Practice Essentials
Pseudomembranous colitis (PMC; also knows as antibiotic-associated colitis or Clostridium difficile colitis) is a descriptive term for colitides defined by the presence of pseudomembranes on the colonic or small intestinal mucosa. [1] A pseudomembrane is a layer of fibropurulent exudate that is omposed of acute inflammatory cells and mucus originating from inflamed and erupting crypts. [2] Although small intestine can be involved in PMC, most cases encountered in the modern era involve only the colon. Clostridium difficile infection is responsible for virtually all cases of PMC and for as many as 20% of cases of antibiotic-induced diarrhea without colitis. [3]
The etiology of antibiotic-associated diarrhea and colitis not caused by C difficile is poorly understood, and a variety of other organisms have been implicated as causative agents, including Staphylococcus aureus, Candida species, Clostridium perfringens, and Salmonella. [4]
Pseudomembranous lesions in the intestinal tract, originally reported in 1893, were thought to be caused by S aureus on the basis of its recovery in the stool samples of affected patients. With time, S enterocolitis (involving both small intestine and colon) became an accepted entity. Widespread antibiotic use made PMC a common problem, and it became apparent that the disease primarily involved the colon and only rarely involved the small intestine. In 1977, C difficile was recognized as the pathogen responsible for the development of PMC.
The risk factors for PMC in patients with hospital-acquired diarrhea (HAD) may include cephalosporin use, proton pump inhibitor use, old age (≥70 yr), and cancer. The prevalence of PMC may be very low in patients with HAD without such risk factors. [5]
Radiologic examination
Radiographic studies can aid in the diagnosis of C difficile infection. Plain radiography may reveal colonic ileus, small bowel ileus, ascites, nodular thickening, or thumbprinting (wide transverse bands associated with haustral thickening). Severe disease may show marked colonic dilatation, perforation, or pneumoperitoneum. CT is more commonly used because of its higher sensitivity. CT findings may include colonic wall thickening and nodularity, bowel wall stranding and edema, ascites, the accordion sign (ingested oral contrast becomes trapped between thickened haustral folds), and the double-halo sign (ie, submucosal edema indicated by 2 or 3 concentric rings in the large bowel on transverse imaging). [6, 7, 8, 9, 10]
(See the images of pseudomembranous colitis below.)
 Gross pathology specimen from a case of pseudomembranous colitis revealing characteristic yellowish plaques.
Gross pathology specimen from a case of pseudomembranous colitis revealing characteristic yellowish plaques.
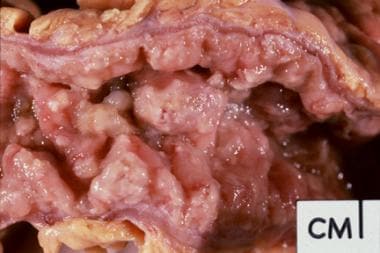 Gross pathology specimen from a case of pseudomembranous colitis demonstrating characteristic yellowish plaques.
Gross pathology specimen from a case of pseudomembranous colitis demonstrating characteristic yellowish plaques.
 Frontal abdominal radiograph in a patient with proved pseudomembranous colitis. Note the nodular haustral thickening, most pronounced in the transverse colon.
Frontal abdominal radiograph in a patient with proved pseudomembranous colitis. Note the nodular haustral thickening, most pronounced in the transverse colon.
 Barium enema demonstrating typical serrated appearance of the barium column resulting from trapped barium between the edematous mucosal folds and the plaquelike membranes in pseudomembranous colitis.
Barium enema demonstrating typical serrated appearance of the barium column resulting from trapped barium between the edematous mucosal folds and the plaquelike membranes in pseudomembranous colitis.
 CT findings in a proved case of pseudomembranous colitis demonstrating wall thickening of the transverse colon.
CT findings in a proved case of pseudomembranous colitis demonstrating wall thickening of the transverse colon.
 CT scan in a patient with pseudomembranous colitis demonstrating the classic accordion sign.
CT scan in a patient with pseudomembranous colitis demonstrating the classic accordion sign.
Imaging in differential diagnosis
Infection with toxigenic C difficile causes a spectrum of diseases ranging from the asymptomatic carrier state, particularly in neonates, to a fulminant relapsing and occasionally fatal colitis. [4] The typical clinical presentation is diarrhea, abdominal pain, fever, leukocytosis, and an often-overlooked history of recent/concurrent use of antibiotics. Hospital inpatients may be asymptomatic or may only have mild-to-moderate symptoms. [11] In severe cases, life-threatening colitis may develop, progressing to toxic megacolon and subsequent perforation.
The American College of Radiology (ACR) recommends abdominal CT scanning as the imaging modality of choice for C difficile colitis when pseudomembranous colitis or other complications of C difficile infection are suspected. [12]
In rare cases, extraintestinal manifestations occur, including bacteremia, osteomyelitis, and splenic abscess. Other clinical manifestations that have been described are reactive arthritis and tenosynovitis. As with other reactive arthritides following enteric infections, many patients are positive for human leukocyte antigen (HLA)-B27. [4] Nonspecific symptomatology of PMC mimics features of acute abdomen, especially sepsis or intra-abdominal infection and abscess.
Most of these patients undergo ultrasonographic or computed tomography (CT) scans without clinical suspicion of PMC. [1] Thus, it is important for radiologists to recognize the radiologic features of PMC, since the radiologist is often the first physician to suggest the diagnosis.
It is important to note that even though the diagnosis of PMC may be suggested by imaging, it is not the method of choice for establishing the diagnosis. This is done by stool assays for C difficile toxins or colonoscopy.
Valiquette et al, in a study of abdominal CT in patients with the BI/NAP1/027 hypervirulent strain of C difficile, found that CT could provide prognostic information additional to what could be obtained by clinical and laboratory parameters. They also found that patients who underwent CT were younger, had higher peak white blood cell counts and serum creatinine levels, and were more likely to experience fever than those who did not undergo CT. However, there were no differences in CT findings before and after emergence of BI/NAP1/027. The authors noted that pleural effusion, colonic wall thickness greater than 15 mm, a peak white blood cell count of ≥30 x 109 cells/L, an albumin level less than 20 g/L, and immunosuppression were independently associated with complicated C difficile infection. [13]
In patients with C difficile colitis on broad-spectrum antibiotic therapy, CT findings of colonic wall thickening (0.5 -1.6 cm), a mild degree of pericolonic fat stranding, and the accordion sign may be detected. In one study of 15 patients, 11 (73.3%) had pancolonic wall thickening, 4 (26.6%) had segmental involvement, and 11 (73.3%) displayed the accordion sign. [14]
Radiography
Plain films of the abdomen are notoriously insensitive for the diagnosis of PMC; plain radiographic abnormalities are observed in perhaps only 32% of cases of the disease. [15] Even when radiographs demonstrate abnormalities, they tend to underestimate the extent and severity of PMC, with findings on plain films ranging from normal to nonspecific. [11] However, because these films are often the first studies to be ordered, it is important to be aware of these findings. Classic findings consist of the following:
-
Colonic dilatation
-
Nodular haustral thickening
-
Thumb printing
Findings range from colonic ileus to toxic megacolon and even perforation with pneumoperitoneum. Toxic megacolon is suggested by acute dilatation of transverse colon to a diameter greater than 6 cm associated with systemic toxicity and the absence of mechanical obstruction.
Nodular haustral thickening is considered to be fairly specific for PMC but is observed only in severe cases. [1] Any part of the colon may be involved. In a study by Boland et al, the transverse colon was most commonly involved, followed by the left colon and then the right colon. [15] (See the image below.)
Frontal abdominal radiograph in a patient with proved pseudomembranous colitis. Note the nodular haustral thickening, most pronounced in the transverse colon.
Thumb printing is nonspecific, since it can be observed with either inflammatory or ischemic colitis.
Contrast enemas should be avoided in patients with possible PMC because of potential risk for perforation. Barium enemas are rarely indicated, especially with the advent of cross-sectional imaging.
Barium enema findings may vary, depending on the severity of the disease. In the milder forms, nodular filling defects involving the mucosa may be observed that coalesce as the disease progresses, giving an irregular appearance to the bowel wall. The serrated outline of the colon does not result from mucosal ulceration but, rather, is a consequence of trapped barium between the plaquelike membranes. (See the image below.)
Barium enema demonstrating typical serrated appearance of the barium column resulting from trapped barium between the edematous mucosal folds and the plaquelike membranes in pseudomembranous colitis.
Computed Tomography
With increased use of CT scanning as a primary imaging modality in the evaluation of patients with diffuse abdominal pain or fever, it is critical for radiologists to recognize CT scan features of PMC. CT scan findings, although not specific, may be highly suggestive of PMC, and CT scanning is excellent for evaluation of the extent of PMC. [1, 16, 14, 17] The sensitivity of detection of PMC on CT is approximately 85%. Specificity of CT is low (approximately 48%), since other types of colitis can cause a similar appearance. [18] Pneumatosis, toxic megacolon, and portal venous gas may be observed. These features are nonspecific and may be observed with severe colitis of any cause.
The following are CT scan findings in PMC:
-
Marked colonic wall thickening
-
Target sign
-
Accordion sign
-
Pericolonic stranding
-
Ascites
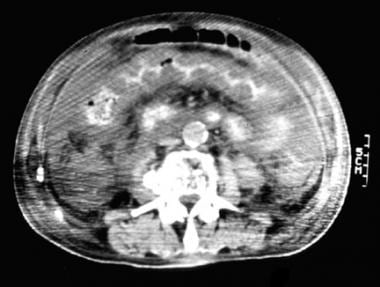
Colonic wall thickening is the most common CT finding in patients with PMC and ranges from 3-32 mm. [11] Most cases reveal total colonic involvement; however, focal and segmental involvement has been well documented. Mural thickening can be smooth or irregular and eccentric or concentric. PMC more often causes irregular and shaggy wall thickening rather than the smooth and homogeneous thickening observed with Crohn disease. (See the image below.)
CT findings in a proved case of pseudomembranous colitis demonstrating wall thickening of the transverse colon.
On contrast-enhanced CT, mucosal hyperemia leads to enhancement with relatively hypodense submucosa secondary to edematous changes. This gives the appearance of a bull's eye or target sign. The sign is better appreciated on the arterial phase of enhancement. It is a nonspecific sign and has been reported with other forms of colitis such as Crohn disease and ulcerative colitis.
The accordion sign is highly suggestive of PMC but is only observed in advanced disease. The cause of this sign is entrapment of orally administered barium in between thick and edematous haustral folds, giving alternating low- and high-density bands. (See the image below.)
CT scan in a patient with pseudomembranous colitis demonstrating the classic accordion sign.
Pericolonic stranding, if observed, is usually mild, reflecting mucosal, rather than serosal, involvement. The typical CT appearance of PMC is mild pericolonic stranding disproportionate to marked colonic wall thickening.
Ascites is a nonspecific finding and tends to occur in severe cases of PMC. Ascites is observed on CT in an average of 35% of patients. [1]
Ultrasonography
Ultrasonography is not commonly used for evaluation of possible PMC; however, it may be helpful in evaluation of postoperative patients in surgical intensive care units who are on antibiotics and develop nonspecific abdominal symptoms. [1]
Ultrasonographic findings rely on wall thickening of the colon, as well as on the target sign, demonstrated by hyperechoic mucosa in the background of hypoechoic edematous submucosa. Ascites may be an associated finding and has been observed in as many as 77% of cases. [19]
Thickened colon may be discovered incidentally during ultrasonographic examination of the abdomen.
-
Gross pathology specimen from a case of pseudomembranous colitis revealing characteristic yellowish plaques.
-
Gross pathology specimen from a case of pseudomembranous colitis demonstrating characteristic yellowish plaques.
-
Frontal abdominal radiograph in a patient with proved pseudomembranous colitis. Note the nodular haustral thickening, most pronounced in the transverse colon.
-
Barium enema demonstrating typical serrated appearance of the barium column resulting from trapped barium between the edematous mucosal folds and the plaquelike membranes in pseudomembranous colitis.
-
CT findings in a proved case of pseudomembranous colitis demonstrating wall thickening of the transverse colon.
-
CT scan in a patient with pseudomembranous colitis demonstrating the classic accordion sign.





