Practice Essentials
Choledochal cysts are congenital anomalies of the bile ducts. They consist of cystic dilatations of the extrahepatic biliary tree, intrahepatic biliary radicles, or both. [1, 2] Choledochal cyst is a rare cystic dilatory condition with malignant tendency that is reported more frequently in children. Surgical resection of cysts can significantly decrease the risk of malignancy and reduce associated complications and remains the key to treatment. [3] The 5-year overall survival rate after excision of a choledochal cyst is 95.5%. [4]
The disease usually occurs in children younger than 10 years, so there is a long follow-up after repair. Early or late complications may occur in various organs after surgical repair for choledochal cyst, such as an anastomotic stricture or intrahepatic bile duct stone in the liver; pancreatitis, residual bile duct dilation, or pancreatic fistula/leakage In the pancreas; and Roux-en-Y reconstruction complications In the intestines, such as an obstruction at the site of anastomosis or retrograde intussusception. [5]
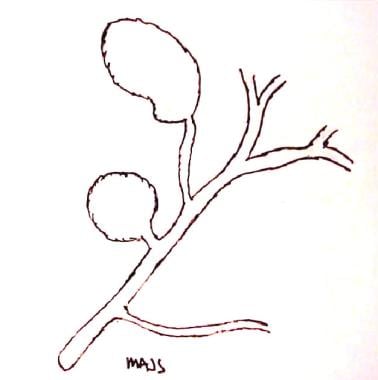
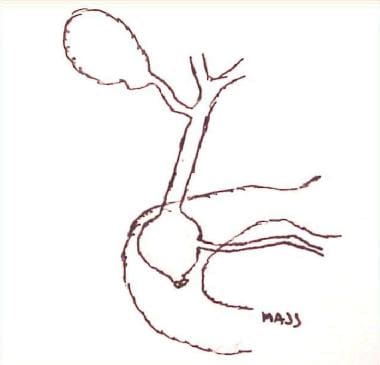
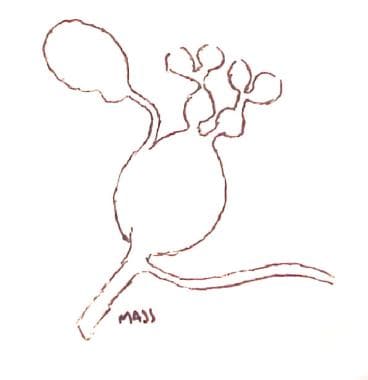
Alonso-Lej et al provided the first systematic description of choledochal cysts based on clinical and anatomic findings in 96 cases. [6] The resultant system classified choledochal cysts into 3 types and outlined therapeutic strategies for each. This classification system for choledochal cysts was further refined by Todani and colleagues and currently includes 5 major types (see the images below). [2, 7, 8]
According to the Todani classification, choledochal cysts are believed to arise as the result of reflux of pancreatic enzymes into the biliary tree due to anomalous pancreaticobiliary duct union. Complications of these cysts include abdominal pain, jaundice, cystolithiasis, cholecystitis, pancreatitis, liver abscess, liver cirrhosis, and malignant transformation. [4]
An association exists between an anomalous pancreaticobiliary junction (APBJ) and choledochal cysts, cholangiocarcinoma, and carcinoma of the gallbladder. The potential exists for imaging modalities to miss small cancers of the bile ducts and gallbladder; however, definitive surgery should be planned for all patients and should include resection of incidental lesions.
In a study of 394 patients with choledochal cysts, 10 (2.5%) had cholangiocarcinoma. On follow-up, 13 patients (3.3%) presented with biliary cancer. Adults were found to be more likely to present with abdominal pain, and children more likely to present with jaundice. Type I choledochal cysts were seen more often in children, and type IV more often in adults. [9]
Radiologists, gastroenterologists, and surgeons should work as a team when treating patients with choledochal cyst. The diagnostic workup should not cease until all are satisfied that enough information is available for operative planning. Such information usually includes data derived through a combination of ultrasonography (US) and computed tomography (CT) scanning, magnetic resonance imaging (MRI)/magnetic resonance cholangiopancreatography (MRCP), and endoscopic retrograde cholangiopancreatography (ERCP). [2]
(See the images below.)

Imaging modalities
Radiologic and endoscopic imaging is the cornerstone of choledochal cyst diagnosis. Management is generally guided by cyst classification; complete cyst excision is necessary for choledochal cysts with high potential for malignant transformation, such as types I and IV. Five-year overall survival after choledochal cyst excision is 95.5%. [4]
A number of imaging modalities such as ultrasonography, CT, MRCP, ERCP, and percutaneous transhepatic cholangiography can be used to detect a choledochal cyst. [1] Magnetic resonance cholangiopancreatography, in particular, can be helpful in detecting an abnormal pancreaticobiliary junction. [10, 11]
According to Miyano and Yamataka, the preferred initial radiologic examination in the diagnostic workup of a choledochal cyst is an abdominal ultrasound. [12] Ultrasound scanning is noninvasive and involves no radiation exposure, and its findings are sensitive and specific for the diagnosis. Clinically, these features make sense. Patients with choledochal cysts most often have symptoms referable to the hepatobiliary system, and most US operators are familiar with the anatomy of this area.
In a study by Cochran et al, infants who were prenatally suspected of having a choledochal cyst and had prenatal ultrasounds underwent ultrasound imaging shortly after birth to identify newborns at risk for early complications. Of the 23 patients, 5 (21.7%) developed symptoms at a median age of 16.5 days, and 18 (78.3%) remained asymptomatic throughout the first year after birth. Five patients (21.7%) had cysts of 4.5 cm or greater, and 18 (78.3%) had cysts less than 4.5 cm. Postnatal cyst size of 4.5 cm or greater was associated with neonatal symptom manifestation, with 88.9% specificity and 60% sensitivity. [13]
Once a preliminary diagnosis has been made using US scanning, other supportive studies may be ordered, including abdominal CT scans, MRI studies, or MRCP examinations. [14, 15, 16] These studies reveal the cyst in more precise anatomic detail. In addition, important anatomic relationships to surrounding structures are better defined than with other modalities.
Angiographic techniques are not part of the standard workup for choledochal cysts. However, angiographic studies and angiographic interventions can be instrumental, and even lifesaving, when major vascular complications associated with choledochal cysts occur. Fortunately, these complications are rare, and most experience has been limited to case reports. [17, 18]
Endoscopic retrograde cholangiopancreatography (ERCP) has the highest diagnostic accuracy for choledochal cysts, but because of associated complications, exposure to ionizing radiation, and its invasive nature, use of ERCP has been limited in suspected cases of choledochal cyst. This modality provides the benefit of being both diagnostic and therapeutic, which is of particular interest in patients with type III choledochal cysts (choledochoceles), for whom endoscopic sphincterotomy can be performed. [19]
Limitations of techniques
Ultrasound scanning is an excellent choice for initial imaging, but it does have limitations, including the fact that its effectiveness is dependent on operator experience, that cysts on US images may be misinterpreted as the gallbladder or other structures, and that US scanning shows decreased sensitivity in the presence of overlying bowel gas, pancreatitis, cholangitis, or other inflammatory processes. Differentiating a choledochal cyst from a hepatic cyst, a hepatic abscess, an acute fluid collection, or a pancreatic pseudocyst may be difficult.
Radiography
Plain abdominal radiographs are of little use in the diagnosis of choledochal cysts. They offer no specific information related to this diagnosis. For patients presenting with abdominal pain, radiographs are frequently ordered as part of the standard workup. At best, radiographs may suggest displacement of an adjacent hollow viscus such as the duodenum by a mass.
False-positive and false-negative rates are high if the diagnosis is based on plain abdominal radiographs. Plain radiographs cannot depict choledochal cysts well. Many other masses or inflammatory processes can produce the same clinical picture, which cannot be differentiated by use of plain images. Examples of these processes include an acute fluid collection associated with acute pancreatitis, a pancreatic pseudocyst, and choledocholithiasis or cholangitis.
Computed Tomography
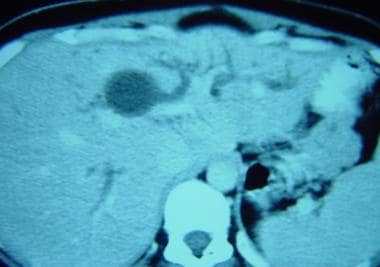
Abdominal CT scanning is useful in the diagnostic algorithm for choledochal cysts (see the images below). Computed tomography is highly accurate and offers a great deal of information that is helpful not only in confirming the diagnosis but also in planning surgical approaches.
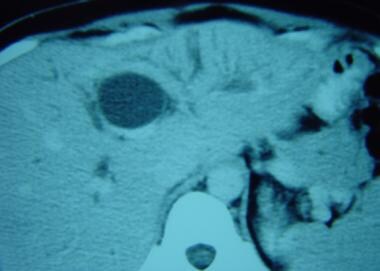
 Computed tomography scan demonstrates a choledochal cyst involving the intrahepatic portion of the common hepatic duct and the main left hepatic duct.
Computed tomography scan demonstrates a choledochal cyst involving the intrahepatic portion of the common hepatic duct and the main left hepatic duct.
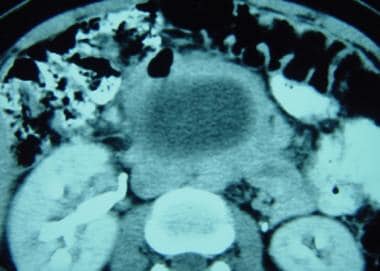 Computed tomography (CT) CT scan demonstrates the proximity of the duodenum to the distal aspect of a choledochal cyst.
Computed tomography (CT) CT scan demonstrates the proximity of the duodenum to the distal aspect of a choledochal cyst.
CT scans of a choledochal cyst show a dilated cystic mass with clearly defined walls that is separate from the gallbladder. The fact that this mass arises from or actually is the extrahepatic bile duct usually is clear from its location and its relationships to surrounding structures. The cyst is typically filled with bile, which produces waterlike attenuation. Depending on the patient's age and clinical history, the wall of the cyst can appear thickened, especially if multiple episodes of inflammation and cholangitis have occurred.
Most patients with choledochal cysts have undergone abdominal US imaging prior to CT scanning. US findings suggest the diagnosis in most patients and may be conclusive in many.
According to Lipsett and colleagues, CT scanning confirms an unclear diagnosis and provides information concerning the relationship of the cyst to surrounding structures. [20] These include portal vein, duodenum, and liver. In addition, CT scanning is superior to US scanning in defining the extent of the cyst in the extrahepatic biliary system and in detecting intrahepatic disease.
CT cholangiography is one of the CT imaging techniques that have been used in the diagnosis of choledochal cysts.
Lam and colleagues investigated the use of CT cholangiography versus MR cholangiography in the diagnosis of choledochal cysts in 14 children and described good results with both techniques. [21] Satisfactory visualization of the biliary tree was achieved in 93% of patients by using CT cholangiography and in 100% of patients by using MR cholangiography. CT cholangiography adequately depicted 10 (91%) of 11 choledochal cysts, whereas MR cholangiography showed 100% of the cysts. Intrahepatic stones were detected, with sensitivities of 83% and 67% for CT scanning and MR cholangiography, respectively. Specificities were 100% for both. CT cholangiography revealed the pancreatic duct and the common pancreatobiliary channel in 64% of patients, whereas MR cholangiography depicted these features in 46%. Postoperatively, CT cholangiography was better for surveillance of the hepaticojejunostomy.
Researchers have recommended the use of MR cholangiography as the confirmatory imaging study in children with choledochal cysts because it does not require breath holding, is noninvasive, does not require administration of contrast material, and is not associated with ionizing radiation.
Degree of confidence
CT scans can be relied on with a high degree of confidence. False-positive and false-negative results with CT are rare. CT scans provide a great deal of information concerning choledochal cysts and their relationships to surrounding structures. Typically, the only preoperative study that may be considered after a confirmatory CT scan is endoscopic retrograde cholangiopancreatography (ERCP). ERCP often provides additional information concerning the pancreatic duct and the distal extent of the choledochal cyst, and it can reveal more detailed information concerning the epithelium of the cyst while detecting the presence of associated tumors or strictures.
Magnetic Resonance Imaging
Use of magnetic resonance imaging (MRI) and magnetic resonance cholangiopancreatography (MRCP) techniques is increasing dramatically for the noninvasive diagnosis of biliary and pancreatic diseases. [10] Choledochal cysts are no exception. These cysts appear as large fusiform or saccular masses that may be extrahepatic, intrahepatic, or both, depending on the type of cyst. They produce a particularly strong signal on T2-weighted images. Associated anomalies of the pancreatic duct, its junction with the common bile duct, and the long common channel formed by these 2 structures are usually well demonstrated on MRI/MRCP images. [22, 23, 24, 25, 26, 27, 28]
In a single-center retrospective analysis of 18 fetuses diagnosed with choledochal cyst through prenatal MRI, Wu and colleagues found that the sensitivity of prenatal MRI signs were greater than postnatal MRCP signs (100% vs 76.9%). [29]
Irie and associates reported that MRCP is an important noninvasive diagnostic study for choledochal cysts but suggested that it should not replace ERCP, especially in children. These investigators used MRCP in the diagnosis of choledochal cysts in 16 patients. [30] They found that MRCP defined the proximal bile duct better than ERCP but that defects in the distal common bile duct were missed with MRCP in 2 pediatric patients. The anomalous pancreaticobiliary junction (APBJ) was delineated in all 6 adult patients but was missed in 6 of 10 pediatric patients.
Kim et al concluded that MR cholangiography is equivalent or superior to conventional cholangiography in the evaluation of choledochal cysts. These researchers compared MR cholangiography with conventional cholangiography in 13 patients with choledochal cysts. [31] Magnetic resonance cholangiography was superior for complete imaging of the cyst. Detection rates for the APBJ and for bile duct stones were not significantly different.
Degree of confidence
On the basis of reported results, MRCP appears to be a reliable study in the diagnosis of choledochal cysts, with diagnostic accuracy of 82-100%. [11] In preparation for surgery, particularly when information is needed concerning the location of the APBJ and the length of the common channel, an additional study such as ERCP should be performed.
Differentiating a choledochal cyst from a pancreatic pseudocyst or other cystic lesions of the pancreas may be difficult on the basis of MRI findings.
No normal anatomic variants mimic a choledochal cyst. However, false-negative findings of the absence of the APBJ and the common pancreatobiliary channel are possible. In addition, small neoplasms of the gallbladder and the bile duct may be missed.
Ultrasonography
Ultrasonography (US) scanning is the initial screening examination of choice for patients with choledochal cysts. Pertinent findings include a cystic extrahepatic mass. Depending on the skill of the operator, the specific type or class of choledochal cyst may be identified. [32] High-resolution US equipment helps clinicians make such diagnoses. Furthermore, advances in US technology have enabled ultrasonographers to make the diagnosis during the antenatal period. [33, 34, 35]
(A diagnostic sonogram is shown in the image below.)
 Diagnostic sonogram demonstrating a type I choledochal cyst in a 4-month-old child presenting with elevated hyperbilirubinemia and hepatic transaminase levels.
Diagnostic sonogram demonstrating a type I choledochal cyst in a 4-month-old child presenting with elevated hyperbilirubinemia and hepatic transaminase levels.
Ultrasound findings are diagnostic for many patients; however, during the preoperative period, complementary studies such as ERCP, CT, or MRI/MRCP may be helpful in delineating details of surrounding anatomy, location of an APBJ, and length of the common pancreatobiliary channel.
Abdominal US findings can help detect conditions associated with choledochal cysts. as well as complications of choledochal cysts, such as choledocholithiasis, intrahepatic biliary dilatation, portal vein thrombosis, gallbladder or biliary neoplasms, pancreatitis, and hepatic abscesses.
Tannuri et al reported that they found that US was the only necessary diagnostic imaging in patients with choledochal cysts and that performing bile enteric anastomosis in the lower portion of the common hepatic duct was safer and was associated with a lower risk of complications. [36]
Xin et al reported that US can be used to effectively diagnose perforation of a congenital choledochal cyst in children. [37]
In a surgical series with a total of 140 patients, ultrasound findings, although sensitive, were routinely confirmed by performing another study or procedure, such as CT scanning, hepatoiminodiacetic acid scanning, or ERCP. [38, 39, 40]
Sato et al reviewed their US findings in 12 patients with choledochal cysts and found that cyst diameter changed greatly under compression. These authors cautioned against compressing these structures because this can lead to confusion about the diagnosis. [41]
Degree of confidence
Ultrasonography is sensitive in demonstrating a cystic lesion in the region of the porta hepatis. If such a lesion is visualized, US frequently provides enough information to inform the diagnosis of a choledochal cyst.
No actual normal variants are mimetic of choledochal cysts. Pathologic conditions in the differential diagnosis include pancreatic pseudocysts, hepatic cysts, and biliary atresia with associated cystic masses. At times, differentiating these lesions may be difficult on the basis of ultrasound findings. In this situation, other confirmatory tests are indicated.
Nuclear Imaging
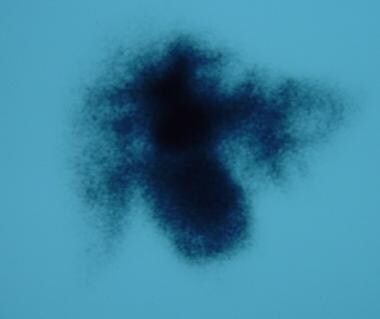
Hepatobiliary scintigraphic modalities are used commonly in the setting of acute cholecystitis and in the investigation of neonatal jaundice. In addition, these techniques are useful in the diagnosis of choledochal cysts (see the images below).
 Nuclear medicine scan of a choledochal cyst. Early image shows most of the radionuclide in the liver.
Nuclear medicine scan of a choledochal cyst. Early image shows most of the radionuclide in the liver.
 Nuclear medicine scan of a choledochal cyst midway through the study, with better filling of the cyst by the radionuclide (see the previous image).
Nuclear medicine scan of a choledochal cyst midway through the study, with better filling of the cyst by the radionuclide (see the previous image).
 Nuclear medicine scan of a choledochal cyst late in the study, with the cyst completely defined (see the previous 2 images).
Nuclear medicine scan of a choledochal cyst late in the study, with the cyst completely defined (see the previous 2 images).
Kao et al concluded that nonvisualization of the gallbladder on cholescintigraphy in patients with choledochal cysts is not necessarily indicative of acute cholecystitis and that large choledochal cysts may compress the gallbladder, leading to nonvisualization. This study included 27 patients with choledochal cysts. Nonvisualization of the gallbladder occurred in 18 (67%) of 27 patients at 4 hours after injection of radionuclide. Most patients did not have acute cholecystitis. [42]
Rajnish et al reported that hepatobiliary scintigraphy was effective in helping to diagnose type I and type IV choledochal cysts. A total of 21 patients with confirmed choledochal cysts (12 type I, 9 type IV) had cholescintigraphic examinations; 2 nuclear medicine specialists were asked to review the scans in an attempt to classify choledochal cysts according to the Todani classification. [8]
Hepatobiliary scintigraphy has been shown to correlate with ERCP or surgical diagnosis in 86% of patients. In one study, all 12 type I cysts were diagnosed correctly using hepatobiliary scintigraphy. Sensitivity for the diagnosis and classification of type IV cysts was 67% (6 of 9 cases). The difficulty involved relative inability to diagnose intrahepatic disease in patients with type IV cysts.
Technetium-99m hepatobiliary iminodiacetic acid (HIDA) scan can be performed to distinguish between a choledochal cyst and biliary atresia in neonates. This imaging study is also beneficial for detecting spontaneous rupture of choledochal cysts, which would be characterized by leakage of dye into the peritoneal cavity. [19]
Kawaguchi et al evaluated the usefulness of hepatobiliary scintigraphy, a minimally invasive method used to evaluate bile flow dynamics, for predicting late complications in patients with choledochal cysts. Researchers included 108 pediatric patients (median age at surgery, 2 yr 11 mo) and found no significant difference in the occurrence of hepatolithiasis between cholestasis and noncholestasis patients but noted that cholangitis was significantly more common in the cholestasis group. [43]
Degree of confidence
Hepatobiliary scintigraphy has reasonably good accuracy in the diagnosis of choledochal cysts. However, it probably should not be relied on as the sole study and should be complemented by ERCP, CT scanning, or MRCP.
No known normal anatomic variants mimic this disease process. However, false-negative results can derive from relative inability to diagnose intrahepatic disease in type IV choledochal cysts.
-
Type I choledochal cyst.
-
Type II choledochal cyst.
-
Type III choledochal cyst.
-
Type IV (A) choledochal cyst.
-
Type V choledochal cyst (Caroli disease).
-
Nuclear medicine scan of a choledochal cyst. Early image shows most of the radionuclide in the liver.
-
Nuclear medicine scan of a choledochal cyst midway through the study, with better filling of the cyst by the radionuclide (see the previous image).
-
Nuclear medicine scan of a choledochal cyst late in the study, with the cyst completely defined (see the previous 2 images).
-
Computed tomography scan demonstrates a choledochal cyst involving the intrahepatic portion of the common hepatic duct and the main left hepatic duct.
-
Choledochal cyst involving the intrahepatic common hepatic duct.
-
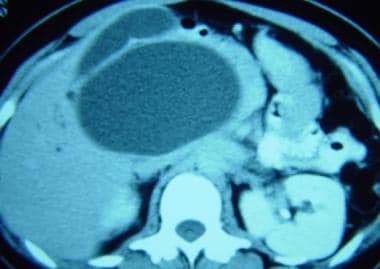
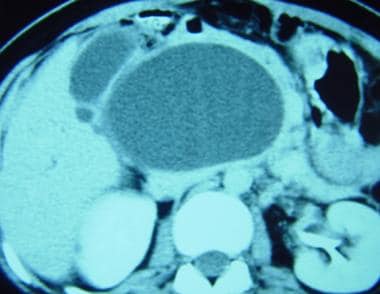
Large, saccular, type I choledochal cyst compressing the adjacent gallbladder.
-
Large type I choledochal cyst and adjacent gallbladder.
-
Computed tomography (CT) CT scan demonstrates the proximity of the duodenum to the distal aspect of a choledochal cyst.
-
Diagnostic sonogram demonstrating a type I choledochal cyst in a 4-month-old child presenting with elevated hyperbilirubinemia and hepatic transaminase levels.
-
Operative cholangiogram delineating choledochal cyst and pertinent associated biliary anatomy.
-
Surgical specimen.
-
Roux-en-Y hepaticojejunostomy to restore biliary-enteric continuity following resection of choledochal cyst







