Practice Essentials
The term cecal volvulus is a misnomer because, in most patients with cecal volvulus, the torsion is located in the ascending colon above the ileocecal valve. In general, a partial malrotation is necessary for cecal volvulus to occur, because the cecum and parts of the ascending colon are involved. Early diagnosis is essential to reduce the high mortality rate reported with this condition, which is essentially a closed-loop obstruction that may lead to vascular compromise with consequent gangrene and perforation. [1, 2, 3]
Patients with a cecal volvulus will usually present with both small bowel and large bowel obstructions, with collapse of the distal large bowel and extensive dilatation of the proximal small bowel. According to studies, a definitive sign of a cecal volvulus is upward displacement of the appendix and obstruction of the large bowel. [2]
The diagnosis is mostly based on plain abdominal radiographic findings aided by those of single-contrast barium enema examination (see the following images). Computed tomography (CT) scanning is useful in identifying signs of ischemia, which include mural thickening, infiltration of the mesenteric fat, and pneumatosis intestinalis. Abdominopelvic CT scanning has been reported to be diagnostic for a cecal volvulus in about 90% of cases, and 10% are diagnosed intraoperatively. [2, 4] Treatment is surgical, but reduction of the volvulus has been reported after barium enema examination. Colonoscopy may be considered for the purpose of decompression. [5, 6, 7, 8, 9]
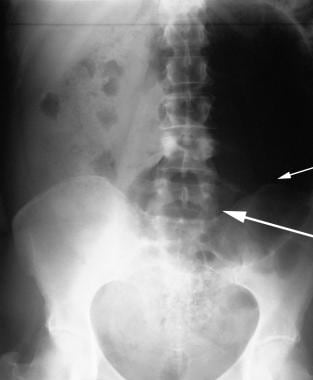
 Plain supine abdominal radiograph from an 81-year-old man presenting with abdominal pain and vomiting. The radiograph shows a markedly distended loop of bowel 15-cm in diameter with its axis running from the right lower quadrant to the mid abdomen. This loop of bowel represent a twisted cecum with the caput cecum directed medially (arrows). The haustra within the cecum (C) are effaced. Note the proximal dilated loop of small bowel. The distal colon shows little if any air. At surgery a cecal volvulus was confirmed.
Plain supine abdominal radiograph from an 81-year-old man presenting with abdominal pain and vomiting. The radiograph shows a markedly distended loop of bowel 15-cm in diameter with its axis running from the right lower quadrant to the mid abdomen. This loop of bowel represent a twisted cecum with the caput cecum directed medially (arrows). The haustra within the cecum (C) are effaced. Note the proximal dilated loop of small bowel. The distal colon shows little if any air. At surgery a cecal volvulus was confirmed.
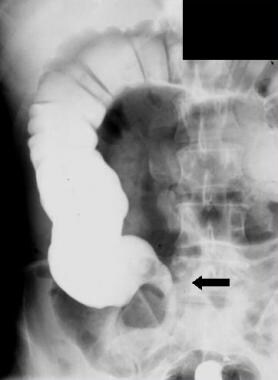
 Right oblique image from a barium enema examination in from a 53-year-old woman who presented with clinical features of intestinal obstruction. This image shows a bird-beak appearance (arrow). At surgery, a cecal volvulus was confirmed.
Right oblique image from a barium enema examination in from a 53-year-old woman who presented with clinical features of intestinal obstruction. This image shows a bird-beak appearance (arrow). At surgery, a cecal volvulus was confirmed.
Wolfer et al described defective peritoneal fixation of the ascending colon and cecum in 10% of the population. [10] This fixation permits abnormal mobility of the ascending colon and cecum, making displacement of the right colon into any part of the abdominal cavity possible. Depending on the length of the mobile ascending colon, a variety of obstructive bowel patterns may result. Many authors have described an association with adhesions, membranes, and bands, which may provide a nodal point around which the mobile ascending colon may twist. Although these conditions are frequently present, they are not essential for a volvulus to occur.
Many studies of cecal volvulus have focused on the possibility of volvulus of the right colon occurring in association with obstructive lesions, usually in the left colon. [11] The most common distal colonic lesions associated with cecal volvulus are colonic carcinoma and diverticulitis.
Imaging modalities
The preferred examinations are plain abdominal radiography, barium enema examination (usually with a single contrast agent), and CT scanning. [5, 12] Bowel gas patterns on a plain abdominal radiograph may not be characteristic, because the right colon and/or cecum may be displaced to any part of the abdominal cavity. A redundant looplike cecal volvulus may be confused with a sigmoid volvulus. In the presence of a closed-loop obstruction of the colon, evaluation of the 2 sites of obstruction may not be possible with barium enema examination. [13, 14, 15, 16, 3]
Signs of cecal volvulus on CT include the whirl sign, abnormal cecal position, bird-beak sign, severe cecal distention, mesenteric engorgement, and the central appendix sign (defined as abnormal appendix position near midline). [4, 17, 18]
Sigmoid volvulus is part of the differential diagnosis. Other conditions to be considered are a distended stomach from high gastrointestinal obstruction or gastroparesis, other forms of large bowel obstruction, and a giant sigmoid diverticulum.
An attempt should always be made to reduce the volvulus with barium enema examination, unless contraindications are present. Reduction with barium enema examination is particularly successful in the rare cecal volvulus that occurs in the postpartum patient. The volvulus may reduce during evacuation of the contrast agent. However, surgery is required in many patients and is urgent after reduction in those with gross abdominal tenderness or in those in whom leukocytosis suggests ischemia.
The postoperative abdomen, especially after closed segmental resection of the descending colon, presumably with stenosis, is a precipitating cause of cecal volvulus. After colonic resection and anastomosis, evaluation of the colon with a barium enema is undesirable, no matter how carefully the procedure is performed. Evaluation with water-soluble contrast material has been used to evaluate the postoperative colon. The safety of this procedure in the postoperative abdomen cannot yet be determined because experience is limited.
The contraindications for a barium enema are signs and symptoms of peritonitis, rectal bleeding, radiographic signs of gas in the bowel wall, and pneumoperitoneum.
Overdistention of the cecum with air and/or barium during a barium enema examination may result in cecal perforation. Delay in surgical treatment in the presence of increasing cecal distention can also result in cecal perforation.
Types of cecal volvulus
Two types of cecal volvulus are described: axial torsion type and the cecal bascule type. In practice, differentiation between the 2 types is not clinically important, because the clinical presentation and treatment are the same. However, the radiographic appearances are different, and recognition of these differences is important for diagnosis.
Axial torsion, the most common form of volvulus, occurs with the development of a twist of 180-360o; along the longitudinal axis of the ascending colon. This form is associated with a high mortality, because the obstructive process is associated with vascular compromise, which can lead to gangrene and perforation, often on the antimesenteric border, where the ischemic changes may be most pronounced.
In the cecal bascule type of volvulus, the cecum folds anteromedial to the ascending colon, with the production of a flap-valve occlusion at the site of flexion. This form of torsion occurs in a transverse plane and is associated with marked distention of the cecum, which is often displaced into the center of the abdomen. As many as one third of the patients with cecal volvulus have this variety, and reduction of cecal bascule after barium enema examination is reported. With a cecal bascule, the ileum may passively twist with the cecum and not be obstructed. A constant feature of cecal bascule is the presence of a constricting band across the ascending colon; this may be found at laparotomy. [19]
Anatomy
Occasionally, diaphragmatic interposition of the right colon (Chilaiditi syndrome) occurs. This is related to redundancy of bowel rather than defective fixation. The right side of the colon may have a defective fixation and abnormal mobility; therefore, it may be located anywhere in the abdomen, including beneath the right hemidiaphragm. This motility may allow the right side of the colon and cecum to herniate into the inguinal and femoral canals. Most of these abnormalities of fixation can be diagnosed radiologically. The most important complication of the abnormalities of fixation is a volvulus of the right side of the colon and/or cecum.
Radiography
The plain abdominal radiograph is usually the key to the diagnosis of cecal volvulus. In axial torsion, the image may show a markedly distended loop of large bowel, with its long axis extending from the right lower quadrant to the epigastrium or left upper quadrant, the most common site to which the cecum is displaced (see the image below). Depending on the initial bowel position and the length of mobile right colon, the distended cecum may be seen anywhere in the abdomen.
Plain supine abdominal radiograph from an 81-year-old man presenting with abdominal pain and vomiting. The radiograph shows a markedly distended loop of bowel 15-cm in diameter with its axis running from the right lower quadrant to the mid abdomen. This loop of bowel represent a twisted cecum with the caput cecum directed medially (arrows). The haustra within the cecum (C) are effaced. Note the proximal dilated loop of small bowel. The distal colon shows little if any air. At surgery a cecal volvulus was confirmed.
Despite the varying positions of the distended cecum, the plain radiographic features of a cecal volvulus are characteristic, and the caput cecum can typically be identified (see the first image below). The colonic haustral pattern is generally maintained, although some effacement may be present if superimposed ischemia is present. When shorter segments of the colon and cecum are involved, the distended cecum may be found in the normal location (see the second image below).
 A 53-year-old woman presented with clinical features of intestinal obstruction. This plain supine radiograph was performed on the day of admission. It shows a large air-filled viscus (15 cm in diameter), with the axis running from the mid abdomen to the left hypochondrium. No haustra are seen in the air-filled viscus (short arrow). Note that the right iliac fossa is empty (long arrow), but formed feces intermingled with air are noted in part of the ascending colon. The air can be traced up to the rectum. At this stage, no firm radiologic diagnosis was entertained, although the working clinical diagnosis was partial bowel obstruction.
A 53-year-old woman presented with clinical features of intestinal obstruction. This plain supine radiograph was performed on the day of admission. It shows a large air-filled viscus (15 cm in diameter), with the axis running from the mid abdomen to the left hypochondrium. No haustra are seen in the air-filled viscus (short arrow). Note that the right iliac fossa is empty (long arrow), but formed feces intermingled with air are noted in part of the ascending colon. The air can be traced up to the rectum. At this stage, no firm radiologic diagnosis was entertained, although the working clinical diagnosis was partial bowel obstruction.
 This plain supine radiograph was obtained 24 hours after the radiograph in the previous image (from a 53-year-old woman who presented with clinical features of intestinal obstruction). The position of the air filled viscus has changed and suggests that the air-filled viscus is mobile. The viscus now looks much more like a cecum. The caput cecum is directed toward the right iliac fossa. The twist is outlined by air (arrows).
This plain supine radiograph was obtained 24 hours after the radiograph in the previous image (from a 53-year-old woman who presented with clinical features of intestinal obstruction). The position of the air filled viscus has changed and suggests that the air-filled viscus is mobile. The viscus now looks much more like a cecum. The caput cecum is directed toward the right iliac fossa. The twist is outlined by air (arrows).
In most patients, obstruction is almost complete; thus, the distal colon is usually empty and the small bowel is frequently distended. Occasionally, a long-axis torsion may be associated with signs of incomplete obstruction. Rarely, small-bowel loops are identified to the right of the distended cecum and ascending colon. The ileocecal valve may possibly be identified, and on occasion, the point of torsion may be outlined by gas, as an area of conelike narrowing.
In the cecal bascule form of volvulus, the distended air-filled cecum is located more centrally. With this variant, the ileum can passively twist with the cecum, and small bowel is not obstructed. If the appendix is filled with gas and in an unusual location attached to a distended cecum, the diagnosis can be made readily.
Single contrast barium enema examination is generally adequate for the evaluation of cecal volvulus. A double-contrast barium enema study does not confer any significant advantage, because no fine detail is necessary to make the diagnosis. The administration of glucagon is often necessary, because patients may have considerable colonic spasm and find it difficult to retain the contrast agent.
The barium enema study shows a nondilated distal colon to the point of twist (see the following images). If the obstruction is not complete, some barium may trickle past the site of obstruction, and the twist may be visualized in more detail. If the twist occurs along the transverse axis, the obstruction appears relatively smooth, and no spiral twist is usually seen. In a cecal bascule, a rounded termination of the barium column may be seen. This, when seen near a distended gas-filled viscus, should alert the radiologist to the diagnosis of a volvulus.
 This unprepared barium enema examination was obtained 12 hours after the first supine plain radiograph from a 53-year-old woman who presented with clinical features of intestinal obstruction. The image shows a nondilated colon. The barium-filled colon can be traced back to the right iliac fossa where there is a bird-beak cutoff (solid arrow). The dilated cecum lies in the epigastrium where there is an air fluid level (open arrow). Note that the barium has not entered the cecum.
Right oblique image from a barium enema examination in from a 53-year-old woman who presented with clinical features of intestinal obstruction. This image shows a bird-beak appearance (arrow). At surgery, a cecal volvulus was confirmed.
This unprepared barium enema examination was obtained 12 hours after the first supine plain radiograph from a 53-year-old woman who presented with clinical features of intestinal obstruction. The image shows a nondilated colon. The barium-filled colon can be traced back to the right iliac fossa where there is a bird-beak cutoff (solid arrow). The dilated cecum lies in the epigastrium where there is an air fluid level (open arrow). Note that the barium has not entered the cecum.
Right oblique image from a barium enema examination in from a 53-year-old woman who presented with clinical features of intestinal obstruction. This image shows a bird-beak appearance (arrow). At surgery, a cecal volvulus was confirmed.
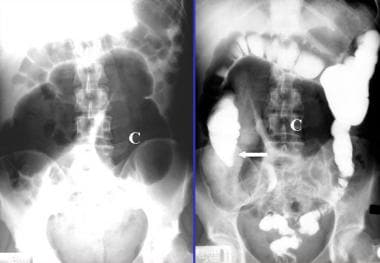 Left: Plain abdominal radiograph from a 48-year-old woman showing a massively distended and medially displaced proximal ascending colon and cecum. The cecal pole is now lying in the left upper abdominal quadrant (C). At least 2 or 3 haustrations are seen in the distended large bowel, which is consistent with cecal volvulus. No air fluid levels were demonstrated in this case. Right: A single contrast barium study of the same patient showing free barium flow through the sigmoid colon in to the mid ascending colon. The proximal ascending colon and the cecum are void of barium due to obstruction at the level of the mid-ascending colon.
Left: Plain abdominal radiograph from a 48-year-old woman showing a massively distended and medially displaced proximal ascending colon and cecum. The cecal pole is now lying in the left upper abdominal quadrant (C). At least 2 or 3 haustrations are seen in the distended large bowel, which is consistent with cecal volvulus. No air fluid levels were demonstrated in this case. Right: A single contrast barium study of the same patient showing free barium flow through the sigmoid colon in to the mid ascending colon. The proximal ascending colon and the cecum are void of barium due to obstruction at the level of the mid-ascending colon.
 A post-evacuation film from the same 48-year-old patient as in the previous image. This image shows a medially pointed end column of the barium (beak sign) in the mid-ascending colon. Distally, the large bowel is distended with gas and represents the cecal volvulus.
A post-evacuation film from the same 48-year-old patient as in the previous image. This image shows a medially pointed end column of the barium (beak sign) in the mid-ascending colon. Distally, the large bowel is distended with gas and represents the cecal volvulus.
As little barium as possible should be allowed to flow proximal to the site of obstruction, because flooding the bowel proximal to the obstruction site might precipitate a complete obstruction. When the barium enema is administered, overdistention should also be avoided, because this can lead to perforation. An attempt should always be made to reduce the volvulus. This reduction may be achieved during colonic filling by barium, but reduction occasionally occurs during barium evacuation. With an intermittent volvulus, the barium enema results may be normal, but a postevacuation radiograph may reveal the twist. [19, 20]
Plain radiographic findings can be diagnostic of a cecal volvulus in most patients. In others, the findings on the plain images only suggest the diagnosis, and barium enema examination is necessary to confirm the diagnosis.
Rarely, the dilated displaced cecum and ascending colon in the left upper quadrant may be confused with a normal or abnormally distended stomach. A redundant looplike cecal volvulus may be confused with a sigmoid volvulus. In the presence of a double obstruction of the colon (left colon obstruction associated with a cecal volvulus), evaluation of the right colon may not be possible, and the diagnosis of volvulus must be based on plain radiographic findings alone.
Computed Tomography
CT scans demonstrate a mechanical intestinal obstruction, show the site of obstruction and its severity, and can be used to differentiate between mechanical obstruction and adynamic ileus. A volvulus or strangulation generally causes a closed-loop obstruction, and CT scans characteristically demonstrate a U-shaped distended bowel segment and signs of ischemia. These signs include mural thickening, infiltration of the mesenteric fat, and pneumatosis intestinalis. In the presence of a cecal or sigmoid volvulus, a whirl sign may be apparent because of a tight torsion of the mesentery that is caused by a twist between the afferent and efferent loops. [6, 7, 8, 13] A "coffee bean" appearance in a loop of transverse colon and an abrupt cut-off with “bird's beak” tapering at the distal cecum are 2 other characteristic findings for cecal volvulus. [21, 22]
Several studies have shown the superiority of CT scanning compared with plain abdominal radiography in the diagnosis of intestinal obstruction. However, the use of CT scanning remains controversial. The present consensus is that abdominal CT scanning should be performed in the presence of mechanical intestinal obstruction when the plain radiographic and clinical examination findings are inconclusive, especially in patients in whom the identification of the cause of obstruction may affect treatment.
The whirl sign on CT scans is not specific for cecal volvulus and may also occur in other types of volvulus, including sigmoid volvulus. [6]
Acute colonic pseudo-obstruction (ACPO) has a similar presentation to cecal volvulus, and cross-sectional imaging with CT can be used to differentiate between them. ACPO findings include colonic dilatation with possible transition zone and no obvious mechanical cause of the obstruction. [23]
The detection of a transitional zone between the dilated proximal bowel loops and collapsed distal loops distal to the obstructed site is important in diagnosing bowel obstruction on CT scans. However, a false-negative diagnosis may occur in a mixed type of ileus or in a mild partial obstruction. A false-positive diagnosis of intestinal obstruction may be made when a distended air-filled right colon is seen in the presence of a collapsed left colon.
Ultrasonography
Ultrasonography is usually the first modality used in the emergency department to investigate an acute abdomen. Cecal volvulus is usually associated with a small-bowel obstruction. The small-bowel loops are distended with fluid, and to-and-fro peristalsis is often visible. Cecal volvulus may be depicted as a grossly distended fluid-filled cecum at a lead point of small-bowel obstruction, but the appearances are generally nonspecific. [9]
Ultrasonograms may suggest a diagnosis or indicate a more appropriate investigation for diagnosis. However, ultrasonography is not a sensitive technique in the workup of a cecal volvulus.
-
Plain supine abdominal radiograph from an 81-year-old man presenting with abdominal pain and vomiting. The radiograph shows a markedly distended loop of bowel 15-cm in diameter with its axis running from the right lower quadrant to the mid abdomen. This loop of bowel represent a twisted cecum with the caput cecum directed medially (arrows). The haustra within the cecum (C) are effaced. Note the proximal dilated loop of small bowel. The distal colon shows little if any air. At surgery a cecal volvulus was confirmed.
-
A 53-year-old woman presented with clinical features of intestinal obstruction. This plain supine radiograph was performed on the day of admission. It shows a large air-filled viscus (15 cm in diameter), with the axis running from the mid abdomen to the left hypochondrium. No haustra are seen in the air-filled viscus (short arrow). Note that the right iliac fossa is empty (long arrow), but formed feces intermingled with air are noted in part of the ascending colon. The air can be traced up to the rectum. At this stage, no firm radiologic diagnosis was entertained, although the working clinical diagnosis was partial bowel obstruction.
-
This plain supine radiograph was obtained 24 hours after the radiograph in the previous image (from a 53-year-old woman who presented with clinical features of intestinal obstruction). The position of the air filled viscus has changed and suggests that the air-filled viscus is mobile. The viscus now looks much more like a cecum. The caput cecum is directed toward the right iliac fossa. The twist is outlined by air (arrows).
-
This unprepared barium enema examination was obtained 12 hours after the first supine plain radiograph from a 53-year-old woman who presented with clinical features of intestinal obstruction. The image shows a nondilated colon. The barium-filled colon can be traced back to the right iliac fossa where there is a bird-beak cutoff (solid arrow). The dilated cecum lies in the epigastrium where there is an air fluid level (open arrow). Note that the barium has not entered the cecum.
-
Right oblique image from a barium enema examination in from a 53-year-old woman who presented with clinical features of intestinal obstruction. This image shows a bird-beak appearance (arrow). At surgery, a cecal volvulus was confirmed.
-
Left: Plain abdominal radiograph from a 48-year-old woman showing a massively distended and medially displaced proximal ascending colon and cecum. The cecal pole is now lying in the left upper abdominal quadrant (C). At least 2 or 3 haustrations are seen in the distended large bowel, which is consistent with cecal volvulus. No air fluid levels were demonstrated in this case. Right: A single contrast barium study of the same patient showing free barium flow through the sigmoid colon in to the mid ascending colon. The proximal ascending colon and the cecum are void of barium due to obstruction at the level of the mid-ascending colon.
-
A post-evacuation film from the same 48-year-old patient as in the previous image. This image shows a medially pointed end column of the barium (beak sign) in the mid-ascending colon. Distally, the large bowel is distended with gas and represents the cecal volvulus.


