn disease is pervasive. The basic pathologic process of disease can occur at any segment of the alimentary tract.
Crohn disease and ulcerative colitis share similar inflammatory changes. Cryptitis and subsequent crypt abscesses consisting of polymorphonuclear cells are identical for the 2 diseases. However, during the inflammatory flare-ups, Crohn disease involves increases in the number of cells containing immunoglobulin G2 (IgG2), and ulcerative colitis involves a predominant increase in immunoglobulin G1 (IgG1) and immunoglobulin G3 (IgG3) cell types.
The inflammatory infiltrate of the lamina propria in Crohn disease leads to loose aggregations of macrophages, and they organize into noncaseating granulomas, which involve all layers of the bowel wall from mucosa to serosa. Occasionally, they can be seen on laparoscopy as miliary nodules, and they function as contiguous spread of the disease from the intestine. With chronic inflammation, the bowel walls become thickened, fibrotic, and stenotic in Crohn disease, and an extension of inflammation and fistula formation often occurs as a result of a transmural fissure.
In ulcerative colitis, hemorrhagic and ulcerative inflammation is mostly limited to the mucosa, with recurrence leading to atrophic mucosa. Ulcers often have irregular borders, giving rise to a collar-stud effect. In recurrent disease, inflammatory polyps develop from exuberant epithelial regeneration. When inflammation infiltrate extends into the submucosa and muscularis propria, it does so in a diffuse pattern, in contrast to Crohn disease, in which lymphoid aggregates occur. Why Crohn disease has a skip-distribution as opposed to that seen in ulcerative colitis is uncertain.
Epidemiology
Findings from studies in the United States and Western Europe indicate that the incidence of Crohn disease is 2 cases per 100,000 population. The prevalence is estimated to be 20-40 cases per 100,000 population. Recent data show that at least in Europe, rates in Southern European countries are catching up to those of their northern neighbors.
Approximately 15% of the cases of Crohn disease appear in persons older than 50 years.
The relative risk for adenocarcinoma of the ileum is at least 100-fold greater in Crohn disease patients than in age- and sex-matched controls. Small-bowel cancers typically arise at sites of macroscopic disease after a mean age of 18 years.
For excellent patient education resources, visit eMedicineHealth's Digestive Disorders Center. Also, see eMedicineHealth's patient education articles Inflammatory Bowel Disease, Crohn Disease, and Crohn Disease FAQs.
Radiography
The role of plain radiography with barium studies in Crohn disease is fairly limited. Endoscopy has been found to be superior to barium enema for the detection of early inflammatory changes and has largely replaced it as the initial diagnostic examination. The American College of Radiology (ACR) appropriateness criteria find it is usually not appropropriate as a first-line modality for diagnosis of Crohn disease. [7]
Radiographs of the abdomen are limited in the initial diagnosis for CD. The ability to directly visualize bowel pathology is limited, and the diagnosis of Crohn disease is indirectly inferred. Radiographs may be useful in severely ill patients for assessment of complications related to Crohn disease, including evidence for free air in bowel perforation or evidence for obstruction. [7]
Aphthoid ulcers
Aphthoid ulcers, as shown in the image below, are detected on barium studies in 25-50% of patients with Crohn disease. These are identified in as many as 75% of surgical specimens with Crohn disease. Endoscopy is slightly superior to barium studies in the demonstration of isolated or a few aphthoid ulcers.
Crohn disease. Aphthous ulcers. Double-contrast barium enema examination in Crohn colitis demonstrates numerous aphthous ulcers.
Cobblestoning
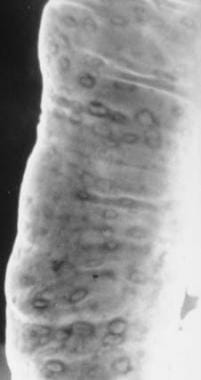
As inflammation penetrates the submucosa and muscularis layers, deep knifelike linear clefts form the basis of "cobblestoning" and fissure or fistula formation. They appear as a barium-filled reticular network of grooves that surround round or ovoid radiolucent islands of mucosa. Eventually, transmural inflammation leads to decreased luminal diameter and limited distensibility. This leads to a radiographic string sign that represents long areas of circumferential inflammation and fibrosis resulting in long segments of luminal narrowing. (See the image below.)
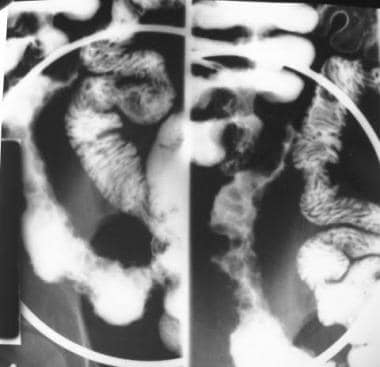 Crohn disease. Cobblestoning. Spot view of the terminal ileum from a small-bowel follow-through study demonstrates linear longitudinal and transverse ulcerations that create a cobblestone appearance. Also note the relatively greater involvement of the mesenteric side of the terminal ileum and the displacement of the involved loop away from the normal small bowel secondary to mesenteric inflammation and fibrofatty proliferation.
Crohn disease. Cobblestoning. Spot view of the terminal ileum from a small-bowel follow-through study demonstrates linear longitudinal and transverse ulcerations that create a cobblestone appearance. Also note the relatively greater involvement of the mesenteric side of the terminal ileum and the displacement of the involved loop away from the normal small bowel secondary to mesenteric inflammation and fibrofatty proliferation.
Computed Tomography
The role of CT in the evaluation of Crohn disease is well accepted. The ability of CT to depict bowel involvement and extraluminal pathology (eg, abscess, obstruction, fistula) makes it an essential imaging tool for patient care. For the detection of intra-abdominal abscesses, the sensitivity, specificity, and accuracy of CT are comparable to those of surgical findings. [3]
The earliest CT finding of Crohn disease is bowel wall thickening, which usually involves the distal small bowel and colon, although any segment of the GI tract can be affected. Typically, the luminal thickening is 5-15 mm. [6, 12, 13, 14, 15]
CT should be the first radiologic procedure performed in patients with acute symptoms and suspected or known Crohn disease. [1, 2, 7, 16] The ability to directly demonstrate the bowel wall, adjacent abdominal organs, mesentery, and retroperitoneum makes CT superior to barium studies in diagnosing the complications of Crohn disease. CT directly demonstrates bowel wall thickening, mesenteric edema, and lymphadenopathy, as well as phlegmon and abscess. (See the images below.)
Crohn disease of the terminal ileum with CT and sonographic correlation. Small-bowel follow-through study demonstrates the string sign in the terminal ileum. Also note pseudodiverticula of the antimesenteric wall of the terminal ileum, secondary to greater distensibility of this less-involved segment of the wall.
Crohn disease of the terminal ileum with CT and sonographic correlation. Note terminal ileal-wall thickening and adjacent mesenteric inflammatory stranding.
 Crohn disease. Active small-bowel inflammation. CT scan demonstrates small-bowel wall thickening, mesenteric inflammatory stranding, and mesenteric adenopathy.
Crohn disease. Mesenteric inflammation. CT scan demonstrates inflammatory mass in the right lower quadrant associated with thickening of the wall and narrowing of the lumen of the terminal ileum.
Crohn disease. Active small-bowel inflammation. CT scan demonstrates small-bowel wall thickening, mesenteric inflammatory stranding, and mesenteric adenopathy.
Crohn disease. Mesenteric inflammation. CT scan demonstrates inflammatory mass in the right lower quadrant associated with thickening of the wall and narrowing of the lumen of the terminal ileum.
Certain distinguishing features have been cited in delineating Crohn disease from other forms of enterocolitis, including differences in wall thickness and attenuation; the distribution of colonic wall involvement; and the presence or absence of abscesses, fistulas, small-bowel disease, and mesenteric fibrofatty proliferation. In using the mentioned features, CT can attain positive predictive value above 90% and a diagnostic accuracy as high as 93%. [17] (See the image below.)
 Crohn disease. Fibrofatty proliferation. CT scan in a patient with Crohn colitis in the chronic phase demonstrates wall thickening of the right colon, an absence of adjacent mesenteric inflammatory stranding, and a large amount of fatty proliferation around the right colon separating the colon from the remainder of the gut, so-called creeping fat.
Crohn disease. Fibrofatty proliferation. CT scan in a patient with Crohn colitis in the chronic phase demonstrates wall thickening of the right colon, an absence of adjacent mesenteric inflammatory stranding, and a large amount of fatty proliferation around the right colon separating the colon from the remainder of the gut, so-called creeping fat.
The introduction of multidetector-row CT scanners with thinner collimation and faster intravenous injections of contrast material have allowed more detailed evaluation of the bowel. The enhancement of the bowel wall after intravenous contrast enhancement is correlated with the enlargement of the feeding vessel and hyperemia during active disease. In an article by Del Campo et al, patients with active disease had a bowel wall attenuation of 95 HU, as compared with 65 HU in patients with disease in remission. [18] The ability to measure bowel wall enhancement may prove valuable in treating patients with Crohn disease.
One limitation of CT has been in the area of delineating active versus inactive disease. The presence of mesenteric stranding does not reliably signify active disease because residual mesenteric thickening can remain during remission.
Ulcerations
Ulcerations in the mucosa can be detected on thin-section CT, although small-bowel series or enteroclysis is more sensitive to the early mucosal changes of Crohn disease. In addition, mesenteric stranding, increase in mesenteric fat, local adenopathy, fistula, and abscess are readily and commonly identified on CT scans.
Hazy fat
Edema or mild inflammation of the mesenteric fat results in increased attenuation, the so-called hazy fat on CT. Greater inflammation or fibrosis results in attenuating linear bands of soft tissue coursing through the mesentery. On CT, an ill-defined inflamed mass of mixed attenuation may represent a phlegmon or early abscess formation. Enlarged lymph nodes are usually seen in proximity to the bowel wall along the mesenteric course of the vascular bundle. (See the image below.)
 Crohn disease. Mesenteric inflammation. CT scan demonstrates an inflammatory mass in the right lower quadrant associated with thickening of the wall and narrowing of the lumen of the terminal ileum.
Crohn disease. Mesenteric inflammation. CT scan demonstrates an inflammatory mass in the right lower quadrant associated with thickening of the wall and narrowing of the lumen of the terminal ileum.
Abscesses
On CT scans, abscesses appear as well-defined, round or oval masses of fluid attenuation, and they are often multilocular. Pockets or bubbles of gas usually result from fistulous communication with bowel or, less likely, from infection by gas-producing organisms.
Crohn disease versus ulcerative colitis
There is considerable overlap between CT findings of ulcerative colitis and Crohn disease. Despite this fact, certain defining features of each disease have been characterized. Ulcerative colitis is predominantly a mucosal disease. However, with progression of illness, there is hypertrophy of the muscularis often by 40-fold, increased submucosa fatty deposition, and thickening of the lamina propria from round cell infiltration, which all leads to bowel wall thickening. On average, thickening of the luminal wall is 7.8 mm in ulcerative colitis, which is less than the amount of wall thickening typically seen with Crohn disease.
Submucosal fat is a prominent finding in chronic ulcerative colitis and is one of the defining features of the mural stratification seen in ulcerative colitis. In comparison, Crohn disease has transmural involvement that over time leads to replacement of submucosal fat with fibrosis and loss of mural stratification. In distinction to ulcerative colitis, Crohn disease also has several extraluminal CT findings, including mesenteric fibrofatty proliferation and abscess.
(Additional images of Crohn disease on CT scanning are provided below.)
 Crohn disease. CT with MRI correlation. CT scan in a patient with chronic inactive Crohn disease demonstrates thickening of the wall of the right colon with intramural lucency. This was believed to represent intramural fat deposition.
Crohn disease. MRI with CT correlation. MRI demonstrates thickening of the wall of the right colon with intramural increased signal on a T1-weighted image. This was believed to represent intramural fat deposition.
Crohn disease. CT with MRI correlation. CT scan in a patient with chronic inactive Crohn disease demonstrates thickening of the wall of the right colon with intramural lucency. This was believed to represent intramural fat deposition.
Crohn disease. MRI with CT correlation. MRI demonstrates thickening of the wall of the right colon with intramural increased signal on a T1-weighted image. This was believed to represent intramural fat deposition.
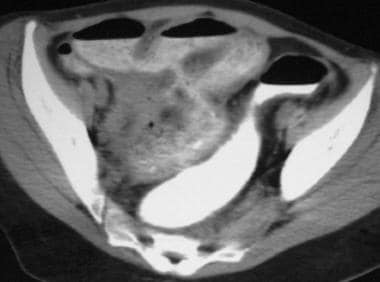
 Crohn disease. Perianal abscesses. CT scan demonstrates multiple fluid, contrast material, and air collections around the anorectum. Note the presence of a rectal tube.
Crohn disease. Perianal abscesses. CT scan demonstrates multiple fluid, contrast material, and air collections around the anorectum. Note the presence of a rectal tube.
 Crohn disease. Perianal abscesses. CT scan demonstrates multiple fluid, contrast agent, and air collections around the anorectum. Note the presence of a rectal tube.
Crohn disease. Perianal abscesses. CT scan demonstrates multiple fluid, contrast agent, and air collections around the anorectum. Note the presence of a rectal tube.
 Crohn disease. Small-bowel obstruction in a patient with recurrence proximal to an anastomosis. CT scan in a patient with a prior ileocolectomy demonstrates small-bowel dilatation and wall thickening of the small bowel proximal to the anastomosis.
Crohn disease. Small-bowel obstruction in a patient with recurrence proximal to an anastomosis. CT scan in a patient with a prior ileocolectomy demonstrates small-bowel dilatation and wall thickening of the small bowel proximal to the anastomosis.
 Crohn disease. Enteroenteric fistula. CT scan demonstrates the tract of an enteroenteric fistula.
Crohn disease. Enteroenteric fistula. CT scan demonstrates the tract of an enteroenteric fistula.
 Crohn disease. Enterocutaneous fistula. CT scan demonstrates enterocutaneous and colocutaneous fistula formation.
Crohn disease. Enterocutaneous fistula. CT scan demonstrates enterocutaneous and colocutaneous fistula formation.
Magnetic Resonance Imaging
Traditionally, MRI has had a well-defined role in evaluation of anorectal complications of Crohn disease. With a regular fast spin-echo technique, the pathologic entities of a fistula, a sinus tract, and an abscess can be detected in the static anorectal region by using MRI. [19] In addition, MRI enterography and enteroclysis has allowed detection of small bowel Crohn disease, similar to that of small bowel series, with the additional benefits of assessment of extraluminal disease. [20] High-resolution imaging with the current MRI technology has increased the accuracy of assessing the grade and severity of patients with Crohn disease. [20, 21, 22, 23, 24] Its increased use and availability will likely rival traditional imaging in the assessment of this disease. [4, 5, 6, 25]
Perianal sinus tracts and fistulas
Sinus tracts and fistulas often appear hyperintense on T1-weighted images and hyperintense on T2-weighted images because of their fluid content. With fat suppression, the fluid signal is further intensified and is easily seen as being hyperintense on T2-weighted images. An abscess often appears as an isolated collection of high-signal-intensity areas on the T2-weighted image, especially in ischioanal fossa. Defining whether an abscess, fistula, or sinus tract is above or below the levator ani muscle is important for drainage, because any part of the abscess above the levator ani muscle will not drain adequately in the inferior direction, and vice versa.
MRI sequences
The development of faster pulse sequences (eg, single-shot fast spin-echo, steady-state free precession, and gradient-echo sequences) and higher-gradient systems has made T1- and T2-weighted breath-hold imaging possible. This breath-hold imaging has been a major breakthrough in overcoming physiologic motion artifacts in abdominal imaging. It has made routine abdominal MRI feasible.
In the single-shot fast spin-echo sequence, T2-weighted images are acquired by using half-Fourier transformation and a long echo train. Each image section is acquired independently in less than 1 second, and the method eliminates physiologic motion from the bowel and the need for breath-holds. Fat suppression can be added to increase specificity for bowel and mesenteric edema.
The steady-state free precession imaging is based on a low flip angle gradient echo series with short repetition time. It is another series of sequences that is insensitive to motion artifacts and can provide T2-type imaging. It can have black boundary artifacts along the bowel wall that mask small lesions, but fat suppression can reduce the artifact. The major feature of the sequence is the ability to acquire an entire series within a single breath-hold. In fact, MR fluoroscopy is performed with cine of steady-state free precession imaging and a frame rate of 0.5-2 sections per second along the long axis of the affected segments.
Contrast evaluation is often imaged with 3-dimensional spoiled gradient echo T1 fat-suppressed sequences. Images are acquired with breath-hold. For bowel imaging, series are taken after intravenous glucagon at 30 and 70 seconds post contrast.
Because of a decrease in cumulative radiation exposure and because of the capability of attaining high-quality coronal images correlating with barium studies, MRI is currently an alternative for monitoring disease activity in Crohn disease.
MRI enterography and enteroclysis
With the development of faster imaging sequence and with the use of intravenous 0.2-mg glucagon to decrease bowel motility, the small bowel is distended in both MRI enterography or enteroclysis, often with 1.5-2 L of solution containing biphasic intraluminal contrast agents (low T1 and high T2). Some of these agents are Volumen (EZ-E-M), mannitol (2.5%), methylcellulose, sorbitol (2%), and polyethylene glycol. The image is performed for 40-60 minutes subsequent to luminal distention for MRI enterography and enteroclysis.
Oral ingestion of the intraluminal contrast is performed in enterography, while nasojejunal intubation and infusion of intraluminal contrast is performed in enteroclysis. Nasojejunal intubation under fluoroscopy is required for MRI enteroclysis; it provides excellent bowel distention and provides detailed luminal information. [26] However, there is added procedure time for the fluoroscopy nasojejunal intubation, along with increased invasiveness and patient discomfort. [27, 28] These factors can be a major drawback, especially in the pediatric population.
MRI enterography is associated with less patient discomfort, but the bowel preparation may not produce the uniform distention achieved with enteroclysis. Nevertheless, several studies have shown better patient tolerance of enterography than enteroclysis, and some studies have shown similar sensitivities for the 2 techniques. [27]
Initial imaging with serial coronal steady-state free precession for the small bowel can demonstrate decreased motility in areas of small bowel disease, along with luminal thickening (wall thickness >4 mm) while monitoring adequate distention of the ileocecal lumen. After adequate luminal distention, 0.2 mg of glucagon IV or 1 mg of intramuscular glucagon is administered to reduce motion artifacts, followed by T2-weighted single-shot fast spin-echo series. The coronal and axial T2-weighted single-shot fast spin-echo images can show edema in the small bowel mesentery and small bowel wall deep ulcers, while fat-saturated images can determine chronic mural fat changes. Lastly, after administration of a gadolinium-based intravenous contrast agent, coronal volume gradient-echo sequences are acquired to assess vascular engorgement, mucosal hyperemia, mural enhancement, inflammatory hyperenhancing lymph nodes, abscess, and fistula.
There are ongoing investigations into the use of MRI enterography and assessment of active disease in the colon.
Active Crohn disease
Assessment of inflammatory activity is fundamental to the management of Crohn disease. Clinical scores such as the Crohn disease activity index and biochemical markers such as C-reactive protein are widely used, but they lack utility for assessment of the entire bowel. [23] Endoscopy is the current reference standard for evaluation of disease of the colon and terminal ileum. It has the key advantages of direct visualization and sampling of disease, but it is limited in its assessment of the entire small bowel. MRI currently serves as a viable method for global assessment.
Many of the MRI criteria of disease activity are based on luminal and extraluminal disease. In terms of luminal disease, active disease includes ulcer, wall thickening, mural and perimural T2 intensity, and bowel wall enhancement with gadolinium-based contrast agents. [23] Extraluminal active disease includes enlarged inflammatory lymph nodes, fibrofatty proliferation, and mesenteric edema.
During active inflammation, gadolinium enhancement of the bowel wall can be seen on T1-weighted images, and it is easily differentiated from normal adjacent bowel. There are 3 main patterns of enhancement in determining the level of disease. The layered or stratified enhancement is seen with enhancement of the mucosa, and relatively poor submucosal enhancement and submucosal edema are seen in active disease. [29, 30, 31] Diffuse, intense homogeneous enhancement of the entire bowel wall thickness occurs from transmural inflammation. [32] Low-level heterogeneous enhancement occurs with fibrosis. [33] (See the image below.)
 MRI enterography 3-dimensional gradient postcontrast series demonstrates stratified hyperenhancement of the mucosa of the distal ileum in a patient with active Crohn disease.
MRI enterography 3-dimensional gradient postcontrast series demonstrates stratified hyperenhancement of the mucosa of the distal ileum in a patient with active Crohn disease.
Wall thickening is variable in active disease, as described in many reports. The general consensus is that concentric bowel wall thickening greater than 4 mm is suggestive of active disease. In study by Maccioni et al, active disease was characterized by a thickened bowel wall with gadolinium enhancement, but inactive disease was not. [34] With the advent of MRI enteroclysis, and to a lesser degree optimal enterography, alteration of folds in early active Crohn disease can be seen as diffuse thickened folds as in a picket-fence pattern, reduction and distortion of folds secondary to ulceration, and cobblestoning on single-shot spin-echo series. [33] (See the image below.)
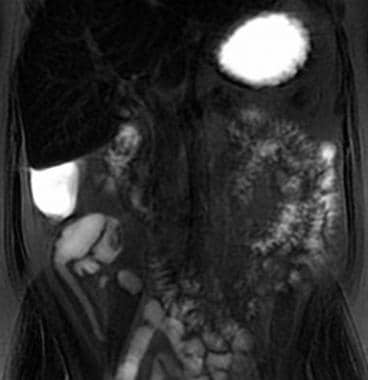
 MRI enterography with coronal fat-saturated T2-weighted single-shot fast spin echo imaging demonstrates mesenteric edema and mural wall edema and thickening in a patient with active Crohn disease in the distal ileum.
MRI enterography with coronal fat-saturated T2-weighted single-shot fast spin echo imaging demonstrates mesenteric edema and mural wall edema and thickening in a patient with active Crohn disease in the distal ileum.
Fat-suppressed T2-weighted images can also be used for differentiation because they show high-signal intensity in active disease and low or absent signal intensity in nonactive disease. Mural T2 increased signal intensity is a well-validated marker of disease activity. [30, 34, 35, 36, 37, 38] In fact, the fat suppression in T2-weighted images helps differentiate fibrofatty changes of mural disease from mural wall edema.
Ulceration in active Crohn disease is highly dependent on the quality of luminal distention and is best depicted by MRI enterography and enteroclysis. Deep ulcers appear as thin lines of high signal within a thickened bowel wall on single-shot fast spin-echo series and can be seen more readily on MRI enterography, whereas aphthous ulcer, with a nidus of high signal with surrounding intermediate signal, can be seen on high-resolution MRI enteroclysis. (See the image below.)
 MRI enterography coronal single-shot fast spin-echo images in a patient with active Crohn disease demonstrates wall thickening and wall deep fissuring along an ascending limb of the distal ileum small bowel loop in the right lower quadrant of the abdomen.
MRI enterography coronal single-shot fast spin-echo images in a patient with active Crohn disease demonstrates wall thickening and wall deep fissuring along an ascending limb of the distal ileum small bowel loop in the right lower quadrant of the abdomen.
Fibrofatty proliferation is hyperintense on T2-weighted images and is related to regional mesenteritis or edema and dilatation of local vessels. The dilatation of the local vessels is seen supplying a local inflamed bowel segment, akin to the “comb sign” seen on CT examination; this finding is well depicted in postcontrast gradient-echo images and steady-state free prccession images. Inclusive in the term fibrofatty proliferation is “fat wrapping,” whereby there is chronic enlarged mesenteric fat leading to increased separation of the mesenteric bowel loops. Fat proliferation is a distinguishing feature of Crohn disease and is indicative of the diagnosis. (See the image below.)
 MRI enterography, steady-state free-procession image, demonstrates vascular engorgement of the vasa recta or "comb" sign in a thickened ileum bowel loop during active disease.
MRI enterography, steady-state free-procession image, demonstrates vascular engorgement of the vasa recta or "comb" sign in a thickened ileum bowel loop during active disease.
Mesenteric edema in active disease is seen accompanying bowel wall edema and hyperenhancement and is seen often with the comb sign of the mesentery.
Active lymph nodes are enlarged, hyperenhancing, and edematous, typically along the vascular supply of affected bowel segment. The nodal enhancement is usually homogeneous and is greater than or equal to one of the adjacent lymph nodes for active disease. [30]
Low et al [39] and Marcos and Semelka [40] have found gradient-echo imaging to be more sensitive than other methods in determining the severity of Crohn disease, and they favor the use of gadolinium-enhanced gradient-echo MRI.
Gadolinium-enhanced spoiled gradient echo MRI has a reported sensitivity of 85-89%, a specificity of 96-94%, and an accuracy of 94-91% for active disease, as compared with single-shot fast spin-echo MRI, which has a sensitivity of 51-52%, specificity of 98-96%, and accuracy of 83-84%. [39]
Chronic Crohn disease and complications of Crohn disease
There are 3 major forms of chronic Crohn disease: fistula and perforating disease, fibrostenotic disease, and reparative or regenerative disease. Fistulas are sequelae of deep transmural ulcers that extend through the musculature, leading to the formation of small abscesses and sinus tracts. The sinus tract can involve and communicate with adjacent hollow organ and form fistulas. MRI depiction of fistulas is often seen as fibrotic, star-shaped reactions of the mesentery, with tethering of the adjacent communicating structures. It has avid enhancement post contrast and, on occasion, shows a linear T2-hyperintense tract. The chronic mesenteric inflammation can eventually form fibrous bands with enhancement similar to sinuses and fistulas. However, they often lead to tenting and segmental obstruction with MR fluoroscopy, showing kinking and stretching of the adjacent bowel loops.
Fibrostenotic disease is often depicted as bowel obstruction without bowel wall thickening. The bowel stricture has low T1 and T2 mural signal and has mild nonhomogeneous enhancement. With asymmetric bowel wall involvement, pseudosacculation can occur.
Regenerative disease is depicted on MRI as luminal narrowing without inflammation or obstruction. On steady-state, free-procession imaging, filiform polyposis may be suggested without enhancement or obstruction. Neoplasia is also a concern in chronic disease, since Crohn disease patients are at increased risk of developing adenocarcinoma of the affected bowel segment. [41, 42] Eccentric bowel wall thickening or shouldering, mesenteric infiltration, and lymphadenopathy on MRI enterography or enteroclysis are often early signs of malignancy.
Warning about gadolinium-based contrast agents
Gadolinium-based contrast agents have been linked to the development of nephrogenic systemic fibrosis (NSF) or nephrogenic fibrosing dermopathy (NFD). The disease has occurred in patients with moderate to end-stage renal disease after being given a gadolinium-based contrast agent to enhance MRI or MR angiography scans. [43] NSF/NFD is a debilitating and sometimes fatal disease. Characteristics include red or dark patches on the skin; burning, itching, swelling, hardening, and tightening of the skin; yellow spots on the whites of the eyes; joint stiffness with trouble moving or straightening the arms, hands, legs, or feet; pain deep in the hip bones or ribs; and muscle weakness.
Degree of confidence and impact of MRI
In a study comparing T2-weighted breath-hold single-shot fast spin-echo versus gadolinium-enhanced spoiled gradient-echo, the latter was found to better depict the extent and severity of Crohn disease. Gadolinium-enhanced spoiled GRE MR images depicted more segments of diseased bowel, and severity of Crohn disease was correctly depicted by gadolinium-enhanced spoiled GRE imaging in 93% versus only 43% by single-shot fast SE imaging. [39] A number of studies have reported that MRI for Crohn disease has a sensitivity ranging from 88 to 98% and a specificity that ranges from 78 to 100%. [20] In a retrospective study, MR enterography was confirmed to impact the management of patient care with additional information from endoscopy and clinical assessment. In 120 MRE patients, 53% underwent additional medical treatment of active disease, and 16% underwent surgery for complicated Crohn disease or medical intractability. [44]
Ultrasonography
Ultrasonography can be an alternative to CT in the evaluation of the intraluminal and extraluminal manifestations of Crohn disease. The normal GI wall appears as 5 concentric, alternating echogenic and hypoechoic layers; this appearance is known as the gut signature. The GI wall has an average thickness of less than 5 mm. [45]
In the case of active Crohn disease, the wall thickness can range from 5 mm to 2 cm with either partial or total loss of layering, which reflects transmural edema, inflammation, or fibrosis. With severe inflammation, the wall appears diffusely hypoechoic with a central hyperechoic line that corresponds to the narrowed lumen. Peristalsis is reduced or absent, and the diseased segment is noncompressible and rigid with a loss of haustra.
Ultrasonography can depict ballooning of the less involved segments, which is seen as focal sacculation or outpouching. These findings reflect the skip lesions found in Crohn disease. The accuracy of ultrasonography is further improved with the use of color Doppler imaging. The use of Doppler imaging is helpful in the detection of hyperemia of an inflamed bowel wall and adjacent fat during active disease.
With transmural inflammation, edema and fibrosis of the adjacent mesentery occurs, leading to fingerlike projections of mesenteric fat that creeps over the serosal surface of the bowel. This creeping fat eventually envelops the diseased bowel segment. On sonograms, this appears as a uniform hyperechoic mass, which is classically seen at the cephalic margin of the terminal ileum. With long-standing disease, this becomes more heterogeneous or even hypoechoic.
In active Crohn disease, reactive mesenteric nodes are enlarged and may coalesce to form a conglomerate mass. On sonograms, enlarged nodes can be seen as oval hypoechoic masses in the mesentery. With confluence, they become lobulated masses of various sizes.
Many complications of Crohn disease can also be seen in their ultrasonographic forms. Phlegmon appears as a hypoechoic mass with irregular borders and no identifiable wall or fluid. Abscess appears as a fluid collection with a thickened wall containing air or echogenic debris. Obstruction appears as dilated hyperperistaltic fluid filled segments. Perforation appears as bright echoes with distal acoustic shadows outside the boundaries of bowel loops.
A fistula, on the other hand, appears as a hypoechoic tract. If gas is present in the fistulous tract, it contains hyperechoic foci with acoustic shadowing. Palpation of diseased loops during sonography enables tract identification. In addition, sonography should be able to identify gas bubbles in abnormal locations, such as air in the bladder or vaginal vault, the retroperitoneum, the subcutaneous tissue, and the urachal remnant.
The detection of bowel wall thickening varies widely. Detection rates range from 22 to 89%. The large variation presumably reflects differences in technique, operator experience, and ultrasound equipment. Determination of the extent of the disease is not always possible, and correlation between wall thickening and the clinical activity of disease is poor.
The loss of gut signature and bowel wall thickening is a nonspecific finding. It is found in infectious, ischemic, neoplastic, and radiation-induced conditions. In addition, the detection of bowel wall changes in Crohn disease varies significantly because of operator dependence.
(See the images below.)
Crohn disease of the terminal ileum with CT and sonographic correlation. Note terminal ileal-wall thickening and adjacent mesenteric inflammatory stranding.
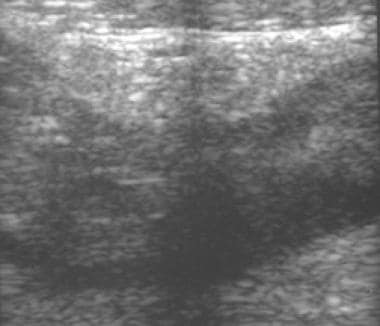 Crohn disease of the terminal ileum with CT and sonographic correlation. Note hypoechoic wall thickening, loss of the gut signature, and the hyperechoic line representing the narrowed lumen.
Crohn disease of the terminal ileum with CT and sonographic correlation. Note hypoechoic wall thickening, loss of the gut signature, and the hyperechoic line representing the narrowed lumen.
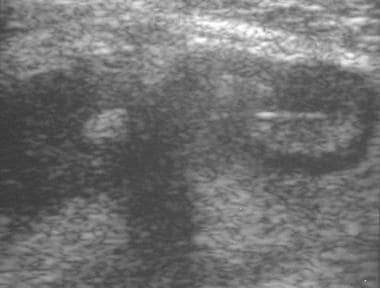 Crohn disease of the terminal ileum with CT and sonographic correlation. Note hypoechoic wall thickening, loss of the gut signature, and the hyperechoic line representing the narrowed lumen.
Crohn disease of the terminal ileum with CT and sonographic correlation. Note hypoechoic wall thickening, loss of the gut signature, and the hyperechoic line representing the narrowed lumen.
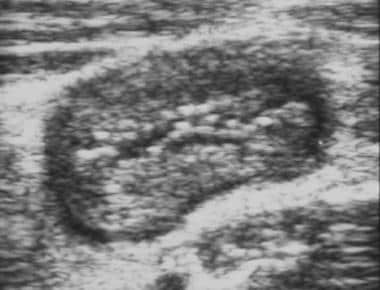 Crohn disease. Sonogram of a thickened bowel wall demonstrates the so-called pseudokidney appearance.
Crohn disease. Sonogram of a thickened bowel wall demonstrates the so-called pseudokidney appearance.
The literature states that the differentiation between hypoechoic foci from creeping fat and that from phlegmon or edema may be difficult or nearly impossible. Proponents of CT have also stated that the specificity of color Doppler imaging is still unknown. In general, the confidence level of the radiologist in interpreting the results is operator dependent, and it is often lower than that for CT. For these reasons, ultrasonography has not been the favored modality for imaging Crohn disease.
Nuclear Imaging
There is a limited role for scintigraphy in disease surveillance after the diagnosis of CD has been established.
Scintigraphic examinations include technetium-99m hexamethyl propylene amine oxime-labeled white blood cell scan (99mTc-HMPAO WBC) and fluorine-18-2-fluoro-2-deoxy-D-glucose positron emission tomography (FDG/PET) CT. 99mTc-HMPAO WBC has demonstrated good sensitivity and specificity for intestinal inflammation. However, the disadvantages of this examination, such as the decreased ability to depict and therefore detect alternative diagnoses and the complicated and time-consuming technical aspects, have limited its use in initial diagnosis. [2, 7, 14, 46, 47, 48]
Leukocyte scintigraphy is well tolerated and noninvasive and potentially permits assessment of the presence, extent, and activity of inflammation, but it is limited by radiation exposure and lower sensitivity, especially in patients undergoing steroid treatment. [2] Leukocytes labeled with either indium-111 (111In) or 99mTc-HMPAO can be used to assess for active bowel inflammation in inflammatory bowel disease. Compared to 111In, 99mTc- HMPAO has better imaging characteristics and can be imaged much sooner after injection. However, imaging must typically be done within an hour after injection of 99mTc-HMPAO-labeled leukocytes, as there is normal excretion into the bowel after this time, unlike with 111In-labeled leukocytes, which have no normal bowel excretion. [2, 7, 14, 46, 47, 48]
-
Crohn disease. Aphthous ulcers. Double-contrast barium enema examination in Crohn colitis demonstrates numerous aphthous ulcers.
-
Crohn disease. Cobblestoning. Spot view of the terminal ileum from a small-bowel follow-through study demonstrates linear longitudinal and transverse ulcerations that create a cobblestone appearance. Also note the relatively greater involvement of the mesenteric side of the terminal ileum and the displacement of the involved loop away from the normal small bowel secondary to mesenteric inflammation and fibrofatty proliferation.
-
Crohn disease. Spot view of the terminal ileum from a small-bowel follow-through study demonstrates several narrowing and stricturing, consistent with the string sign. Also note a sinus tract originating from the medial wall of the terminal ileum and the involvement of the medial wall of the cecum.
-
Crohn disease of the terminal ileum with CT and sonographic correlation. Small-bowel follow-through study demonstrates the string sign in the terminal ileum. Also note pseudodiverticula of the antimesenteric wall of the terminal ileum, secondary to greater distensibility of this less-involved segment of the wall.
-
Crohn disease of the terminal ileum with CT and sonographic correlation. Note terminal ileal-wall thickening and adjacent mesenteric inflammatory stranding.
-
Crohn disease of the terminal ileum with CT and sonographic correlation. Note hypoechoic wall thickening, loss of the gut signature, and the hyperechoic line representing the narrowed lumen.
-
Crohn disease of the terminal ileum with CT and sonographic correlation. Note hypoechoic wall thickening, loss of the gut signature, and the hyperechoic line representing the narrowed lumen.
-
Crohn disease. Active small-bowel inflammation. CT scan demonstrates small-bowel wall thickening, mesenteric inflammatory stranding, and mesenteric adenopathy.
-
Crohn disease. Mesenteric inflammation. CT scan demonstrates inflammatory mass in the right lower quadrant associated with thickening of the wall and narrowing of the lumen of the terminal ileum.
-
Crohn disease. Mesenteric inflammation. CT scan demonstrates an inflammatory mass in the right lower quadrant associated with thickening of the wall and narrowing of the lumen of the terminal ileum.
-
Crohn disease. Sonogram of a thickened bowel wall demonstrates the so-called pseudokidney appearance.
-
Crohn disease. Crohn colitis. Double-contrast barium enema study demonstrates marked ulceration, inflammatory changes, and narrowing of the right colon.
-
Crohn disease. Crohn colitis. CT scan demonstrates marked thickening of the wall of the right colon with inflammatory stranding in the adjacent mesenteric fat.
-
Crohn disease. Fibrofatty proliferation. CT scan in a patient with Crohn colitis in the chronic phase demonstrates wall thickening of the right colon, an absence of adjacent mesenteric inflammatory stranding, and a large amount of fatty proliferation around the right colon separating the colon from the remainder of the gut, so-called creeping fat.
-
Crohn disease. Single-contrast barium enema study demonstrates stricturing of the caput cecum, the so-called coned cecum.
-
Crohn disease. Coned cecum. CT scan demonstrates wall thickening of the cecum with marked narrowing of the lumen.
-
Crohn disease. CT with MRI correlation. CT scan in a patient with chronic inactive Crohn disease demonstrates thickening of the wall of the right colon with intramural lucency. This was believed to represent intramural fat deposition.
-
Crohn disease. MRI with CT correlation. MRI demonstrates thickening of the wall of the right colon with intramural increased signal on a T1-weighted image. This was believed to represent intramural fat deposition.
-
Crohn disease. Perianal abscesses. CT scan demonstrates multiple fluid, contrast material, and air collections around the anorectum. Note the presence of a rectal tube.
-
Crohn disease. Perianal abscesses. CT scan demonstrates multiple fluid, contrast agent, and air collections around the anorectum. Note the presence of a rectal tube.
-
Crohn disease. Small-bowel obstruction in a patient with recurrence proximal to an anastomosis. CT scan in a patient with a prior ileocolectomy demonstrates small-bowel dilatation and wall thickening of the small bowel proximal to the anastomosis.
-
Crohn disease. Small-bowel obstruction in a patient with recurrence proximal to an anastomosis. CT scan demonstrates small-bowel dilatation and a transition zone at the anastomosis. Note the narrowed segment of bowel at the staple line in the right lower quadrant.
-
Crohn disease. Small-bowel obstruction in a patient with recurrence proximal to an anastomosis. Small-bowel follow-through demonstrates mucosal changes of Crohn disease in the distal ileum proximal to the anastomosis and anastomotic stricture.
-
Crohn disease. Enteroenteric fistula. CT scan demonstrates the tract of an enteroenteric fistula.
-
Crohn disease. Enterocutaneous fistula. CT scan demonstrates enterocutaneous and colocutaneous fistula formation.
-
Crohn disease. Enterocolic fistula. Double-contrast barium enema study demonstrates multiple fistulous tracts between the terminal ileum and the right colon adjacent to the ileocecal valve, the so-called double-tracking of the ileocecal valve.
-
Crohn disease. Small-bowel follow-through study demonstrates narrowing of the lumen and multiple enteroenteric fistulae, but it fails to show the enterovesical fistula.
-
Crohn disease. Cystogram demonstrates a filling defect and inflammatory changes of the dome of the bladder, but it fails to demonstrate the enterovesical fistula.
-
Crohn disease. Enterovesical fistula. CT demonstrates an air-filled fistulous tract from the small bowel to the bladder.
-
Crohn disease. Enterovesical fistula. CT demonstrates focal thickening of the bladder dome and air in the urinary bladder.
-
MRI enterography coronal single-shot fast spin-echo images in a patient with active Crohn disease demonstrates wall thickening and wall deep fissuring along an ascending limb of the distal ileum small bowel loop in the right lower quadrant of the abdomen.
-
MRI enterography with coronal fat-saturated T2-weighted single-shot fast spin echo imaging demonstrates mesenteric edema and mural wall edema and thickening in a patient with active Crohn disease in the distal ileum.
-
MRI enterography 3-dimensional gradient postcontrast series demonstrates stratified hyperenhancement of the mucosa of the distal ileum in a patient with active Crohn disease.
-
MRI enterography, steady-state free-procession image, demonstrates vascular engorgement of the vasa recta or "comb" sign in a thickened ileum bowel loop during active disease.







