Practice Essentials
Clubfoot, or talipes equinovarus, is a congenital deformity consisting of hindfoot equinus, hindfoot varus, and forefoot varus. The deformity was described as early as the time of Hippocrates. The term talipes is derived from a contraction of the Latin words for ankle, talus, and foot, pes. The term refers to the gait of severely affected patients, who walked on their ankles. [1, 2] Although most clubfeet are idiopathic, it can be secondary or syndromic when its presentation is associated with another congenital disease (20% of cases). Some studies have focused on the interaction between genetics and environmental factors, showing a multifactorial etiology of the disease. [3] [4, 5]
Clubfoot is one of the most common congenital limb deformities. Epidemiological studies suggest a birth prevalence in the range of 1 to 3 cases per 1000 live births, [4] resulting in an annual estimated 7 to 43 new cases of clubfoot per million population, depending mainly on the birth rate. The higher prevalence seems to be associated with social-demographic, genetic, and environmental risk factors, which explain its prevalence among low- and middle-income countries. It affects males more than females, with a male-to-female ratio of 2:1. [6]
(See the images below.)
 Lateral view in talipes equinovarus demonstrates an abnormally elevated tibiocalcaneal angle. A normal angle is 60-90°.
Lateral view in talipes equinovarus demonstrates an abnormally elevated tibiocalcaneal angle. A normal angle is 60-90°.
 Dorsoplantar views obtained in a patient with unilateral clubfoot show that the talus and calcaneus are more overlapped than in the normal condition. The talocalcaneal angle is 15° or less. Note that the line through the long axis of the talus passes lateral to the first metatarsal due to the varus position of the forefoot.
Dorsoplantar views obtained in a patient with unilateral clubfoot show that the talus and calcaneus are more overlapped than in the normal condition. The talocalcaneal angle is 15° or less. Note that the line through the long axis of the talus passes lateral to the first metatarsal due to the varus position of the forefoot.
Preferred examination
The standard radiologic method of postnatal evaluation is plain radiography. The equipment required is inexpensive and readily available. Evaluation should include the acquisition of only weight-bearing images because the stress involved is reproducible. In infants, weight bearing can be simulated with the application of dorsal flexion stress. The standard views are the dorsoplantar (DP) and lateral views. For the DP view, the beam is angled 15° toward the heel to prevent overlap of the structures of the lower leg. The lateral view should include the ankle, and not the foot, for proper depiction of the talus. Other methods of imaging are not routinely used in the evaluation of clubfoot, and experience with these is limited. [7, 8, 9, 10]
Plain radiography has the disadvantage of exposing the patient to ionizing radiation. Additionally, proper positioning can be difficult. Improper positioning can simulate deformities. Further, because clubfoot is a congenital condition, the lack of ossification in some of the involved bones is another limitation. In neonates, only the talus and calcaneus are ossified. The navicular does not ossify until the child is aged 2-3 years.
While clubfoot has been diagnosed on ultrasonography prenatally as early as 13 weeks, it is more likely to be diagnosed between the 18th and 24th weeks of pregnancy. Up to 85% of diagnoses are made on ultrasound between weeks 12 and 23 of gestation, and 70-75% of isolated cases are confirmed at delivery. Alternative imaging is not indicated prenatally. There is no consensus regarding whether to propose fetal karyotyping when isolated clubfoot is diagnosed by prenatal ultrasonography. [11]
The accuracy of ultrasonography is dependent on many factors, such as experience of the physician, gestational age, the quality of equipment and the methodology used. A diagnosis of congenital clubfoot cannot be made in the first trimester of pregnancy because a transient clubfoot position is present during the normal development of the lower limbs. [12] Scans performed between the 20th and 24th week of pregnancy have been found to be the most reliable to confirm or exclude a diagnosis of clubfoot. [11] Prenatal ultrasound diagnosis of clubfoot has been reported to be more accurate in singletons than in twins. [13, 14] The rates of false-positive prenatal diagnosis vary widely from 0 to 40% in isolated clubfoot, with a smaller (< 10%) false-positive rate when prenatal diagnosis is made in specialized centers with a targeted anatomic ultrasound survey. [11]
Radiography
The 3 main components of the deformity are evident on radiographs and can be reproducibly quantified. With proper positioning and exposure, quantification of alignment abnormalities on plain radiographs is reliable. No confirmatory imaging is routinely used. Oblique positioning of the heel on the DP view can simulate hindfoot varus. If the lateral view is one of the foot rather than the ankle, the flat talar dome has a spurious appearance. [15]
Hindfoot equinus is plantar flexion of the anterior calcaneus (similar to a horse's hoof) such that the angle between the long axis of the tibia and the long axis of the calcaneus (tibiocalcaneal angle) is greater than 90° (see the image below).
Lateral view in talipes equinovarus demonstrates an abnormally elevated tibiocalcaneal angle. A normal angle is 60-90°.
In hindfoot varus, the talus is assumed to be fixed relative to the tibia. The calcaneus is considered to rotate around the talus into a varus (toward midline) position. On the lateral view, the angle between the long axis of the talus and the long axis of the calcaneus (talocalcaneal angle) is less than 25°, and the 2 bones are more nearly parallel than in the normal condition (see the images below).
 Normal lateral view shows the measurement of the talocalcaneal angle. The calcaneal long axis is drawn along the plantar surface. The normal range is 25-45°. Note the normal overlap of the metatarsals on the lateral view.
Normal lateral view shows the measurement of the talocalcaneal angle. The calcaneal long axis is drawn along the plantar surface. The normal range is 25-45°. Note the normal overlap of the metatarsals on the lateral view.
 Lateral view of clubfoot shows the nearly parallel talus and calcaneus, with a talocalcaneal angle of less than 25°.
Lateral view of clubfoot shows the nearly parallel talus and calcaneus, with a talocalcaneal angle of less than 25°.
On the DP view, the talocalcaneal angle is less than 15°, and the 2 bones appear to overlap more than normal. Also, the longitudinal axis through the middle of the talus (midtalar line) passes lateral to the base of the first metatarsal, because the forefoot is medially deviated (see the images below).
 Dorsoplantar projection of a healthy foot shows that the line through the long axis of the talus passes just medial to the base of the first metatarsal. The talocalcaneal angle measurement is shown. The normal range is 15-40°.
Dorsoplantar views obtained in a patient with unilateral clubfoot show that the talus and calcaneus are more overlapped than in the normal condition. The talocalcaneal angle is 15° or less. Note that the line through the long axis of the talus passes lateral to the first metatarsal due to the varus position of the forefoot.
Dorsoplantar projection of a healthy foot shows that the line through the long axis of the talus passes just medial to the base of the first metatarsal. The talocalcaneal angle measurement is shown. The normal range is 15-40°.
Dorsoplantar views obtained in a patient with unilateral clubfoot show that the talus and calcaneus are more overlapped than in the normal condition. The talocalcaneal angle is 15° or less. Note that the line through the long axis of the talus passes lateral to the first metatarsal due to the varus position of the forefoot.
Forefoot varus and supination increase the convergence of the bases of the metatarsals on the DP view, compared with the normal slight convergence (see the image below).
 Dorsoplantar view of talipes equinovarus shows that the convergence of the bases of the metatarsals is abnormally increased compared with the normal convergence.
Dorsoplantar view of talipes equinovarus shows that the convergence of the bases of the metatarsals is abnormally increased compared with the normal convergence.
On the lateral view, instead of having the normal overlapped appearance, the metatarsals are arranged in a ladderlike configuration, with the first being most dorsal (see the image below).
 Lateral view of shows the ladderlike configuration of the metatarsals in forefoot varus in clubfoot.
Lateral view of shows the ladderlike configuration of the metatarsals in forefoot varus in clubfoot.
The following table contains a summary of the normal and clubfoot measurements.
Table. A Summary of the Normal and Clubfoot Measurements (Open Table in a new window)
Measurement |
Normal Foot |
Clubfoot |
Tibiocalcaneal angle |
60-90° on lateral view |
>90° (hindfoot equinus) on lateral view |
Talocalcaneal angle |
25-45° on lateral view, 15-40° on DP view |
< 25° (hindfoot varus) on lateral view, < 15° (hindfoot varus) on DP view |
Metatarsal convergence |
Slight on lateral view, slight on DP view |
None (forefoot supination) on lateral view, increased (forefoot supination) on DP view |
In an incompletely corrected or recurrent clubfoot, characteristic abnormalities are observed. [16] The talocalcaneal angle is normal on the DP view (see the image below), but talocalcaneal parallelism persists on the lateral view.
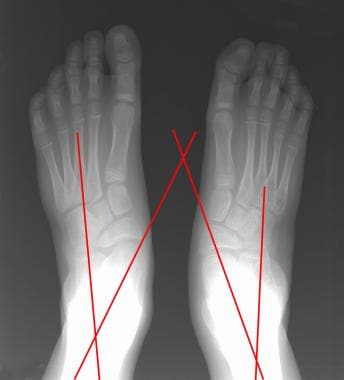 Image of clubfoot obtained after repair shows restoration of a normal talocalcaneal angle on the dorsoplantar view. The line along the long axis of the talus now passes medial to the first metatarsal; this finding indicates overcorrection of the forefoot varus.
Image of clubfoot obtained after repair shows restoration of a normal talocalcaneal angle on the dorsoplantar view. The line along the long axis of the talus now passes medial to the first metatarsal; this finding indicates overcorrection of the forefoot varus.
Flattening of the talar dome persists on this view as well (see the image below).
 Postoperative lateral view of a clubfoot shows persistent parallelism of the talus and calcaneus. Note the characteristic flattening of the talar dome on this true lateral view of the ankle.
Postoperative lateral view of a clubfoot shows persistent parallelism of the talus and calcaneus. Note the characteristic flattening of the talar dome on this true lateral view of the ankle.
Cavus of the plantar arch may be present, particularly if no plantar release was performed. Also, a periosteal reaction, sclerosis, or fracture of the lateral metatarsals may occur as a result of abnormal weight bearing on this side of the foot in cases of inadequate correction of forefoot varus (see the images below).
 Lateral radiographs obtained in a 12-year-old girl after surgical clubfoot repair shows persistent forefoot varus and resultant stress changes (cortical thickening) in the most lateral metatarsals.
Lateral radiographs obtained in a 12-year-old girl after surgical clubfoot repair shows persistent forefoot varus and resultant stress changes (cortical thickening) in the most lateral metatarsals.
 DP radiographs obtained in the same girl as in the previous image after surgical clubfoot repair shows persistent forefoot varus and resultant stress changes to the lateral metatarsals.
DP radiographs obtained in the same girl as in the previous image after surgical clubfoot repair shows persistent forefoot varus and resultant stress changes to the lateral metatarsals.
Tarraf and Carroll found that residual forefoot adduction and supination were, by far, the most common deformities that lead to repeat surgery for clubfoot. In addition to hindfoot alignment, these deformities should be actively evaluated on intraoperative radiographs. [17]
Computed Tomography
There are limited studies regarding the use of CT in the evaluation of clubfoot. Disadvantages of CT include the risk of ionizing radiation, the lack of ossification of the tarsal bones, susceptibility of the images to motion artifact, and the need for expensive equipment and software applications for multiplanar reconstruction. On the other hand, this complex 3-dimensional deformity may ultimately be better assessed with 3-dimensional reconstructions than with 2-dimensional radiographs. The utility of CT in the evaluation of talar articulations in trauma and tarsal coalition is already well established.
In preliminary study of CT with 3-dimensional reconstructions, Johnston et al showed that wire-frame surface renderings of the bones in clubfoot can be created and that the axes of inertia can be computed around the center of mass in 3 perpendicular planes for each bone involved. [18] These renderings can be manually rotated to elucidate deformities and misalignments that are obscured because of overlap on plain radiographs. The relationship between the hindfoot bones and ankle mortise can be evaluated in this way, because the information from the lower leg does not overlap. Similarly, the vertical axes of the talus and calcaneus can be compared with a reference line perpendicular to the floor in a coronal reconstruction of the heel. This view can be obtained only with CT.
These analyses by Johnston et al revealed that, in the normal foot, both the talus and the calcaneus are medially rotated relative to a line perpendicular to the mortise in the transverse plane, but the rotation in the calcaneus is much less. This difference is the normal divergence of the long axes of the 2 bones. In the clubfoot, the talus is laterally rotated, and the calcaneus is more medially rotated than normal; these rotations cause convergence of the long axes. Additionally, the authors observed mild pronation of the talus and calcaneus in the coronal plane in the clubfoot, in contrast to mild supination of both in the normal foot. These findings imply that surgical correction should involve supination and medial rotation of the talus in the mortise and supination and lateral rotation of the calcaneus.
Magnetic Resonance Imaging
There is limited experience in the use of MRI for imaging clubfoot. The use of MRI is limited because of its multiple disadvantages, including the need for equipment and patient sedation, the software-related expenses, the loss of signal caused by the ferromagnetic effects of fixation devices, and the additional time required for data transfer and postprocessing. On the other hand, the advantages of MRI compared with plain radiography and CT are its multiplanar imaging capability and its excellent depiction of ossific nuclei, cartilaginous anlage, and surrounding soft-tissue structures. [8, 19]
Results of a pilot study of MRI and of preliminary work in magnetic resonance multiplanar reconstructions have shown that these methods can be used to elucidate the complex pathoanatomy of this disorder. Intermediate- and T2-weighted spin-echo images are most useful for depicting the cartilaginous anlage and the articular surfaces, respectively. [20] When 3-dimensional gradient-echo acquisitions are used to create multiplanar reconstructions, the center of mass and the principal axes of inertia of each bone or cartilaginous structure can be determined. These axes can be compared with each other or a standard of reference to obtain reproducible, objective measurements of the deformities. [21, 22]
The talar deformity, which many researchers believe is primary in clubfoot, is not precisely defined by using any other imaging modality. However, with the method described above, MRI with multiplanar reconstructions can depict the intraosseous deformity of the talus defined by the elevated talar body-neck angle.
Particularly well defined is the talonavicular relationship, which is not seen on radiographs obtained in young children because of the lack of ossification in the navicular. In most patients, the navicular is medially dislocated. [23]
Ultrasonography
Clubfoot has been diagnosed on ultrasonography prenatally as early as 13 weeks, but it is more likely to be diagnosed between the 18th and 24th weeks of pregnancy. Up to 85% of cases are diagnosed by week 23 of gestation. [11, 4]
Few studies of the ultrasonographic findings in normal feet or clubfeet have been performed, and the clinical utility of this modality has yet to be established. The main disadvantage of ultrasonography is the inability of the beam to penetrate all of the bones, particularly if a postoperative scar is present. Advantages of ultrasonography include the lack of ionizing radiation, no need for sedation, its ability to depict nonossified portions of bones, and its capacity for dynamic imaging. [24, 15, 9, 10]
Preliminary studies have shown that reproducible views and objective assessments of some of the interosseus relationships in normal feet and clubfeet can be obtained with ultrasonography. In the future, these may assist in directing surgical and conservative therapies for clubfoot and in assessing the results. [25]
A 7.5-MHz linear transducer and stand-off pad are used to obtain several reproducible and helpful views. The posterior-sagittal view is obtained with the transducer aligned with the midline sagittal plane and placed on the posterior and upper part of the heel. The anteromedial view is obtained from that position at the junction of the ankle and foot, with the foot plantar flexed. The transducer is aligned along the distal tibia, talus, and navicular. The medial transverse view is transverse to the foot on its medial side. A lateral transverse view of the foot may also be useful. Furthermore, these views can be obtained through a dynamic range of motion.
The Achilles tendon can be measured on the posterior-sagittal view. It is often shortened in clubfoot and spastic deformities. On this view, the distal tibia, talus, and calcaneus are perfectly aligned. The distance between the distal ossified tibia and the superior ossified calcaneus can be measured. With plantar flexion, this distance decreases in the normal foot but not in clubfoot. This view permits evaluation of the talonavicular relationship in the DP plane, which is often persistently abnormal after complete subtalar release.
On the anterior-medial view, the medial malleolus, talus, navicular, and medial cuneiform can be seen (see the image below).
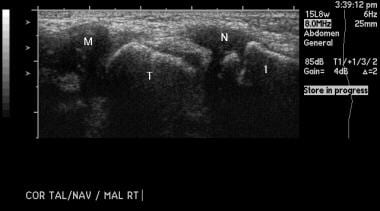 Clubfoot. Sonogram of the medial aspect of a normal foot illustrates the relationships between the cartilaginous medial malleolus (M), ossified talus (T), and nonossified navicular (N). The first metatarsal (1) is also ossified.
Clubfoot. Sonogram of the medial aspect of a normal foot illustrates the relationships between the cartilaginous medial malleolus (M), ossified talus (T), and nonossified navicular (N). The first metatarsal (1) is also ossified.
The important and elusive talonavicular relationship can be quantified by measuring the distances or angles. The distance between the medial malleolar epiphysis and the cartilaginous navicular can be measured. With medial displacement of the navicular in clubfoot, this measurement is shorter than in the normal foot (see the images below).
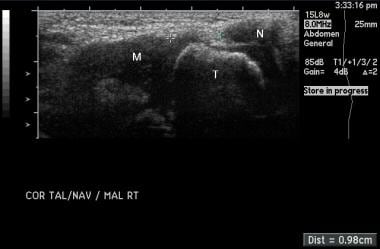 The distance between the medial malleolus (M) and navicular (N) can be reproducibly measured in a dynamic range of motion. Here, it is shown in the neutral position in the normal foot.
The distance between the medial malleolus (M) and navicular (N) can be reproducibly measured in a dynamic range of motion. Here, it is shown in the neutral position in the normal foot.
 With abduction of the normal foot, the distance between the medial malleolus and the navicular increases.
With abduction of the normal foot, the distance between the medial malleolus and the navicular increases.
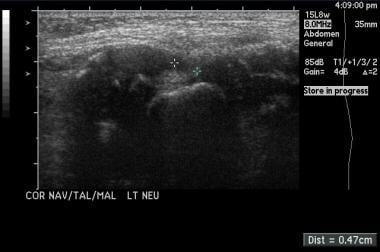
 Image of a clubfoot in abduction shows a smaller increase in the distance between the medial malleolus and navicular, compared with the distance in the normal foot. This patient may benefit from medial soft tissue release.
Image of a clubfoot in abduction shows a smaller increase in the distance between the medial malleolus and navicular, compared with the distance in the normal foot. This patient may benefit from medial soft tissue release.
Hamel and Becker introduced an angle to quantify the talonavicular relationship. With medial subluxation of the navicular, the angle is positive rather than negative, as it is in normal feet. These measurements can be used to preoperatively estimate the amount of medial release necessary or to assess the success of conservative manipulation and use of braces and/or casts. [26]
The lateral transverse view may be used to assess the important calcaneocuboid (lateral column) relationship. Future investigations may show that reproducible quantification of this relationship may be useful in directing surgical release of this joint.
The dynamic imaging that is possible with ultrasonography may complement physical examination in the assessment of the rigidity of the foot. Thus, it may aid in the selection of patients for surgical rather than conservative therapy. [27]
-
Lateral view in talipes equinovarus demonstrates an abnormally elevated tibiocalcaneal angle. A normal angle is 60-90°.
-
Normal lateral view shows the measurement of the talocalcaneal angle. The calcaneal long axis is drawn along the plantar surface. The normal range is 25-45°. Note the normal overlap of the metatarsals on the lateral view.
-
Lateral view of clubfoot shows the nearly parallel talus and calcaneus, with a talocalcaneal angle of less than 25°.
-
Dorsoplantar projection of a healthy foot shows that the line through the long axis of the talus passes just medial to the base of the first metatarsal. The talocalcaneal angle measurement is shown. The normal range is 15-40°.
-
Dorsoplantar views obtained in a patient with unilateral clubfoot show that the talus and calcaneus are more overlapped than in the normal condition. The talocalcaneal angle is 15° or less. Note that the line through the long axis of the talus passes lateral to the first metatarsal due to the varus position of the forefoot.
-
Dorsoplantar view of talipes equinovarus shows that the convergence of the bases of the metatarsals is abnormally increased compared with the normal convergence.
-
Lateral view of shows the ladderlike configuration of the metatarsals in forefoot varus in clubfoot.
-
Image of clubfoot obtained after repair shows restoration of a normal talocalcaneal angle on the dorsoplantar view. The line along the long axis of the talus now passes medial to the first metatarsal; this finding indicates overcorrection of the forefoot varus.
-
Postoperative lateral view of a clubfoot shows persistent parallelism of the talus and calcaneus. Note the characteristic flattening of the talar dome on this true lateral view of the ankle.
-
Lateral radiographs obtained in a 12-year-old girl after surgical clubfoot repair shows persistent forefoot varus and resultant stress changes (cortical thickening) in the most lateral metatarsals.
-
DP radiographs obtained in the same girl as in the previous image after surgical clubfoot repair shows persistent forefoot varus and resultant stress changes to the lateral metatarsals.
-
Clubfoot. Sonogram of the medial aspect of a normal foot illustrates the relationships between the cartilaginous medial malleolus (M), ossified talus (T), and nonossified navicular (N). The first metatarsal (1) is also ossified.
-
The distance between the medial malleolus (M) and navicular (N) can be reproducibly measured in a dynamic range of motion. Here, it is shown in the neutral position in the normal foot.
-
With abduction of the normal foot, the distance between the medial malleolus and the navicular increases.
-
Medial ultrasonogram shows a clubfoot in the neutral position.
-
Image of a clubfoot in abduction shows a smaller increase in the distance between the medial malleolus and navicular, compared with the distance in the normal foot. This patient may benefit from medial soft tissue release.
Tables
Measurement |
Normal Foot |
Clubfoot |
Tibiocalcaneal angle |
60-90° on lateral view |
>90° (hindfoot equinus) on lateral view |
Talocalcaneal angle |
25-45° on lateral view, 15-40° on DP view |
< 25° (hindfoot varus) on lateral view, < 15° (hindfoot varus) on DP view |
Metatarsal convergence |
Slight on lateral view, slight on DP view |
None (forefoot supination) on lateral view, increased (forefoot supination) on DP view |





