Practice Essentials
The World Health Organization (WHO) has defined dilated cardiomyopathy as a condition in which the ventricular chambers exhibit increased diastolic and systolic volume and a low (< 40%) ejection fraction. [1, 2, 3] In the WHO/International Society and Federation of Cardiology classification, dilated cardiomyopathy in its primary (eg, idiopathic or familial) and secondary forms is the most common cause of the clinical syndrome of chronic heart failure. Dilated cardiomyopathy is the most common form of childhood cardiomyopathy and causes significant morbidity and mortality. [4]
In most cases, dilated cardiomyopathy is progressive, leading to heart failure and death. Without a transplant, survival rates are poor. Continued enlargement of the ventricles leads to a decline in ventricular function, followed by conduction system abnormalities, ventricular arrhythmias, thromboembolism, and heart failure. [5, 4, 6]
The prevalence of heart failure is approximately 1-1.5% in the adult population of Western countries. Dilated cardiomyopathy is associated with a large number of systemic or cardiac diseases, including specific heart muscle diseases (eg, ischemic cardiomyopathy, diabetic cardiomyopathy, alcoholic cardiomyopathy).
Dilated cardiomyopathy constitutes approximately 90% of all cardiomyopathies. An estimated 30% of dilated cardiomyopathy cases have a genetic cause. Mutations in several genes have been linked to dilated cardiomyopathy, including genes encoding structural components of the sarcomere and desmosome. Nongenetic causes include inflammation of the myocardium due to an infection (mostly viral); exposure to drugs, toxins or allergens; and systemic endocrine or autoimmune diseases. Approximately 25% of all cases of dilated cardiomyopathy are of unknown etiology. Cardiac resynchronization therapy and implantable cardioverter-defibrillators may be required to prevent life-threatening arrhythmias. [7, 8, 6]
Despite improved treatment, the mortality for dilated cardiomyopathy remains high, with a median period of survival of 1.7 years for men and 3.2 years for women. The annual incidence of sudden cardiac death is 2-4% and may be the initial presentation of dilated cardiomyopathy. [9] The natural history of the condition is progressive, and its cost, disability, and morbidity are among the highest of any disease. [10, 11, 12]
(See the dilated cardiomyopathy mages below.)
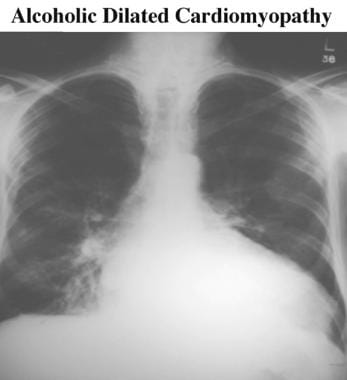 Chest radiograph shows a large heart. Image does not provide any clue to the etiology of the dilated cardiomyopathy; however, the healing rib fractures and right lower lobe pneumonia (aspiration pneumonia) suggest alcoholic cardiomyopathy as the cause.
Chest radiograph shows a large heart. Image does not provide any clue to the etiology of the dilated cardiomyopathy; however, the healing rib fractures and right lower lobe pneumonia (aspiration pneumonia) suggest alcoholic cardiomyopathy as the cause.
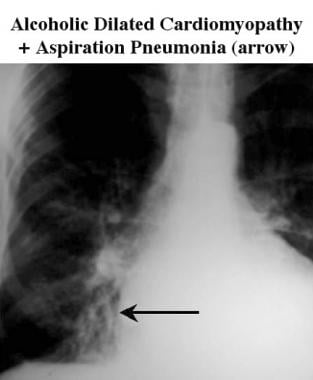 Magnified right chest radiograph shows an area of right lower lobe aspiration pneumonia in a patient with dilated cardiomyopathy (same patient as in the previous image).
Magnified right chest radiograph shows an area of right lower lobe aspiration pneumonia in a patient with dilated cardiomyopathy (same patient as in the previous image).
Imaging modalities
Currently available radiologic investigations are as varied in technique and sophistication as they are in cost. Studies vary from the noninvasive to the invasive and from the dynamic to the static. Radiologic tests are used to help make a diagnosis, to assess the degree of cardiac dysfunction, to identify a cause (though this is unusual), and to guide therapy. [13]
It is difficult to make an accurate clinical identification of heart failure resulting from poor ventricular function, but it is important to do so because of the need to relieve symptoms. A substantial number of patients with heart failure have normal ECG results. [14] In other patients with apparent heart failure, echocardiography provides extra information on the nature of the cardiac disease that affects management. [15] In addition, providing appropriate treatment is important in patients affected more severely (ejection fraction < 35-40%), in whom treatment can significantly reduce mortality. [16, 17, 18]
In a study by Merlo et al of 414 patients with dilated cardiomyopathy who underwent ECG testing, 55 patients experienced death or heart transplant and 57 patients experienced sudden death or malignant ventricular arrhythmias during a 125-month follow-up period. Left ventricular hypertrophy, heart rate, and anterolateral T-wave inversion predicted death or heart transplant. S wave amplitude in V2, R wave amplitude in DIII, and anterolateral T-wave inversion were predictors of sudden death or malignant ventricular arrhythmias. [19]
The initial chest radiograph should usually be followed by echocardiography. These studies may be the only investigations required, and this approach is by far the most common method for diagnosing dilated cardiomyopathy. Subsequent evaluation of cardiac function may be performed by using cine computed tomography (CT) scanning (in rare cases), nuclear scintigraphy, or magnetic resonance imaging (MRI). [20, 21, 22, 23]
Although ultrafast CT scanners (electron beam) and multidetector-row CT scanners can be used with ECG gating to assess ventricular function, little reason exists to employ this equipment. CT scanners require ionizing radiation and injection of relatively large amounts of iodinated contrast agents. [24]
Gated CT scanning is an accurate means of evaluating cardiac function, especially with the use of ultrafast CT scanning and 50-millisecond image acquisition. Only 1 short breath-hold period is required, and definition of the endocardial margins is excellent, allowing a degree of automation for defining the ventricular volumes. However, coverage of the entire heart may be difficult.
Cardiac MRI is excellent for assessing cardiac function in dilated cardiomyopathy because of the high intrinsic contrast between blood and myocardium, especially on cine MRA. [25] Cine MRA is a repeatable examination, as compared with echocardiography, with less risk of intertest variation resulting from differences in operator or technique. [26] Cine MRA is especially suitable for evaluating the right ventricle, which is difficult to reliably image with other techniques. [27]
MRI and MRA offer excellent noninvasive means of displaying cardiac and coronary anatomy. [28] They provide high spatial and contrast resolution, which can be used to evaluate congenital and acquired abnormalities and assess results of therapy. [29] Pulse sequences (eg, cine MRA sequences) that provide high temporal resolution can be used to identify and quantify functional abnormalities.
Late gadolinium enhancement (LGE) cardiac MRI has shown strong prognostic value in many studies. [30, 31, 32, 33]
A retrospective study by Fu et al of 126 patients with idiopathic dilated cardiomyopathy (IDCM) with reduced left ventricular ejection fraction (LVEF< 40%) showed that the cardiac MRI parameters NT-proBNP (B-type natriuretic peptide), late‑gadolinium enhancement (LGE) mass, and LGE mass/left ventricle mass were significant predictors for major adverse cardiac events (MACEs). [34]
Nuclear images can identify specific causes of left ventricular dysfunction, such as cardiac sarcoidosis and amyloidosis. [35]
Limitations of techniques
Chest radiography is good for assessing the effects of cardiac dysfunction on pulmonary perfusion and the development of pulmonary edema, but radiographs seldom help in identifying the etiology of the dysfunction.
Echocardiography is an excellent method for assessing cardiac function, determining the presence of valve lesions, detecting complications such as thrombus or pericardial effusion, and assessing response to treatment. Echocardiography may be limited in 10-20% of patients by restricted acoustic access and is dependent on operator experience.
Cine CT scanning and CT angiography scanning require radiation and intravenous contrast enhancement; therefore, these techniques are seldom used.
Nuclear scintigraphy is a repeatable technique that often is used when serial examination of cardiac function is required. It is not as valuable as echocardiography, since it provides little anatomic information.
MRI and magnetic resonance angiography (MRA) are the most accurate methods for assessing cardiac anatomy or function. MRI/MRA is used when echocardiography is inadequate, but this study is often not used because of its relatively high cost and limited availability, as well as contraindications if ferromagnetic metallic foreign bodies are present in the patient.
Radiography
Despite the development of cross-sectional imaging techniques, chest radiography remains useful in evaluating cardiac disease. Radiography is inexpensive and poses low risk to the patient. Moreover, it may provide useful information in guiding further investigations. Chest radiograph is a good method to detect a large heart and pulmonary vascular changes in heart failure; however, it often provides little information on etiology, on the degree of cardiac dysfunction, on complicating factors such as valve dysfunction, or on pericardial effusion. For this reason, radiography is usually augmented with a cross-sectional imaging test, usually echocardiography.
If the presenting symptom is dyspnea, radiographic findings may differentiate cardiac etiologies (eg, alcoholic cardiomyopathy [as in the first 3 images below]) from pulmonary ones. Cardiomegaly (cardiac shadow >50% of thorax width on the posteroanterior view), Kerley B lines (prominent lines in the peripheral parts of the lungs, secondary to interstitial edema [see the fourth image below]), pleural effusions, and cephalization of the pulmonary vasculature (as in the fifth image below) are consistent with a cardiac origin of dyspnea. Development of cardiomegaly is easily tracked using chest radiography and is associated with a worse prognosis. Although coronary artery calcification may be a clue to ischemic pathology, it is infrequently identified.
Chest radiograph shows a large heart. Image does not provide any clue to the etiology of the dilated cardiomyopathy; however, the healing rib fractures and right lower lobe pneumonia (aspiration pneumonia) suggest alcoholic cardiomyopathy as the cause.
Magnified right chest radiograph shows an area of right lower lobe aspiration pneumonia in a patient with dilated cardiomyopathy (same patient as in the previous image).
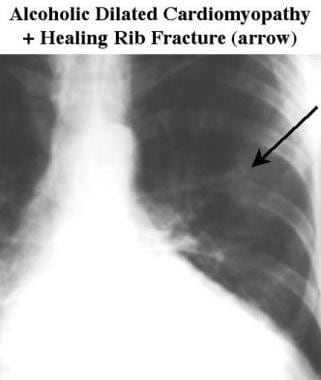 Magnified left chest radiograph in a patient with dilated cardiomyopathy shows rib fractures (arrow) resulting from repeated chest injuries that occurred while the patient was intoxicated (same patient as in the 2 previous images).
Magnified left chest radiograph in a patient with dilated cardiomyopathy shows rib fractures (arrow) resulting from repeated chest injuries that occurred while the patient was intoxicated (same patient as in the 2 previous images).
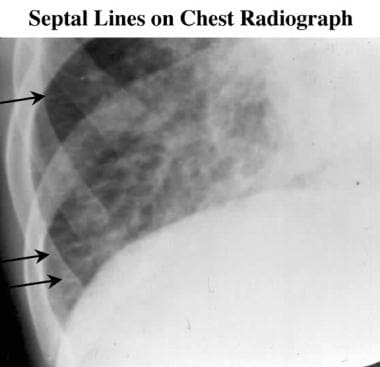 Magnified chest radiograph of the right costophrenic angle in a patient with dilated cardiomyopathy and interstitial pulmonary edema, as demonstrated by prominent septal lines (Kerley B lines). The lines are usually horizontal and seen in the peripheral parts of the lungs secondary to interstitial edema.
Magnified chest radiograph of the right costophrenic angle in a patient with dilated cardiomyopathy and interstitial pulmonary edema, as demonstrated by prominent septal lines (Kerley B lines). The lines are usually horizontal and seen in the peripheral parts of the lungs secondary to interstitial edema.
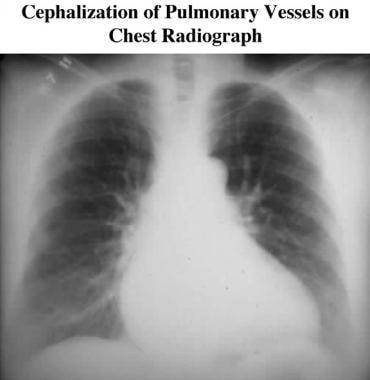 Chest radiograph in a patient with dilated cardiomyopathy shows redistribution of pulmonary blood flow toward the upper lungs (cephalization).
Chest radiograph in a patient with dilated cardiomyopathy shows redistribution of pulmonary blood flow toward the upper lungs (cephalization).
The pattern of cardiac and great vessel enlargement, as well as of alveolar shadowing, may indicate an etiology.
In dilated cardiomyopathy, nonspecific cardiomegaly is usually found, with dilatation of the superior vena cava (see the images below) and the azygos vein. [36]
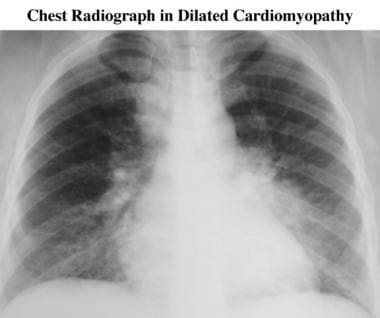 Chest radiograph in a patient presenting with heart failure, which was subsequently found to be the result of dilated cardiomyopathy. Although cardiac size is at the upper limit of normal, left ventricular function is poor, causing severe pulmonary edema with bilateral alveolar edema and marked dilatation of the superior vena cava.
Chest radiograph in a patient presenting with heart failure, which was subsequently found to be the result of dilated cardiomyopathy. Although cardiac size is at the upper limit of normal, left ventricular function is poor, causing severe pulmonary edema with bilateral alveolar edema and marked dilatation of the superior vena cava.
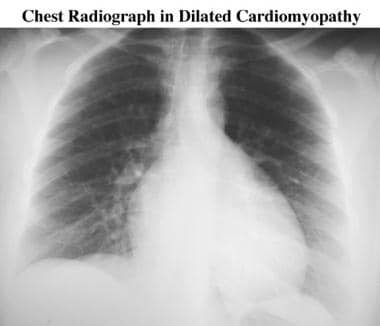 Five-year follow-up chest radiograph in a patient with dilated cardiomyopathy (same patient as in the previous image). The heart is enlarged, but signs of pulmonary congestion (pulmonary edema) and systemic congestion (superior vena cava dilatation) are no longer present, as a result of medical treatment.
Five-year follow-up chest radiograph in a patient with dilated cardiomyopathy (same patient as in the previous image). The heart is enlarged, but signs of pulmonary congestion (pulmonary edema) and systemic congestion (superior vena cava dilatation) are no longer present, as a result of medical treatment.
Magnetic Resonance Imaging
MRI and MRA offer excellent noninvasive means of displaying cardiac and coronary anatomy. [28] They provide high spatial and contrast resolution, which can be used to evaluate congenital and acquired abnormalities and assess results of therapy. [29] Pulse sequences (eg, cine MRA sequences) that provide high temporal resolution can be used to identify and quantify functional abnormalities.
Myocardial edema and inflammation play an important role in dilated cardiomyopathy and have been identified using cardiovascular MRI. T2 mapping has shown that myocardial water content is greater in dilated cardiomyopathy patients and that the myocardial water content increases as the disease progresses. [37]
Cine MRA is well established as the most accurate modality for validating other imaging techniques and for evaluating the effects of medical therapy on ventricular function. [38, 39] MRA can be used to assess cardiac dimensions and systolic function, and phase-contrast techniques can be used to evaluate diastolic dysfunction. [40] Provided ECG gating and breath-holding are effective, reliable and accurate imaging of cardiac function and anatomy is typical.
Contraindications
Contraindications to cardiac MRI are identical to MRI contraindications at any other anatomic site. They include the presence of a pacemaker or other implanted electrical stimulator, ferromagnetic material in the eye, or intracerebral aneurysm clips. Except for the pre-6000 series of Starr-Edwards valves (few of which, if any, exist), no cardiac valve prostheses are a contraindication at the magnetic strengths (< 2 T) currently used for diagnostic MRI. [11] Retained pacemaker wires, surgical clips, and wire sternal sutures are not contraindications to MRI. [41] Coronary and pulmonary artery stents may be imaged safely, although some authors believe it prudent to exclude patients with new (< 6 weeks old) stents from MRI.
Pregnancy is a relative contraindication. If MRI is necessary, the unknown risk to the fetus must be weighed against the benefit to the mother.
Gadolinium-based contrast agents have been linked to the development of nephrogenic systemic fibrosis (NSF) or nephrogenic fibrosing dermopathy (NFD). The disease has occurred in patients with moderate to end-stage renal disease after being given a gadolinium-based contrast agent to enhance MRI or MRA scans.
Technique
MRI of the heart requires an adequate ECG tracing to provide a gating signal for image acquisition at the same part of the cardiac cycle, although some newer sequences (such as true fast imaging with steady-state free precession) are fast enough to be implemented without gating. [42] The quality of the examination probably depends more on this parameter than on any other. The effects of strong magnetic fields on the character of the ECG tracing are unpredictable and may compromise gating.
The hydromagnetic effect of blood flowing in a strong magnetic field may distort the ECG trace and make ECG gating difficult or impossible. Spin-echo MRI has long been used as an accurate method for assessing cardiac dimensions. Phantom studies have shown a high degree of correlation, which is superior to that of other non-MRI techniques.
Spin-echo MRI is the most accurate method for assessing cardiac dimensions, but it is time consuming and provides only static information. [43] Evaluation of cardiac function is improved with cine MRA. For this, either breath-hold or non–breath-hold techniques can be used. [42]
Left ventricular function is optimally evaluated in the following 3 planes (2 of which are demonstrated in the images below):
-
Right anterior oblique equivalent
-
Four-chamber equivalent or oblique axial
-
Multilevel short axis
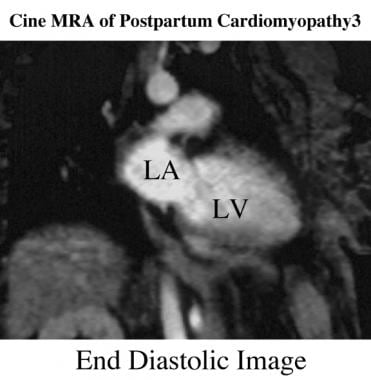 Oblique coronal (right anterior oblique perspective) end-diastolic cine magnetic resonance angiogram in a patient in the recovery phase of postpartum dilated cardiomyopathy. LA is the left atrium; LV, the left ventricle.
Oblique coronal (right anterior oblique perspective) end-diastolic cine magnetic resonance angiogram in a patient in the recovery phase of postpartum dilated cardiomyopathy. LA is the left atrium; LV, the left ventricle.
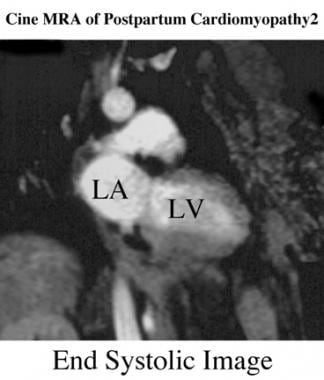 Oblique coronal end-systolic cine magnetic resonance angiogram in a patient recovering from postpartum dilated cardiomyopathy.
Oblique coronal end-systolic cine magnetic resonance angiogram in a patient recovering from postpartum dilated cardiomyopathy.
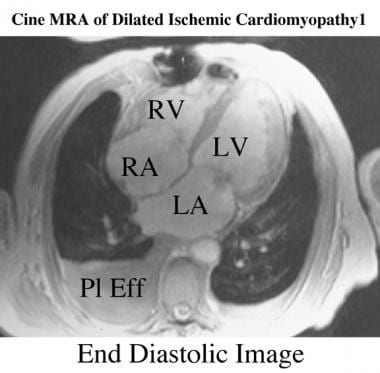 Oblique axial end-diastolic breath-hold cine magnetic resonance angiogram in a patient with dilated ischemic cardiomyopathy. The left ventricle (LV) is moderately dilated as a result of diffuse ischemia. LA is the left atrium; LV, the left ventricle; RV, the right ventricle; and RA, the right atrium.
Oblique axial end-diastolic breath-hold cine magnetic resonance angiogram in a patient with dilated ischemic cardiomyopathy. The left ventricle (LV) is moderately dilated as a result of diffuse ischemia. LA is the left atrium; LV, the left ventricle; RV, the right ventricle; and RA, the right atrium.
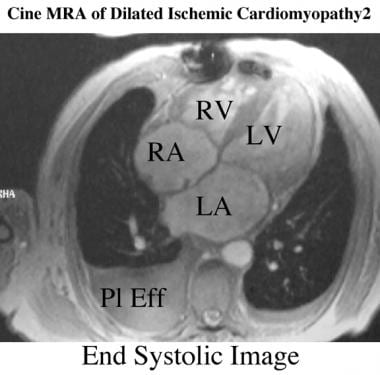 Oblique axial end-systolic breath-hold cine magnetic resonance angiogram in a patient with dilated ischemic cardiomyopathy. Only moderate contraction occurred during systole.
Oblique axial end-systolic breath-hold cine magnetic resonance angiogram in a patient with dilated ischemic cardiomyopathy. Only moderate contraction occurred during systole.




Once the right anterior oblique equivalent and long-axis 4-chamber equivalents are acquired, they can be used to set up short-axis acquisitions. Usually, the authors acquire the images one third and two thirds of the distance between the mitral valve annulus and the apex of the LV, although contiguous sections can be acquired, if necessary, for accurate assessment of left ventricular mass and volume.
As demonstrated in the image below, a variety of mathematical models can be used to derive ventricular dimensions from long-axis views when time is more important than extreme accuracy for measuring volume and mass. [44] For most clinical purposes, the accuracy of long-axis methods compares well with alternative non-MRI techniques. [43] Long-axis views also show signal voids resulting from mitral regurgitation and may be used to assess aortic regurgitation. [45] Short-axis views usually provide better definition of the endocardium, with higher intraluminal signal intensity and a good assessment of septal, inferior, and posterior wall function. Software to automatically calculate ejection fractions and ventricular volumes from data on the images is available. [46]
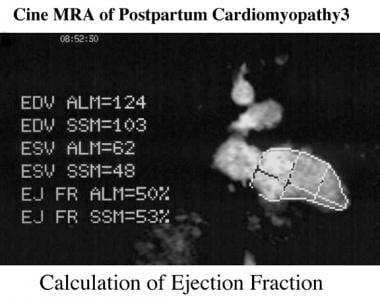 Cine magnetic resonance angiogram in a patient with postpartum cardiomyopathy. Using the area/length method and the Simpson rule, the ejection fraction is calculated as 50-53%. Earlier in the course of the illness, the ejection fraction on echocardiography was as low as 25%. Six months later, left ventricular function was normal (ejection fraction, 67%).
Cine magnetic resonance angiogram in a patient with postpartum cardiomyopathy. Using the area/length method and the Simpson rule, the ejection fraction is calculated as 50-53%. Earlier in the course of the illness, the ejection fraction on echocardiography was as low as 25%. Six months later, left ventricular function was normal (ejection fraction, 67%).
Breath-hold tagging sequences have been developed (see the images below). The use of linear or cross tags enhances appreciation of subtle regional wall motion abnormalities. [47, 48]
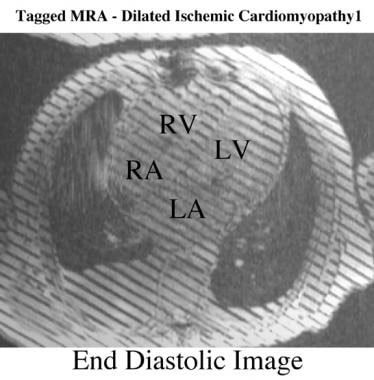 Oblique axial end-diastolic breath-hold linear-tagged cine magnetic resonance angiogram in a patient with dilated ischemic cardiomyopathy. Linear tags have been applied across the myocardium of a dilated left ventricle at end diastole.
Oblique axial end-diastolic breath-hold linear-tagged cine magnetic resonance angiogram in a patient with dilated ischemic cardiomyopathy. Linear tags have been applied across the myocardium of a dilated left ventricle at end diastole.
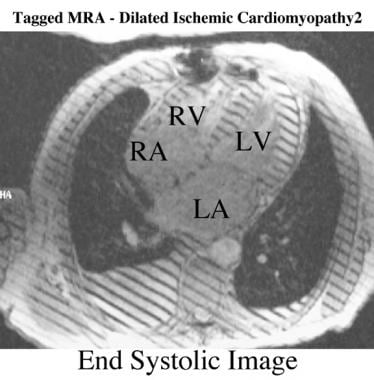 Oblique axial end-systolic breath-hold linear-tagged cine magnetic resonance angiography in a patient with dilated ischemic cardiomyopathy. The linear tags across the myocardium have decayed on this image, acquired at end systole. All tags have moved to a similar extent, indicating diffusely impaired contraction.
Oblique axial end-systolic breath-hold linear-tagged cine magnetic resonance angiography in a patient with dilated ischemic cardiomyopathy. The linear tags across the myocardium have decayed on this image, acquired at end systole. All tags have moved to a similar extent, indicating diffusely impaired contraction.
Cardiac MRI is excellent for assessing cardiac function in dilated cardiomyopathy because of the high intrinsic contrast between blood and myocardium, especially on cine MRA. [25] Cine MRA is a repeatable examination, as compared with echocardiography, with less risk of intertest variation resulting from differences in operator or technique. [26] Cine MRA is especially suitable for evaluating the right ventricle, which is difficult to reliably image with other techniques. [27]
Multilevel cine MRA is the most accurate method for assessing cardiac function and dimensions. [49] In addition to providing a means of assessing cardiac function, signal abnormalities may indicate a metabolic or inflammatory etiology for dilated cardiomyopathy. [50, 51]
In some patients, endocardial surfaces may be defined poorly or intraluminal signal may be lost, as in areas with a slow flow related to ventricular dyskinesia. This may occur especially on long-axis views, which increase the likelihood of in-plane signal saturation. This problem can be overcome by using intravenous contrast media (eg, gadolinium diethylenetriamine pentaacetic acid), which increasees signal intensity for up to 20 minutes. [52] However, this technique reduces the extent of any flow void resulting from valve regurgitation.
Findings
Causes of abnormal myocardial signal intensity on T1-weighted images include the following [53] :
-
Hypertrophic cardiomyopathy (variable signal)
-
Hemochromatosis/hemosiderosis (low signal intensity, also shortened T2 relaxation)
-
Arrhythmogenic right ventricular dysplasia (high signal intensity in right ventricular wall)
-
Transplant rejection
-
Myocarditis (after gadolinium enhancement)
Causes of high myocardial signal on T2-weighted images include the following:
-
Metastases
-
Myocarditis (variable)
-
Abscesses
Late gadolinium enhancement (LGE) cardiac MRI has shown strong prognostic value in many studies. [30, 31, 32, 33]
A retrospective study by Fu et al of 126 patients with idiopathic dilated cardiomyopathy (IDCM) with reduced left ventricular ejection fraction (LVEF< 40%) showed that the cardiac MRI parameters NT-proBNP (B-type natriuretic peptide), late‑gadolinium enhancement (LGE) mass, and LGE mass/left ventricle mass were significant predictors for major adverse cardiac events (MACEs). [34]
In a study by Behera et al of 112 patients with nonischemic dilated cardiomyopathy who underwent CMR, late gadolinium enhancement and its extent greater than14% predicted MACEs irrespective of LVEF and LGE location, pattern, or distribution. [30]
Ultrasonography
Echocardiography is the next and, usually, most useful investigation after chest radiography. Echocardiograms (seen in the images below) are useful for excluding other causes of a large heart shadow, such as pericardial effusion or multiple valve disease. In dilated cardiomyopathy, all of the heart chambers are typically dilated, and both ventricles are diffusely hypokinetic.
In a study by Merlo et al of 414 patients with dilated cardiomyopathy who underwent ECG testing, 55 patients experienced death or heart transplant and 57 patients experienced sudden death or malignant ventricular arrhythmias during a 125-month follow-up period. Left ventricular hypertrophy, heart rate, and anterolateral T-wave inversion predicted death or heart transplant. S wave amplitude in V2, R wave amplitude in DIII, and anterolateral T-wave inversion were predictors of sudden death or malignant ventricular arrhythmias. [19]
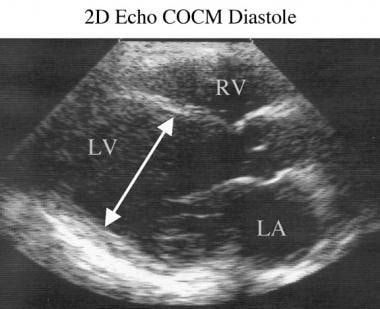 Two-dimensional end-diastolic echocardiogram in a patient with dilated cardiomyopathy (congestive cardiomyopathy at diastole) shows the transverse diameter (arrow). LV is the left ventricle; RV, the right ventricle; and LA, the left atrium.
Two-dimensional end-diastolic echocardiogram in a patient with dilated cardiomyopathy (congestive cardiomyopathy at diastole) shows the transverse diameter (arrow). LV is the left ventricle; RV, the right ventricle; and LA, the left atrium.
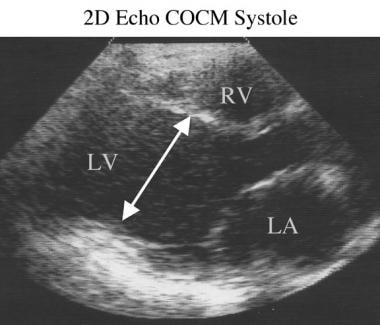 Two-dimensional end-diastolic echocardiogram in a patient with dilated cardiomyopathy (congestive cardiomyopathy at systole). The transverse diameter (arrow) has hardly changed in length from the end-diastolic image. LV is the left ventricle; RV, the right ventricle; and LA, the left atrium.
Two-dimensional end-diastolic echocardiogram in a patient with dilated cardiomyopathy (congestive cardiomyopathy at systole). The transverse diameter (arrow) has hardly changed in length from the end-diastolic image. LV is the left ventricle; RV, the right ventricle; and LA, the left atrium.
A feature that may help distinguish idiopathic dilated cardiomyopathy from ischemic cardiomyopathy is the presence of global, rather than regional, dysfunction. However, in some patients with dilated cardiomyopathy, regional dysfunction may be seen as a result of the preservation of systolic function at the base of the LV or the presence of left bundle branch block, which causes paradoxical septal motion.
Right ventricular function often is relatively preserved in ischemic cardiomyopathy. Ventricular walls may be normal, increased, or decreased in thickness. The left atrium usually is dilated early on, while right ventricular and right atrial enlargement occur later.
The most precise left ventricular cavity and wall-thickness measurements at end diastole, end systole, and ejection fraction are obtained by using M-mode echocardiography (shown in the image below), which has the best temporal resolution of any imaging technique. Measurements obtained in a standardized way (at the tips of the mitral valve leaflets) are important to allow for useful comparison with published reference values.
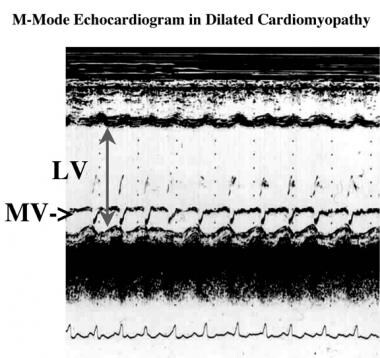 M-mode echocardiogram acquired at the level of the tips of the mitral valve leaflets shows dilated and poorly contracting left ventricle in a patient with dilated cardiomyopathy. Arrow shows the transverse diameter of the left ventricle.
M-mode echocardiogram acquired at the level of the tips of the mitral valve leaflets shows dilated and poorly contracting left ventricle in a patient with dilated cardiomyopathy. Arrow shows the transverse diameter of the left ventricle.
Two-dimensional echocardiography, with its superior spatial coverage, is used to guide the positioning of the M-mode sample for direct measurements of ventricular wall thickness, left ventricular volumes, and ejection fraction. An advantage of 2-dimensional echocardiography (compared with M-mode imaging) is that the myocardial mass, chamber volumes, and ejection fraction of an abnormally shaped ventricle can be measured. However, because of the subjective nature of 2-dimensional echo examination, its risk of error is higher than that of other cross-sectional imaging techniques.
In most patients, images of the mitral and tricuspid valves appear normal but with an abnormally central position with nearly equal excursion of the anterior and posterior leaflets. Significant atrioventricular regurgitation may occur because of incomplete closure of the mitral and tricuspid leaflets as a result of annular dilatation. The motion of the mitral valve may reflect the high diastolic pressure, with early opening of the valve leaflets appreciated on M-mode echo (so-called C-hump). Pericardial effusions are common, but they tend to be relatively small and do not cause significant hemodynamic problems. Mural thrombi may be seen in dilated chambers, especially those with severe hypokinesia. The above characteristics are demonstrated in the images below.
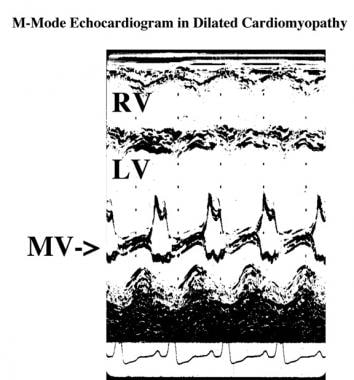 M-mode echocardiogram in a patient with dilated cardiomyopathy shows the mitral valve (MV) centrally placed in the left ventricle (LV), with near equal movement of the anterior and posterior leaflets. The right ventricle (RV) and LV are dilated and poorly contracting as a result of alcoholic cardiomyopathy.
M-mode echocardiogram in a patient with dilated cardiomyopathy shows the mitral valve (MV) centrally placed in the left ventricle (LV), with near equal movement of the anterior and posterior leaflets. The right ventricle (RV) and LV are dilated and poorly contracting as a result of alcoholic cardiomyopathy.
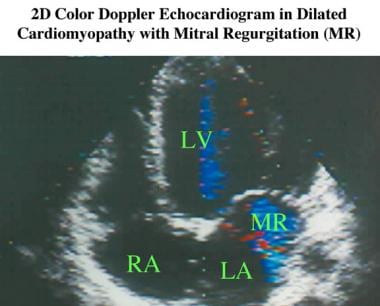 Apical 2-dimensional echocardiogram with color Doppler display (systolic image) in a patient with dilated cardiomyopathy shows a jet of mitral regurgitation (MR) into a large left atrium (LA) (Doppler encoded blue). Note the dilatation of the left ventricle (LV) compared with the right ventricle.
Apical 2-dimensional echocardiogram with color Doppler display (systolic image) in a patient with dilated cardiomyopathy shows a jet of mitral regurgitation (MR) into a large left atrium (LA) (Doppler encoded blue). Note the dilatation of the left ventricle (LV) compared with the right ventricle.
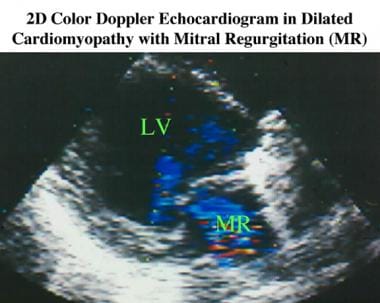 Parasternal long-axis 2-dimensional systolic echocardiogram with color Doppler display. Compare this and the previous image, noting the eccentric nature of the jet of mitral regurgitation. The left ventricle still is clearly dilated, but the left atrium appears smaller than it is on the previous image because of the obliquity of the imaging plane.
Parasternal long-axis 2-dimensional systolic echocardiogram with color Doppler display. Compare this and the previous image, noting the eccentric nature of the jet of mitral regurgitation. The left ventricle still is clearly dilated, but the left atrium appears smaller than it is on the previous image because of the obliquity of the imaging plane.
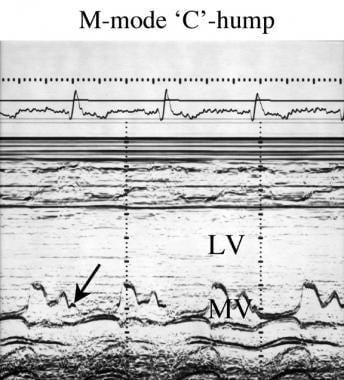 M-mode C-hump (arrow) echocardiogram in a patient with dilated cardiomyopathy. The tips of the mitral valve leaflets are displaced toward the center of the left ventricular cavity.
M-mode C-hump (arrow) echocardiogram in a patient with dilated cardiomyopathy. The tips of the mitral valve leaflets are displaced toward the center of the left ventricular cavity.
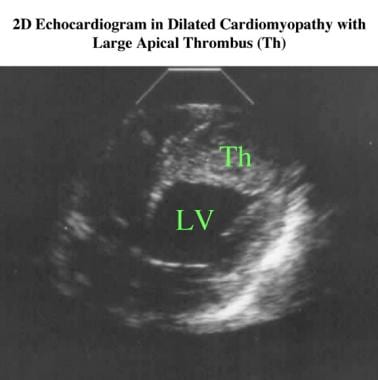 Two-dimensional echocardiogram in a patient with ischemic cardiomyopathy shows extensive thrombus (Th) in the apex of the left ventricle (LV).
Two-dimensional echocardiogram in a patient with ischemic cardiomyopathy shows extensive thrombus (Th) in the apex of the left ventricle (LV).
Nuclear Imaging
The most important contribution of nuclear cardiology is the ability to assess myocardial perfusion and ventricular function. Nuclear ventriculography is a reliable and reproducible method for assessing left ventricular function, which is an especially important consideration when one performs sequential studies to assess the effects of therapy. [54, 55]
Radionuclide ventriculography (multiple-gated acquisition or first-pass scanning; shown in the images below) is used to estimate ventricular size and ejection fraction and to assess wall motion abnormalities. Diastolic dysfunction and the response to exercise also can be reliably evaluated. [55, 56] In idiopathic dilated cardiomyopathy, the global ejection fraction is decreased and wall motion is uniformly poor, with the exception of possible sparing of the septal and anterior basal segments.
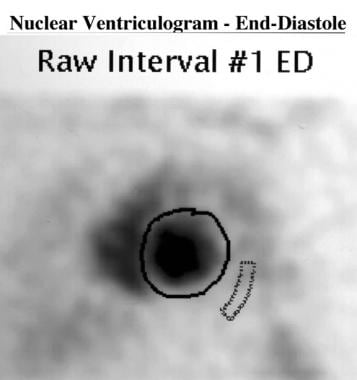 End-diastolic cardiac nuclear ventriculogram (obtained with technetium-99m–tagged red blood cells) in a patient with dilated cardiomyopathy. The left ventricle is outlined, and a sample of activity is demonstrated in the adjacent background. The left ventricle appears enlarged.
End-diastolic cardiac nuclear ventriculogram (obtained with technetium-99m–tagged red blood cells) in a patient with dilated cardiomyopathy. The left ventricle is outlined, and a sample of activity is demonstrated in the adjacent background. The left ventricle appears enlarged.
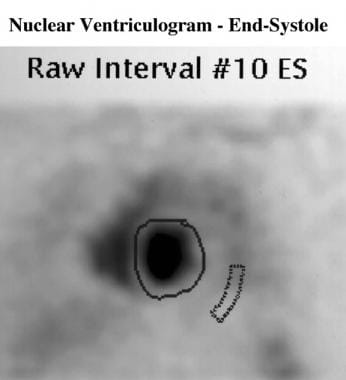 Nuclear image of the heart in end systole, with the left ventricle outlined and the background unchanged, in a patient with dilated cardiomyopathy. Note that the left ventricle does not empty well.
Nuclear image of the heart in end systole, with the left ventricle outlined and the background unchanged, in a patient with dilated cardiomyopathy. Note that the left ventricle does not empty well.
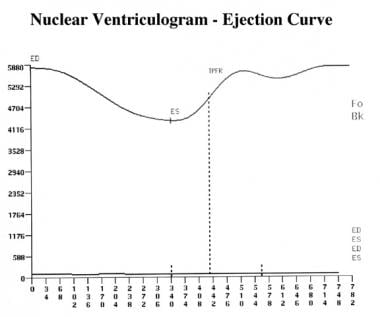 Left ventricular time-activity curve, with end diastole (ED) and end systole (ES) demarcated, in a patient with dilated cardiomyopathy. The curve is shallow, indicating poor ventricular emptying. TPFR is the time-to–peak filling rate.
Left ventricular time-activity curve, with end diastole (ED) and end systole (ES) demarcated, in a patient with dilated cardiomyopathy. The curve is shallow, indicating poor ventricular emptying. TPFR is the time-to–peak filling rate.
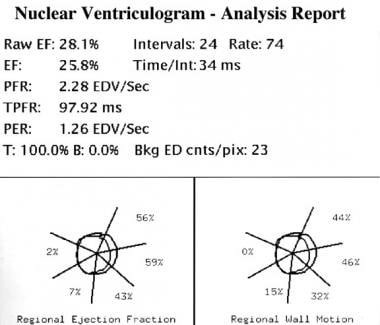 Measured global left ventricular ejection fraction is 25.8% in a patient with dilated cardiomyopathy. This value is severely depressed (reference range, 50-75%). Measurements of regional wall motion and ejection fraction are seen in the small boxes.
Measured global left ventricular ejection fraction is 25.8% in a patient with dilated cardiomyopathy. This value is severely depressed (reference range, 50-75%). Measurements of regional wall motion and ejection fraction are seen in the small boxes.
Radionuclide perfusion imaging can help in differentiating ischemic causes and other etiologies. A perfusion defect of greater than 40% strongly suggests ischemic etiology. Unfortunately, large and fixed (especially apical) perfusion defects have been reported in dilated cardiomyopathy. [57]
Radionuclide ventriculography is frequently used to follow the cardiotoxic effects of drugs (eg, doxorubicin) that cause cardiomyopathy. Dilated cardiomyopathy caused by doxorubicin usually produces severe, irreversible left ventricular dysfunction symptoms of congestive heart failure; therefore, it is essential to detect ventricular dysfunction early, well before any irreversible changes occur. Because radionuclide ventriculography is a reproducible technique, it is used widely for this purpose. [58] The technique can also be used to assess the response to therapy in patients with any form of idiopathic cardiomyopathy.
Gated single-photon emission CT (SPECT) has been used to successfully identify etiologies of dilated cardiomyopathy, because of its ability to depict myocardial perfusion and function. Myocardial perfusion and function imaging has been used to accurately classify cardiomyopathies as ischemic or nonischemic, depending on the gated SPECT and perfusion images. [59] Ischemic cardiomyopathies tend to have reversible or fixed perfusion defects along with regional wall motion abnormalities on gated SPECT, while nonischemic cardiomyopathies demonstrate mild perfusion defects with diffuse wall motion abnormalities.
Degree of confidence
The degree of confidence is high. Nuclear ventriculography is a relatively accurate and repeatable method for assessing left ventricular function. It has been used for longitudinal studies to assess the response to medical treatment and to detect early changes resulting from drug toxicity, which may lead to dilated cardiomyopathy in patients undergoing chemotherapy with anthracycline cytotoxic agents.
Angiography
Determining ischemic heart disease as a cause of cardiomyopathy is important because it may help in identifying treatable pathology. Coronary angiography remains the best technique for assessing epicardial coronary artery disease and for determining whether revascularization can potentially reverse the cardiomyopathy. Multiple studies of patients with symptomatic heart failure, coronary artery disease suitable for revascularization, and poor systolic function (with or without angina) have demonstrated a survival and ventricular function benefit in surgical treatment in comparison with medical therapy.
The need for coronary angiography depends on the following factors:
-
A history of angina, prior myocardial infarction, or antecedent viral syndrome or family history of cardiomyopathy
-
A high probability of coronary artery disease in the patient, as based on age, sex, and risk factors
-
Generalized ischemic heart disease, as indicated on noninvasive tests, such as echocardiography or nuclear medicine studies at rest or after stress
Coronary angiography is performed in multiple projections because it is a projectional technique, and atherosclerotic lesions typically are eccentric. Many groups have correlated the degree of stenosis with ultimate clinical or pathologic outcome. The severity of obstructive disease is assessed in each coronary artery segment by comparing the arterial diameter at a point of maximum lumen reduction with that of a proximal or distal normal-appearing artery.
Nonatherosclerotic coronary disease occasionally causes ischemic heart disease. Examples include causes of arteritis (eg, Takayasu disease, giant cell arteritis, polyarteritis nodosa), infections (eg, syphilitic stenoses of the coronary ostia, aortic root abscess), congenital coronary anomalies, and Kawasaki disease. [60]
During cardiac catheterization, a left ventriculogram usually is obtained to assess the LV, which demonstrates diffuse enlargement and reduced contractility. Abnormalities of segmental wall motion are common, and mural thrombi may be found in the apex.
Cine angiography was once regarded as the reference standard for assessing LV function. Currently, this is not the case; as a result of its projectional nature and the need to inject contrast agent, cine angiography may be inaccurate. In particular, it can fail to demonstrate regional wall motion abnormalities. Three-dimensional echo imaging and cine MRA are more accurate in assessing global and regional ventricular function. [61] However, a few contraindications to cardiac catheterization have been identified.
-
Chest radiograph shows a large heart. Image does not provide any clue to the etiology of the dilated cardiomyopathy; however, the healing rib fractures and right lower lobe pneumonia (aspiration pneumonia) suggest alcoholic cardiomyopathy as the cause.
-
Magnified right chest radiograph shows an area of right lower lobe aspiration pneumonia in a patient with dilated cardiomyopathy (same patient as in the previous image).
-
Magnified left chest radiograph in a patient with dilated cardiomyopathy shows rib fractures (arrow) resulting from repeated chest injuries that occurred while the patient was intoxicated (same patient as in the 2 previous images).
-
Magnified chest radiograph of the right costophrenic angle in a patient with dilated cardiomyopathy and interstitial pulmonary edema, as demonstrated by prominent septal lines (Kerley B lines). The lines are usually horizontal and seen in the peripheral parts of the lungs secondary to interstitial edema.
-
Chest radiograph in a patient with dilated cardiomyopathy shows redistribution of pulmonary blood flow toward the upper lungs (cephalization).
-
Chest radiograph in a patient presenting with heart failure, which was subsequently found to be the result of dilated cardiomyopathy. Although cardiac size is at the upper limit of normal, left ventricular function is poor, causing severe pulmonary edema with bilateral alveolar edema and marked dilatation of the superior vena cava.
-
Five-year follow-up chest radiograph in a patient with dilated cardiomyopathy (same patient as in the previous image). The heart is enlarged, but signs of pulmonary congestion (pulmonary edema) and systemic congestion (superior vena cava dilatation) are no longer present, as a result of medical treatment.
-
Spiral computed tomography (CT) scan obtained with intravenous contrast enhancement at the level of the center of the mitral valve (between arrows) and tricuspid valve in a patient with dilated cardiomyopathy. Left ventricle (LV) is dilated compared with the right ventricle (RV).
-
Oblique coronal (right anterior oblique perspective) end-diastolic cine magnetic resonance angiogram in a patient in the recovery phase of postpartum dilated cardiomyopathy. LA is the left atrium; LV, the left ventricle.
-
Oblique coronal end-systolic cine magnetic resonance angiogram in a patient recovering from postpartum dilated cardiomyopathy.
-
Cine magnetic resonance angiogram in a patient with postpartum cardiomyopathy. Using the area/length method and the Simpson rule, the ejection fraction is calculated as 50-53%. Earlier in the course of the illness, the ejection fraction on echocardiography was as low as 25%. Six months later, left ventricular function was normal (ejection fraction, 67%).
-
Oblique axial end-diastolic breath-hold cine magnetic resonance angiogram in a patient with dilated ischemic cardiomyopathy. The left ventricle (LV) is moderately dilated as a result of diffuse ischemia. LA is the left atrium; LV, the left ventricle; RV, the right ventricle; and RA, the right atrium.
-
Oblique axial end-systolic breath-hold cine magnetic resonance angiogram in a patient with dilated ischemic cardiomyopathy. Only moderate contraction occurred during systole.
-
Oblique axial end-diastolic breath-hold linear-tagged cine magnetic resonance angiogram in a patient with dilated ischemic cardiomyopathy. Linear tags have been applied across the myocardium of a dilated left ventricle at end diastole.
-
Oblique axial end-systolic breath-hold linear-tagged cine magnetic resonance angiography in a patient with dilated ischemic cardiomyopathy. The linear tags across the myocardium have decayed on this image, acquired at end systole. All tags have moved to a similar extent, indicating diffusely impaired contraction.
-
Oblique axial turbo spin-echo image in a patient with sarcoid shows high signal intensity (circle) in the apical part of the interventricular septum.
-
Two-dimensional end-diastolic echocardiogram in a patient with dilated cardiomyopathy (congestive cardiomyopathy at diastole) shows the transverse diameter (arrow). LV is the left ventricle; RV, the right ventricle; and LA, the left atrium.
-
Two-dimensional end-diastolic echocardiogram in a patient with dilated cardiomyopathy (congestive cardiomyopathy at systole). The transverse diameter (arrow) has hardly changed in length from the end-diastolic image. LV is the left ventricle; RV, the right ventricle; and LA, the left atrium.
-
M-mode echocardiogram acquired at the level of the tips of the mitral valve leaflets shows dilated and poorly contracting left ventricle in a patient with dilated cardiomyopathy. Arrow shows the transverse diameter of the left ventricle.
-
M-mode echocardiogram in a patient with dilated cardiomyopathy shows the mitral valve (MV) centrally placed in the left ventricle (LV), with near equal movement of the anterior and posterior leaflets. The right ventricle (RV) and LV are dilated and poorly contracting as a result of alcoholic cardiomyopathy.
-
Apical 2-dimensional echocardiogram with color Doppler display (systolic image) in a patient with dilated cardiomyopathy shows a jet of mitral regurgitation (MR) into a large left atrium (LA) (Doppler encoded blue). Note the dilatation of the left ventricle (LV) compared with the right ventricle.
-
Parasternal long-axis 2-dimensional systolic echocardiogram with color Doppler display. Compare this and the previous image, noting the eccentric nature of the jet of mitral regurgitation. The left ventricle still is clearly dilated, but the left atrium appears smaller than it is on the previous image because of the obliquity of the imaging plane.
-
M-mode C-hump (arrow) echocardiogram in a patient with dilated cardiomyopathy. The tips of the mitral valve leaflets are displaced toward the center of the left ventricular cavity.
-
Two-dimensional echocardiogram in a patient with ischemic cardiomyopathy shows extensive thrombus (Th) in the apex of the left ventricle (LV).
-
Continuous-wave Doppler image shows tricuspid regurgitation with a peak velocity of 2 m/s. With the modified Bernoulli formula (peak valve gradient – 4V2, where V = velocity in m/s), this indicates a peak pressure difference between the right ventricle and the right atrium of 16 mm Hg and a reasonable estimate of right ventricular pressure of approximately 26-30 mm Hg (if central venous pressure is 10-14 mm Hg, which can be estimated on physical examination).
-
End-diastolic cardiac nuclear ventriculogram (obtained with technetium-99m–tagged red blood cells) in a patient with dilated cardiomyopathy. The left ventricle is outlined, and a sample of activity is demonstrated in the adjacent background. The left ventricle appears enlarged.
-
Nuclear image of the heart in end systole, with the left ventricle outlined and the background unchanged, in a patient with dilated cardiomyopathy. Note that the left ventricle does not empty well.
-
Left ventricular time-activity curve, with end diastole (ED) and end systole (ES) demarcated, in a patient with dilated cardiomyopathy. The curve is shallow, indicating poor ventricular emptying. TPFR is the time-to–peak filling rate.
-
Measured global left ventricular ejection fraction is 25.8% in a patient with dilated cardiomyopathy. This value is severely depressed (reference range, 50-75%). Measurements of regional wall motion and ejection fraction are seen in the small boxes.





