Practice Essentials
The Chiari type II malformation (Arnold-Chiari malformation) is a complex congenital malformation of the brain, nearly always associated with myelomeningocele (see the images below), and the most common serious malformation of the posterior fossa. This condition has skull, dural, brain, spinal, and spinal cord manifestations, including downward displacement of the medulla, fourth ventricle, and cerebellum into the cervical spinal canal, as well as elongation of the pons and fourth ventricle, probably due to a relatively small posterior fossa. [1, 2, 3]
The differential diagnosis includes spinal astrocytoma, Chiari I malformation, chordoma, and encephalocele. Other conditions to be considered include fourth ventricle ependymoma, Lhermitte-Duclos disease, rhombencephalosynapsis, and tectocerebellar dysraphia with posterior encephalocele. [4]
Prenatal surgery for myelomeningocele reduces the need for ventricular shunting and improves motor outcomes in infants with Chiari II malformation. A study performed on the MRIs of 102 fetuses with open spinal dysraphism (OSD) found that in fetuses with severe Chiari II malformation that did not undergo prenatal repair, most (65.5%) had no change in severity of cerebellar ectopia/Chiari grade postnatally. In fetuses that underwent in utero repair, most (81.3%) had resolution of cerebellar ectopia postnatally. [5]
Complete reversibility of Chiari II malformation after postnatal repair of myelomeningocele has been reported. In a study by Beuriat et al of 47 patients who had a Chiari II malformation confirmed before myelomeningocele repair, only 28 (45.9%) patients had Chiari II malformation after myelomeningocele closure. The reversibility rate was 40.4%. [6]
Chiari II malformation is best explained with the theory of McLone and Knepper, which allows the hindbrain disorder to be conceptualized as resulting from a normal-sized cerebellum developing in an abnormally small posterior fossa with a low tentorial attachment. [7]
 A thoracic-level myelomeningocele (short arrow) is seen in a patient with a Chiari II malformation (long arrow).
A thoracic-level myelomeningocele (short arrow) is seen in a patient with a Chiari II malformation (long arrow).
 Sagittal T2-weighted magnetic resonance image in a patient with a Chiari II malformation. This image shows a thoracic-level myelomeningocele (arrows). The spinal cord, in addition to the thoracic placode, also extends distally and is further tethered at the sacral level.
Sagittal T2-weighted magnetic resonance image in a patient with a Chiari II malformation. This image shows a thoracic-level myelomeningocele (arrows). The spinal cord, in addition to the thoracic placode, also extends distally and is further tethered at the sacral level.
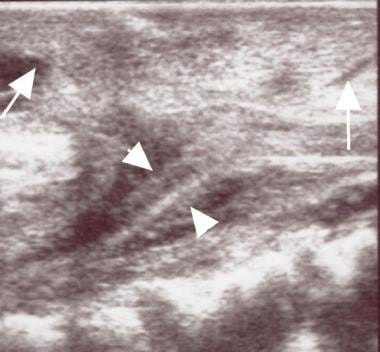 Sagittal ultrasonogram in a patient with a Chiari II malformation. This image shows the thoracic spinal cord (arrowheads) and myelomeningocele (arrows). Note the tethering of the placode at the site of the dysraphic defect.
Sagittal ultrasonogram in a patient with a Chiari II malformation. This image shows the thoracic spinal cord (arrowheads) and myelomeningocele (arrows). Note the tethering of the placode at the site of the dysraphic defect.
Anatomy
The Chiari II malformation is a complex deformity of the calvarium, dura, and hindbrain, and it is almost always associated with myelomeningocele. The spectrum of abnormalities in Chiari II malformation is broad, with many findings reported.
Osseous changes in Chiari II malformation include a lacunar skull or luckenschadel; concave clivus and petrous ridge alterations; a small posterior fossa and gaping foramen magnum; and low-lying transverse sinuses.
Almost all patients manifest dysplasia of the membranous bones of the calvarium (lacunar skull or luckenschadel), which appears as clusters of areas of thinning, pits, and fenestrae that are most prominent near the vertex or torcular herophili (see the image below). These findings may be observed in utero in a fetus as early as at 8 months' gestation. The lacunar skull typically persists until the age of 1-3 months and then disappears at about 6 months of age, regardless of whether progressive hydrocephalus is present. Subtle calvarial thinning and scalloping may persist into adulthood.
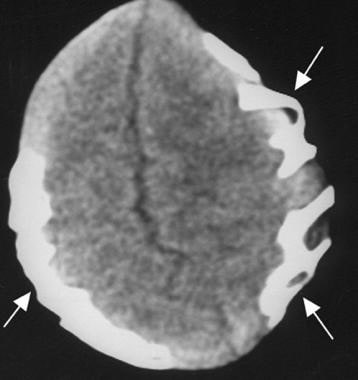 Deep scalloping between the bony septations that characterize the lacunar skull (luckenschadel) (arrows) are best appreciated on an axial computed tomography section, as in this patient with a Chiari II malformation.
Deep scalloping between the bony septations that characterize the lacunar skull (luckenschadel) (arrows) are best appreciated on an axial computed tomography section, as in this patient with a Chiari II malformation.
Clivus and petrous ridge alterations include concavity of the posterior aspects of the petrous temporal bones (see the first image below) and an abnormal clivus that is often short, with a concave configuration similar to that of the petrous ridges (see the second image below).
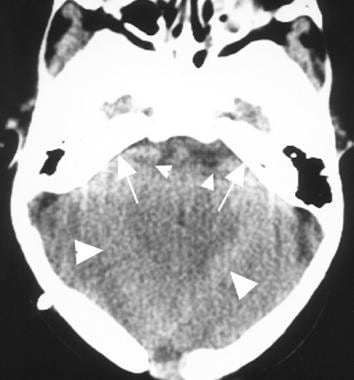 Axial computed tomography scan in a patient with a Chiari II malformation. This image shows a gaping, somewhat heart-shaped tentorial incisura (large arrowheads) that appears to be completely plugged with the upwardly herniating cerebellum. The cerebellar hemispheres extend anteromedially (small arrowheads) and almost completely engulf the brainstem. The petrous ridges are concave (arrows).
Axial computed tomography scan in a patient with a Chiari II malformation. This image shows a gaping, somewhat heart-shaped tentorial incisura (large arrowheads) that appears to be completely plugged with the upwardly herniating cerebellum. The cerebellar hemispheres extend anteromedially (small arrowheads) and almost completely engulf the brainstem. The petrous ridges are concave (arrows).
 Sagittal T1-weighted magnetic resonance image of posterior fossa abnormalities in Chiari II malformation: (1) colpocephaly; (2) beaked tectum; (3) cascade of an inferiorly displaced vermis behind the medulla; (4) elongated, tubelike fourth ventricle; (5) low-lying torcular herophili; (6) cerebellar hemispheres wrapping around the brainstem anteriorly; (7) concave clivus; (8) medullary spur; and (9) medullary kink.
Sagittal T1-weighted magnetic resonance image of posterior fossa abnormalities in Chiari II malformation: (1) colpocephaly; (2) beaked tectum; (3) cascade of an inferiorly displaced vermis behind the medulla; (4) elongated, tubelike fourth ventricle; (5) low-lying torcular herophili; (6) cerebellar hemispheres wrapping around the brainstem anteriorly; (7) concave clivus; (8) medullary spur; and (9) medullary kink.
Other osseous changes include a small posterior fossa and gaping foramen magnum, as well as low-lying transverse sinuses. The posterior fossa is exceptionally small; the foramen magnum is larger and rounder than usual, and the internal occipital protuberance is situated just superior to the foramen magnum. The transverse sinuses and torcular herophili are low lying (see the following images).
Sagittal T1-weighted magnetic resonance image of posterior fossa abnormalities in Chiari II malformation: (1) colpocephaly; (2) beaked tectum; (3) cascade of an inferiorly displaced vermis behind the medulla; (4) elongated, tubelike fourth ventricle; (5) low-lying torcular herophili; (6) cerebellar hemispheres wrapping around the brainstem anteriorly; (7) concave clivus; (8) medullary spur; and (9) medullary kink.
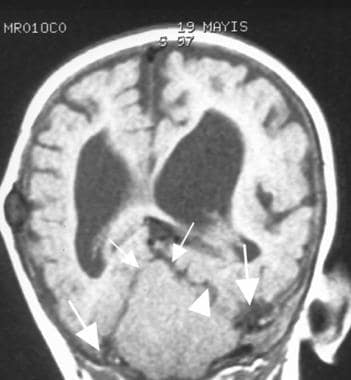 Coronal T1-weighted magnetic resonance image in a patient with a Chiari II malformation. This image shows low-lying transverse sinuses (arrows), hydrocephalus, and a small posterior fossa. A hypoplastic tentorium cerebelli with gaping incisura (arrowhead) is present with a towering cerebellum (small arrows).
Coronal T1-weighted magnetic resonance image in a patient with a Chiari II malformation. This image shows low-lying transverse sinuses (arrows), hydrocephalus, and a small posterior fossa. A hypoplastic tentorium cerebelli with gaping incisura (arrowhead) is present with a towering cerebellum (small arrows).
Changes to the dura include a fenestrated falx, hypoplastic tentorium, and heart-shaped incisura. The falx almost always shows partial absence, hypoplasia, and/or fenestrations (see the first image below). The tentorium is hypoplastic, attaching to the occipital bone far caudally, just above the foramen magnum (see the second image below), and the hypoplastic tentorial leaves arise laterally from the low-lying transverse sinuses (see the third image below).
 Axial T2-weighted magnetic resonance image in a patient with a Chiari II malformation. This image shows a hypoplastic fenestrated falx cerebri with striking interdigitation of the gyri (arrows).
Sagittal T1-weighted magnetic resonance image of posterior fossa abnormalities in Chiari II malformation: (1) colpocephaly; (2) beaked tectum; (3) cascade of an inferiorly displaced vermis behind the medulla; (4) elongated, tubelike fourth ventricle; (5) low-lying torcular herophili; (6) cerebellar hemispheres wrapping around the brainstem anteriorly; (7) concave clivus; (8) medullary spur; and (9) medullary kink.
Axial computed tomography scan in a patient with a Chiari II malformation. This image shows a gaping, somewhat heart-shaped tentorial incisura (large arrowheads) that appears to be completely plugged with the upwardly herniating cerebellum. The cerebellar hemispheres extend anteromedially (small arrowheads) and almost completely engulf the brainstem. The petrous ridges are concave (arrows).
Axial T2-weighted magnetic resonance image in a patient with a Chiari II malformation. This image shows a hypoplastic fenestrated falx cerebri with striking interdigitation of the gyri (arrows).
Sagittal T1-weighted magnetic resonance image of posterior fossa abnormalities in Chiari II malformation: (1) colpocephaly; (2) beaked tectum; (3) cascade of an inferiorly displaced vermis behind the medulla; (4) elongated, tubelike fourth ventricle; (5) low-lying torcular herophili; (6) cerebellar hemispheres wrapping around the brainstem anteriorly; (7) concave clivus; (8) medullary spur; and (9) medullary kink.
Axial computed tomography scan in a patient with a Chiari II malformation. This image shows a gaping, somewhat heart-shaped tentorial incisura (large arrowheads) that appears to be completely plugged with the upwardly herniating cerebellum. The cerebellar hemispheres extend anteromedially (small arrowheads) and almost completely engulf the brainstem. The petrous ridges are concave (arrows).
Changes to the cerebellum, medulla, and spinal cord include a cerebellar peg, medullary kink, and a towering cerebellum or vermian pseudotumor. In addition, the fourth ventricle is elongated and tubelike; the cerebellopontine cistern and the cisterna magna are obliterated; and the combined displacements of the spinal cord, medulla, pons, and cerebellum form a cascade of herniations, each of which compresses all of the tissue in front of it and displaces them anteriorly.
In older patients, a wide subarachnoid space may be seen behind a vermis that is deeply grooved at the level of cervical nerve C1. The vertebral artery frequently loops on itself within the cervical canal and passes caudally to the level of cervical nerve C3. The possible cause of this groove may be the pulsatile effect of the vertebral artery on the adjacent cerebellum.
Protrusion of vermis and hemispheres through the foramen magnum (90%) results in craniocaudal elongation of cerebellum behind the spinal cord, or cerebellar peg (see the following images).
Sagittal T1-weighted magnetic resonance image of posterior fossa abnormalities in Chiari II malformation: (1) colpocephaly; (2) beaked tectum; (3) cascade of an inferiorly displaced vermis behind the medulla; (4) elongated, tubelike fourth ventricle; (5) low-lying torcular herophili; (6) cerebellar hemispheres wrapping around the brainstem anteriorly; (7) concave clivus; (8) medullary spur; and (9) medullary kink.
 Sagittal midline T1-weighted magnetic resonance image in a patient with a Chiari II malformation. This image shows a large massa intermedia (long arrow) and a beaked tectum (short arrow). Other posterior fossa abnormalities are also seen in this patient.
A thoracic-level myelomeningocele (short arrow) is seen in a patient with a Chiari II malformation (long arrow).
Sagittal midline T1-weighted magnetic resonance image in a patient with a Chiari II malformation. This image shows a large massa intermedia (long arrow) and a beaked tectum (short arrow). Other posterior fossa abnormalities are also seen in this patient.
A thoracic-level myelomeningocele (short arrow) is seen in a patient with a Chiari II malformation (long arrow).
The medulla is kinked inferiorly (75%) and lies dorsal to the spinal cord, which is unable to descend because of competent dentate ligaments (see the images below). In addition, the corners of the cerebellum are wrapped around the brainstem, pointing anteriorly and laterally (also shown in the images below).
Sagittal T1-weighted magnetic resonance image of posterior fossa abnormalities in Chiari II malformation: (1) colpocephaly; (2) beaked tectum; (3) cascade of an inferiorly displaced vermis behind the medulla; (4) elongated, tubelike fourth ventricle; (5) low-lying torcular herophili; (6) cerebellar hemispheres wrapping around the brainstem anteriorly; (7) concave clivus; (8) medullary spur; and (9) medullary kink.
Sagittal midline T1-weighted magnetic resonance image in a patient with a Chiari II malformation. This image shows a large massa intermedia (long arrow) and a beaked tectum (short arrow). Other posterior fossa abnormalities are also seen in this patient.
The cerebellar hemispheres and vermis also extend above the incisura of the tentorium (see the following image).
Coronal T1-weighted magnetic resonance image in a patient with a Chiari II malformation. This image shows low-lying transverse sinuses (arrows), hydrocephalus, and a small posterior fossa. A hypoplastic tentorium cerebelli with gaping incisura (arrowhead) is present with a towering cerebellum (small arrows).
The fourth ventricle is elongated craniocaudally, narrowed transversely, and decreased in anteroposterior diameter, resulting in a tubelike, elongated ventricle (see the following images)
Sagittal T1-weighted magnetic resonance image of posterior fossa abnormalities in Chiari II malformation: (1) colpocephaly; (2) beaked tectum; (3) cascade of an inferiorly displaced vermis behind the medulla; (4) elongated, tubelike fourth ventricle; (5) low-lying torcular herophili; (6) cerebellar hemispheres wrapping around the brainstem anteriorly; (7) concave clivus; (8) medullary spur; and (9) medullary kink.
Sagittal midline T1-weighted magnetic resonance image in a patient with a Chiari II malformation. This image shows a large massa intermedia (long arrow) and a beaked tectum (short arrow). Other posterior fossa abnormalities are also seen in this patient.
A thoracic-level myelomeningocele (short arrow) is seen in a patient with a Chiari II malformation (long arrow).
Changes to the midbrain and the third and lateral ventricles include a beaked tectum, hydrocephalus, colpocephaly, and prominent massa intermedia. About one third of patients have a partial block at the level of the ambient cisterns.
Variable degrees of fusion of the colliculi and tectum result in prominent beaking and inferior displacement of the tectal plate (see the images below).
Sagittal T1-weighted magnetic resonance image of posterior fossa abnormalities in Chiari II malformation: (1) colpocephaly; (2) beaked tectum; (3) cascade of an inferiorly displaced vermis behind the medulla; (4) elongated, tubelike fourth ventricle; (5) low-lying torcular herophili; (6) cerebellar hemispheres wrapping around the brainstem anteriorly; (7) concave clivus; (8) medullary spur; and (9) medullary kink.
Sagittal midline T1-weighted magnetic resonance image in a patient with a Chiari II malformation. This image shows a large massa intermedia (long arrow) and a beaked tectum (short arrow). Other posterior fossa abnormalities are also seen in this patient.
 Sagittal midline ultrasonogram shows a large massa intermedia (long arrow) and a beaked tectum (short arrow). This image also shows obliteration of the cisterna magna and the fourth ventricle, as well as compression of the pons and brainstem.
Sagittal midline ultrasonogram shows a large massa intermedia (long arrow) and a beaked tectum (short arrow). This image also shows obliteration of the cisterna magna and the fourth ventricle, as well as compression of the pons and brainstem.
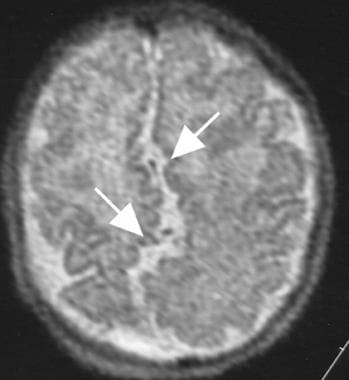
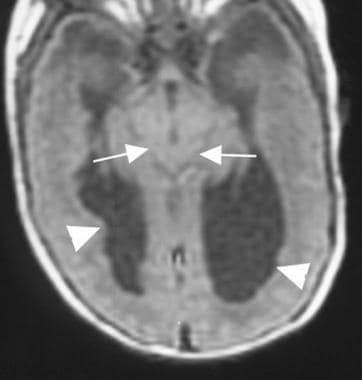 Axial T1-weighted magnetic resonance image in a patient with a Chiari malformation. This image shows a beaked tectum (arrows) and colpocephaly (arrowheads).
Axial T1-weighted magnetic resonance image in a patient with a Chiari malformation. This image shows a beaked tectum (arrows) and colpocephaly (arrowheads).
Ventricular dilatation (hydrocephalus) is present in 98% of patients (see the following image), and 90% require a shunt.
Coronal T1-weighted magnetic resonance image in a patient with a Chiari II malformation. This image shows low-lying transverse sinuses (arrows), hydrocephalus, and a small posterior fossa. A hypoplastic tentorium cerebelli with gaping incisura (arrowhead) is present with a towering cerebellum (small arrows).
Colpocephaly, in which the occipital horns and atria are often mildly enlarged because of maldeveloped occipital lobes, especially in the presence of a malformation involving the corpus callosum, may be seen (see the images below).
Sagittal T1-weighted magnetic resonance image of posterior fossa abnormalities in Chiari II malformation: (1) colpocephaly; (2) beaked tectum; (3) cascade of an inferiorly displaced vermis behind the medulla; (4) elongated, tubelike fourth ventricle; (5) low-lying torcular herophili; (6) cerebellar hemispheres wrapping around the brainstem anteriorly; (7) concave clivus; (8) medullary spur; and (9) medullary kink.
Sagittal midline ultrasonogram shows a large massa intermedia (long arrow) and a beaked tectum (short arrow). This image also shows obliteration of the cisterna magna and the fourth ventricle, as well as compression of the pons and brainstem.
Axial T1-weighted magnetic resonance image in a patient with a Chiari malformation. This image shows a beaked tectum (arrows) and colpocephaly (arrowheads).
A prominent massa intermedia, herniation of the third ventricle into the suprasellar cistern, and an enlarged suprapineal recess are often seen (see the following images). Frequently, a large third ventricle is present as well.
Sagittal midline T1-weighted magnetic resonance image in a patient with a Chiari II malformation. This image shows a large massa intermedia (long arrow) and a beaked tectum (short arrow). Other posterior fossa abnormalities are also seen in this patient.
Sagittal midline ultrasonogram shows a large massa intermedia (long arrow) and a beaked tectum (short arrow). This image also shows obliteration of the cisterna magna and the fourth ventricle, as well as compression of the pons and brainstem.
Other anomalies associated with Chiari II malformations include the following:
-
Myelomeningocele (88-100%)
-
Dysgenesis of corpus callosum (80-90%)
-
Obstructive hydrocephalus following closure of myelomeningocele (50-98%)
-
Syringohydromyelia (50-90%)
-
Aqueductal stenosis (70%)
-
Absence of septum pellucidum (40%)
-
Contracted, narrow gyri (stenogyria; 50%)
-
Heterotopias
-
Diastematomyelia
-
Segmentation anomalies (< 10%), incomplete C1 arch
-
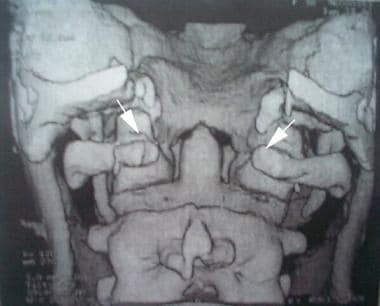
Malrotation of the posterior arches of C1 and C2, as seen in the image below
 Inferior operativelike view on 3-dimensional computed tomography scan. This image shows malrotation of the posterior arches of C1 (long arrow) and C2 (short arrow). Courtesy of Duffau et al.
Inferior operativelike view on 3-dimensional computed tomography scan. This image shows malrotation of the posterior arches of C1 (long arrow) and C2 (short arrow). Courtesy of Duffau et al.
-
Low-lying, often-tethered conus medullaris below lumbar nerve L2
-
Rare anomalies
-
Holoprosencephaly
-
Cervical myelocystocele
-
Frontometaphyseal dysplasia
-
Juvenile distal spinal muscular dystrophy
Chiari II malformation has been reported in a newborn with in utero Zika virus exposure. [8]
Preferred examination
Chiari II malformation is a complex anomaly with skull, dural, brain, spinal, and spinal cord manifestations. Traditionally, when signs and symptoms were suggestive of a Chiari II malformation, plain radiography of the head and spine was performed, followed by myelography. Because myelography is an invasive procedure, clinicians were reluctant to perform the test until the severity of the symptoms warranted it.
The introduction of modern imaging techniques, specifically magnetic resonance imaging (MRI), has radically changed the evaluation of symptoms referable to the brain and spinal cord. MRI is usually used for the detailed evaluation of lesions and complications due to Chiari II malformations. MRI is best used to appreciate the full constellation of findings in Chiari II malformations, and it permits detailed visualization of the cerebellum and spinal cord. MRIs are useful in showing the low position of the cerebellar tissue and in determining whether associated spinal abnormalities, such as diastematomyelia or syringomyelia, are present. In addition, MRI has been used for the diagnosis of fetal craniospinal anomalies. MRI is widely available and accepted and easy to perform. It allows imaging in multiple planes, and it has high spatial and contrast resolution, which allows for the optimal evaluation of morphologic features. [9, 10, 11, 12, 13, 14, 15, 16, 17]
Chiari II malformations are also diagnosed with the help of both computed tomography (CT) scanning and ultrasonography. [17] CT scanning is especially useful after the neonatal period in following up obstructive hydrocephalus in infants who have undergone a ventriculoperitoneal shunt procedure. [18]
CT scanning is useful for appreciating the luckenschadel skull (see the image below), and this modality can be used to identify the other bony changes seen in the Chiari II malformation, such as the large foramen magnum, the flat floor of the posterior fossa, and the scalloping of the petrous pyramids. CT scanning is also excellent for assessing and following up ventricular size before and after shunt placement (approximately 80-90% of patients have hydrocephalus).
Deep scalloping between the bony septations that characterize the lacunar skull (luckenschadel) (arrows) are best appreciated on an axial computed tomography section, as in this patient with a Chiari II malformation.
Many of the typical abnormal Chiari malformation findings depicted on cranial CT scans and MRIs can also be demonstrated on cranial ultrasonograms. Ultrasonography is routinely used during gestation for screening purposes and in the neonatal period for diagnosis and follow-up of hydrocephalus. [19, 20]
Plain radiographs of the cervical spine, including flexion and extension views, can be used to assess any pathologic spinal movement. Depicted abnormalities include widening of the upper cervical spinal canal and incomplete bony arching of C1 in as many as 70% of cases with replacement by a periosteal band that contributes to neural compression. In addition, plain radiography is excellent for demonstrating scoliosis, segmentation errors, and lack of fusion of the dorsal laminae in the spine.
Digital subtraction angiography (DSA) can be helpful in excluding abnormal cases of Chiari II malformation that involve the vertebral artery before surgery. This procedure can be performed noninvasively by using MR angiography or CT angiography. MR angiography can be preferred, especially in infants and children, because of the associated radiation exposure with CT angiography.
Limitation of techniques
Plain radiographic findings of Chiari II malformation do not have diagnostic importance except for the bone abnormalities associated with scoliosis and diastematomyelia and for ventriculoperitoneal shunt malfunction.
CT scanning is an efficient diagnostic examination in following up infants and children with hydrocephalus, but it exposes the patient to ionizing radiation. The value of CT scanning in diagnosing cerebral gyral malformations and spinal cord pathology is limited.
MRI is relatively expensive, is contraindicated in patients with pacemakers, and is not tolerated by all patients. MRI requires patient cooperation or sedation.
Ultrasonography can be performed during the antenatal period as a screening method and in high-risk pregnancies; with a careful ultrasonographic examination, cranial and spinal pathologic changes related to Chiari II malformations in the fetus can be seen and diagnosed antenatally. [21] Ultrasonography is limited to the period before the closure of the anterior fontanelle, which serves as an acoustic window. Abnormalities such as gyral, dural, tentorial, and vermian anomalies accompanying Chiari II malformations are difficult to visualize with ultrasonography.
Reportedly, a lacunar skull can also be detected by using ultrasonography in the fetus. To confirm the diagnosis and gain detailed information, MRI can be used antenatally. In addition, MRI has been used as a diagnostic tool during the antenatal period, allowing the intrauterine diagnosis, and even treatment, of spina bifida.
Failure to diagnose a Chiari II malformation and its associated anomalies in a neonate or a child can cause serious brain and spinal complications; failure to identify early cranial and spinal cord lesions may result in delayed intervention and permanent neurologic deficit; and failure to make the correct diagnosis (eg, cerebellar tumor instead of Chiari II malformation) can cause morbidity and mortality resulting from surgery.
Radiography
Plain radiography has been used most frequently for examining bone anomalies, scoliosis, and ventriculoperitoneal shunt malfunction. Plain images can show enlargement of the cervical spinal canal and posterior midline fusion defects, as well as anterior bony abnormalities, such as C1 and C2 dislocation.
Routine radiography can demonstrate luckenschadel in neonates with myelodysplasia. Additional bony changes that can be seen include scalloping of the posterior surface of the petrous pyramids and the clivus.
Plain radiographs have diagnostic importance in the evaluation of cranial and vertebral bony abnormalities and in the evaluation of ventriculoperitoneal shunt disconnection or displacement of the shunt catheter.
Computed Tomography
CT scanning is the routine diagnostic method for following up patients with a Chiari II malformation and associated hydrocephalus. An encysted fourth ventricle is one of the causes of shunt malfunction. Because the internal regulation of the shunt valve is usually affected by intracranial pressure changes, the pressure dynamics between infratentorial and supratentorial compartments are important. CT scanning also is helpful for follow-up to assess the dynamic changes in the infratentorial and supratentorial ventricular systems.
Luckenschadel can be demonstrated on CT scans (see the image below). Abnormalities are composed of areas of thinning or pits within the calvarial bone. The areas of thinning typically occur on the inner surface of the skull, but they have been seen on both the inner and outer aspects. Within each of the depressions on the inner aspect of the skull, brain tissue can be seen bulging into the bony defect.
Deep scalloping between the bony septations that characterize the lacunar skull (luckenschadel) (arrows) are best appreciated on an axial computed tomography section, as in this patient with a Chiari II malformation.
CT scans may demonstrate an abnormally large foramen magnum, the flat floor of the posterior fossa, and scalloping of the petrous pyramids and clivus (see the following image). CT scanning also demonstrates tectal beaking, cerebellar tissue wrapping around the brainstem, fenestrations of the falx, manifestations of hydrocephalus, and shunt malfunction.
Axial computed tomography scan in a patient with a Chiari II malformation. This image shows a gaping, somewhat heart-shaped tentorial incisura (large arrowheads) that appears to be completely plugged with the upwardly herniating cerebellum. The cerebellar hemispheres extend anteromedially (small arrowheads) and almost completely engulf the brainstem. The petrous ridges are concave (arrows).
CT myelography is rarely performed in patients with Chiari II malformation because of the advent of MRI. High-resolution CT scanning of the spine may be essential for surgical planning, particularly in patients with severe scoliosis and associated complex segmentation anomalies.
Three-dimensional (3-D) CT scans and CT angiograms can be used for a precise analysis of complex osseous malformations, of the relationships between vascular and bony structures, and of postoperative changes in the bone (see the images below).
 Inferior operativelike view on 3-dimensional computed tomography scan. This image shows malrotation of the posterior arches of C1 (long arrow) and C2 (short arrow). Courtesy of Duffau et al.
Inferior operativelike view on 3-dimensional computed tomography scan. This image shows malrotation of the posterior arches of C1 (long arrow) and C2 (short arrow). Courtesy of Duffau et al.
 Postoperative 3-dimensional computed tomography scan. This image shows osseous decompression with a large opening of the foramen magnum and resection of the posterior arch of the atlas (arrows). Courtesy of Duffau et al.
Postoperative 3-dimensional computed tomography scan. This image shows osseous decompression with a large opening of the foramen magnum and resection of the posterior arch of the atlas (arrows). Courtesy of Duffau et al.
Degree of confidence
Chiari II malformation associated with subtle gyral malformations and spinal cord abnormalities, such as a syrinx, are often missed on routine CT images. Thin-section sagittal and/or coronal reformatted CT images may be useful for assessing spinal anomalies. The most common cause of a syrinx of the spinal cord in patients with a Chiari II malformation is ventriculoperitoneal shunt malfunction. All patients with a Chiari II malformation and syrinx (as detected with spinal MRI) should undergo cranial CT scanning and a radiographic shunt series to exclude shunt malfunction as a cause for appearance or worsening of the syrinx.
When posterior fossa and cervical CT scans are evaluated individually, the craniocaudal elongation of cerebellum in a Chiari II malformation can be confused with cervical spinal tumors and cerebellar tumors that ascend through foramen magnum or cause cerebellar herniation.
Magnetic Resonance Imaging
MRI provides studies of the altered anatomy and excellent images in all projections (sagittal, axial, coronal). The sagittal view is one of the most useful (see the following images). [14, 15, 16] Spin-echo T1-weighted sagittal and coronal images and T2-weighted sagittal images, including those of the cervical region, should be obtained. In the authors' department, sagittal images are obtained with 3- or 4-mm thickness and 1-mm gap, and axial and coronal scans are obtained with 5-mm thickness and 1- or 2-mm gap. Craniocervical magnetic resonance (MR) examination is performed in children with myelomeningocele, whereas spinal MR examination is performed in patients with a Chiari II malformation.
MRI is reliable and the best diagnostic method for distinguishing the differential diagnosis between Chiari II malformation and other craniocervical pathologies. Although the soft tissue can be evaluated easily with MRI, bone anomalies that can be depicted easily on plain radiographs and CT scans may be missed on MRI.
Sagittal T1-weighted magnetic resonance image of posterior fossa abnormalities in Chiari II malformation: (1) colpocephaly; (2) beaked tectum; (3) cascade of an inferiorly displaced vermis behind the medulla; (4) elongated, tubelike fourth ventricle; (5) low-lying torcular herophili; (6) cerebellar hemispheres wrapping around the brainstem anteriorly; (7) concave clivus; (8) medullary spur; and (9) medullary kink.
A thoracic-level myelomeningocele (short arrow) is seen in a patient with a Chiari II malformation (long arrow).
Sagittal T2-weighted magnetic resonance image in a patient with a Chiari II malformation. This image shows a thoracic-level myelomeningocele (arrows). The spinal cord, in addition to the thoracic placode, also extends distally and is further tethered at the sacral level.
Hindbrain anomalies, hydrocephalus, and syrinx cavities in the spinal cord are well demonstrated on T1-weighted images. The extent of the S-shaped medullary kink can be easily evaluated by using sagittal MRI in patients with a Chiari II malformation (see the first 2 images below). MRI of the head is easily performed to assess the size and position of the ventricles, and it provides important additional information (see the first and third images below).
Sagittal T1-weighted magnetic resonance image of posterior fossa abnormalities in Chiari II malformation: (1) colpocephaly; (2) beaked tectum; (3) cascade of an inferiorly displaced vermis behind the medulla; (4) elongated, tubelike fourth ventricle; (5) low-lying torcular herophili; (6) cerebellar hemispheres wrapping around the brainstem anteriorly; (7) concave clivus; (8) medullary spur; and (9) medullary kink.
Sagittal midline T1-weighted magnetic resonance image in a patient with a Chiari II malformation. This image shows a large massa intermedia (long arrow) and a beaked tectum (short arrow). Other posterior fossa abnormalities are also seen in this patient.
Axial T1-weighted magnetic resonance image in a patient with a Chiari malformation. This image shows a beaked tectum (arrows) and colpocephaly (arrowheads).
Enlargement of the massa intermedia, occlusion of the cerebral aqueduct, and beaking of the tectum are best evaluated by using a sagittal projection on MRI (as shown in the images below). Gyral interdigitation, cerebral gyral anomalies, an engulfed brainstem, and the level of the medullary kink can easily be evaluated by using axial MRI.
Sagittal T1-weighted magnetic resonance image of posterior fossa abnormalities in Chiari II malformation: (1) colpocephaly; (2) beaked tectum; (3) cascade of an inferiorly displaced vermis behind the medulla; (4) elongated, tubelike fourth ventricle; (5) low-lying torcular herophili; (6) cerebellar hemispheres wrapping around the brainstem anteriorly; (7) concave clivus; (8) medullary spur; and (9) medullary kink.
Sagittal midline T1-weighted magnetic resonance image in a patient with a Chiari II malformation. This image shows a large massa intermedia (long arrow) and a beaked tectum (short arrow). Other posterior fossa abnormalities are also seen in this patient.
MRI enables accurate, objective, and detailed identification of spinal cord and vertebral abnormalities, including syringomyelia and diastematomyelia, both preoperatively and postoperatively (see the following images. The ultrasonogram is from the same patient as the first 2 images below). MRI has also been used as a diagnostic tool during the antenatal period, allowing the intrauterine diagnosis, and even treatment, of spina bifida.
A thoracic-level myelomeningocele (short arrow) is seen in a patient with a Chiari II malformation (long arrow).
Sagittal T2-weighted magnetic resonance image in a patient with a Chiari II malformation. This image shows a thoracic-level myelomeningocele (arrows). The spinal cord, in addition to the thoracic placode, also extends distally and is further tethered at the sacral level.
Sagittal ultrasonogram in a patient with a Chiari II malformation. This image shows the thoracic spinal cord (arrowheads) and myelomeningocele (arrows). Note the tethering of the placode at the site of the dysraphic defect.
Herweh et al demonstrated a strong correlation between both size and fractional anisotropy of the corpus callosum in which callosal fractional anisotropy was significantly reduced, as was the corpus callosum area. [22] Anterior commissure thickness, however, was significantly increased and associated with a higher fractional anisotropy. The investigators compared 6 patients who had Chiari II malformation with 6 healthy patients to identify damage to the corpus callosum and anterior commissure with the use of T1-weighted 3-D imaging and diffusion tensor imaging. In determining fractional anisotropy and the cross-sectional area of the corpus callosum and anterior commissure, Herweh found that 4 of the Chiari II patients had hydrocephalus, 2 had callosal dysplasia, and 4 had hypoplastic corpus callosum. [22] According to the authors, the study findings pointed to white-matter damage in addition to that caused by hydrocephalus. [22]
Shrot et al studied the use of diffusion-weighted imaging to evaluate infratentorial and supratentorial brain in fetuses with Chiari II malformation. MRI and US studies of 26 fetuses with Chiari II malformation and 15 controls were evaluated for the presence/severity of hydrocephalus, myelomeningocele level, and brain apparent diffusion coefficient (ADC) values, along with cerebral flow impedance parameters (resistance and pulsatile indexes, resistance index [RI], and pulsatility index [PI] respectively) from fetal ultrasound. Abnormal ADC values indicated supratentorial microstructural changes in fetuses with Chiari II malformation. Of the fetuses with Chiari II, 16 of 26 had hydrocephalus. There was increasing severity of lateral ventriculomegaly in the high spinal dysraphism subgroup compared to the low spinal dysraphism subgroup. Compared to controls, the Chiari II fetuses had significantly lower ADC values in the frontal (P=0.01) and temporal lobes (P=0.05), regardless of the presence or severity of hydrocephalus. Fetuses with Chiari II had significantly lower RI and PI values. [17]
Ultrasonography
Original reports discuss the limited use of ultrasonography in patients with hydrocephalus and congenital cerebral anomalies, but current applications greatly expand the role of this modality in the evaluation of the developing central nervous system. [23, 24] Many of the typical findings described with the use of cranial CT scans and MRIs can also be demonstrated on the cranial ultrasonograms. [15]
Commercially available equipment is used with a 3- to 7.5-MHz transducer, depending on the size of the patient's head. In newborns, 5- to 7.5-MHz transducers are used, and 3- to 5-MHz transducers are used in older infants. Scans obtained with the transfontanel approach or with the transducer placed directly over the cervical region can demonstrate the downward displacement of the vermis and the medullary kink.
Ultrasonography is suited especially for evaluating the ventricular system in patients with a Chiari II malformation. The lateral ventricles often take on a characteristic pointed appearance that is best demonstrated in the coronal projection. In addition, the lateral ventricles are frequently asymmetric, and they may appear colpocephalic, such that the cerebral mantle appears thinnest over the occipital horns (see the image below). The choroid plexus of the lateral ventricle can be demonstrated best by using sagittal ultrasonographic sections; it is unusually prominent and has been described as having a drumstick configuration or dangling choroid.
Ultrasonography is heavily operator dependent. Findings associated with the Chiari II malformation, such as pachygyria, polymicrogyria, heterotopias, and dural abnormalities, may be missed with the use of this modality.
Sagittal midline ultrasonogram shows a large massa intermedia (long arrow) and a beaked tectum (short arrow). This image also shows obliteration of the cisterna magna and the fourth ventricle, as well as compression of the pons and brainstem.
The characteristic prominence of the massa intermedia and beaked tectum that are often associated with the Chiari II malformation are also visible (see the previous image). The enlarged massa intermedia may appear to fill the third ventricle. A prominent anterior commissure, herniation of the third ventricle into the suprasellar cistern, and an enlarged suprapineal recess are often seen on midline sagittal sections. Dysgenesis of the hindbrain with downward displacement and elongation of the fourth ventricle, medulla, and the cerebellum results in a relatively small-appearing posterior fossa (see the previous image).
Callen et al demonstrated that tectal abnormalities were not only seen equally well in fetuses before and after 24 weeks, but they were also seen more frequently as the severity of posterior fossa findings increased. [23] The authors suggested that such findings may be useful as a supratentorial indicator of both the presence and, potentially, the severity of Chiari II malformations. [23] The study involved retrospectively reviewing fetal intracranial findings of 89 fetuses, with ultrasonographically detected myelomeningocele to identify abnormalities in tectal morphologic characteristics ("beaking" of the tectum). Of the 89 cases, 59 (66%) had an abnormal tectal shape. [23]
In the neonatal period, spinal ultrasonography can be performed by using areas of dysraphism as an acoustic window. In this way, spinal abnormalities in patients with Chiari II malformation can be detected (see the following image).
Sagittal ultrasonogram in a patient with a Chiari II malformation. This image shows the thoracic spinal cord (arrowheads) and myelomeningocele (arrows). Note the tethering of the placode at the site of the dysraphic defect.
Ultrasonography is routinely used during the antenatal period as a screening method. With careful examination, cranial and spinal pathologic changes related to Chiari II malformations in the fetus can be seen. Reportedly, a lacunar skull can be detected with the use of this modality in the fetus.
According to Wong et al, interhemispheric cysts (protrusion of the posterior superior third ventricle) are a common supratentorial feature of Chiari II malformation, but their presence appears to be unrelated to other features of Chiari II malformation. [24] The authors thus suggest that, although interhemispheric cysts are seen in other abnormal fetuses, their striking prevalence in the Chiari II malformation should lead to a thorough examination for myelomeningocele. In their study, 43% of fetuses diagnosed with myelomeningocele had an interhemispheric cyst. Among fetuses without a central nervous system anomaly, no interhemispheric cysts were detected, but a cyst was detected in 1 of 10 fetuses with ventriculomegaly. [24]
Intraoperative ultrasonography is used for surgical purposes, especially lateral ventricular shunt tube placement in infants, and for aiding in the intraoperative placement of catheters into cavities in the syrinx.
-
A thoracic-level myelomeningocele (short arrow) is seen in a patient with a Chiari II malformation (long arrow).
-
Sagittal T2-weighted magnetic resonance image in a patient with a Chiari II malformation. This image shows a thoracic-level myelomeningocele (arrows). The spinal cord, in addition to the thoracic placode, also extends distally and is further tethered at the sacral level.
-
Sagittal ultrasonogram in a patient with a Chiari II malformation. This image shows the thoracic spinal cord (arrowheads) and myelomeningocele (arrows). Note the tethering of the placode at the site of the dysraphic defect.
-
Sagittal T1-weighted magnetic resonance image of posterior fossa abnormalities in Chiari II malformation: (1) colpocephaly; (2) beaked tectum; (3) cascade of an inferiorly displaced vermis behind the medulla; (4) elongated, tubelike fourth ventricle; (5) low-lying torcular herophili; (6) cerebellar hemispheres wrapping around the brainstem anteriorly; (7) concave clivus; (8) medullary spur; and (9) medullary kink.
-
Axial computed tomography scan in a patient with a Chiari II malformation. This image shows a gaping, somewhat heart-shaped tentorial incisura (large arrowheads) that appears to be completely plugged with the upwardly herniating cerebellum. The cerebellar hemispheres extend anteromedially (small arrowheads) and almost completely engulf the brainstem. The petrous ridges are concave (arrows).
-
Sagittal midline T1-weighted magnetic resonance image in a patient with a Chiari II malformation. This image shows a large massa intermedia (long arrow) and a beaked tectum (short arrow). Other posterior fossa abnormalities are also seen in this patient.
-
Sagittal midline ultrasonogram shows a large massa intermedia (long arrow) and a beaked tectum (short arrow). This image also shows obliteration of the cisterna magna and the fourth ventricle, as well as compression of the pons and brainstem.
-
Coronal T1-weighted magnetic resonance image in a patient with a Chiari II malformation. This image shows low-lying transverse sinuses (arrows), hydrocephalus, and a small posterior fossa. A hypoplastic tentorium cerebelli with gaping incisura (arrowhead) is present with a towering cerebellum (small arrows).
-
Axial T1-weighted magnetic resonance image in a patient with a Chiari malformation. This image shows a beaked tectum (arrows) and colpocephaly (arrowheads).
-
Axial T2-weighted magnetic resonance image in a patient with a Chiari II malformation. This image shows a hypoplastic fenestrated falx cerebri with striking interdigitation of the gyri (arrows).
-
Deep scalloping between the bony septations that characterize the lacunar skull (luckenschadel) (arrows) are best appreciated on an axial computed tomography section, as in this patient with a Chiari II malformation.
-
Inferior operativelike view on 3-dimensional computed tomography scan. This image shows malrotation of the posterior arches of C1 (long arrow) and C2 (short arrow). Courtesy of Duffau et al.
-
Postoperative 3-dimensional computed tomography scan. This image shows osseous decompression with a large opening of the foramen magnum and resection of the posterior arch of the atlas (arrows). Courtesy of Duffau et al.
-
Antenatal magnetic resonance image shows a Chiari II malformation in a fetus. Courtesy of Umit Aksoy, MD, Uludag University, Bursa, Turkey.
-
This T1-weighted axial magnetic resonance image demonstrates heart-shaped incisura and a petrous ridge in a patient with a Chiari II malformation.






