Practice Essentials
Bronchogenic cysts are congenital and are commonly located in the middle mediastinal compartment as fluid-filled cysts. [1] They are part of a spectrum of congenital abnormalities of the lung, including pulmonary sequestration, congenital cystic adenomatoid malformation, and congenital lobar hyperinflation (emphysema). [2, 3, 4] Bronchogenic cysts are found in mediastinal, hilar and intrapulmonary locations. Intracranial bronchogenic cysts have been rarely observed. [5, 6, 7]
They are derived from abnormal germination of the embryonic foregut during the first 16 weeks of gestation and differentiate into fluid‐filled pouches and constitute 10-15% of all primary mediastinal masses. They rarely occur in the skin and subcutaneous tissues, neck, pericardium, diaphragm, mesentery of the bowel, and intramedullary part of the spine. There have also been reports of extension from the mediastinum through the diaphragm into the abdomen. [1, 8]
Bronchogenic cysts are usually an incidental finding, and differentiating them from other pathologic conditions is important. [1, 8, 9] On conventional radiographs, the appearances of mediastinal or lung masses are nonspecific and should be evaluated further using computed tomography (CT) scanning or magnetic resonance imaging (MRI). [9, 10]
Bronchogenic cysts can cause life-threatening complications associated with infection, rupture, hemorrhage, and compression of surrounding structures. [7, 11]
Chest radiography is usually adequate for detecting larger mediastinal or lung masses; however, it is limited in its ability to differentiate solid masses from fluid. On chest radiographs, pulmonary bronchogenic cysts are sharply defined, solitary, round or oval opacities, usually located in the lower lobe. They can present as a homogeneous water density, as an air-filled cyst, or with an air-fluid level. Abnormalities in the surrounding lung parenchyma, atelectasis, or consolidation may occur, making the diagnosis more difficult. Mediastinal bronchogenic cysts are homogeneous, smooth, solitary, round or ovoid masses usually in the middle mediastinum [10]
CT scan findings are characteristic when the lesion demonstrates water density. If the lesion demonstrates soft-tissue density, differentiating the cyst from lymph nodes or other solid lesions is difficult. CT is the imaging modality of choice. The density of bronchogenic cysts on CT is variable: from typical water density to high density related to blood, increased calcium content, anthracotic pigment, or increased protein content of the fluid. [12, 13, 10, 14]
MRI is better than CT at delineating anatomic relations and definition of the cyst. On T1-weighted images, the intrinsic signal intensity varies from low to high, depending on the cyst contents. T2-weighted images show high signal intensity. Frequently there is no enhancement with contrast. MRI findings are usually diagnostic for mediastinal cysts. Intrapulmonary cysts are difficult to diagnose and must usually be aspirated to confirm the diagnosis. [12, 13, 15, 16, 17, 18, 10]
(See the images below.)
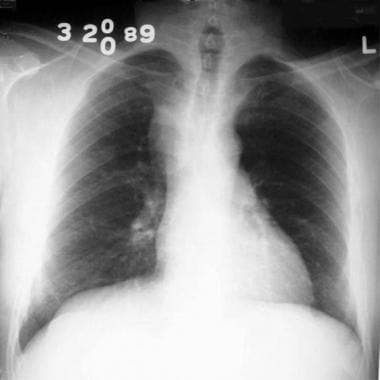
 Bronchogenic cyst. Anteroposterior view on conventional radiograph demonstrates a mass in the aorto-pulmonary window.
Bronchogenic cyst. Anteroposterior view on conventional radiograph demonstrates a mass in the aorto-pulmonary window.

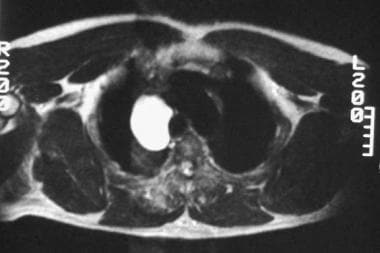 Bronchogenic cyst. Axial T2-weighted MRI demonstrates a high signal mass in the right paratracheal region.
Bronchogenic cyst. Axial T2-weighted MRI demonstrates a high signal mass in the right paratracheal region.
Radiography
Mediastinal cysts are visualized as a mediastinal mass on conventional radiographs. [12] Intrapulmonary cysts usually present as a solitary pulmonary nodule unless the cyst contains air. On conventional radiographs, findings are nonspecific. On chest radiographs, pulmonary bronchogenic cysts are sharply defined, solitary, round or oval opacities, usually located in the lower lobe. They can present as a homogeneous water density, as an air-filled cyst, or with an air-fluid level. Abnormalities in the surrounding lung parenchyma, atelectasis, or consolidation may occur, making the diagnosis more difficult. Mediastinal bronchogenic cysts are homogeneous, smooth, solitary, round or ovoid masses usually in the middle mediastinum. [10]
Mediastinal masses should be evaluated further using CT scanning or MRI to confirm the presence of fluid. Difficulty is encountered in determining whether the visualized mass is benign (eg, a bronchogenic cyst) or malignant.
(Radiographs of bronchogenic cysts are shown below.)
Bronchogenic cyst. Anteroposterior view on conventional radiograph demonstrates a mass in the aorto-pulmonary window.
 Bronchogenic cyst. Lateral view on conventional radiograph demonstrates filling of the retrosternal clear space correlating to the abnormality observed on the frontal view.
Bronchogenic cyst. Lateral view on conventional radiograph demonstrates filling of the retrosternal clear space correlating to the abnormality observed on the frontal view.
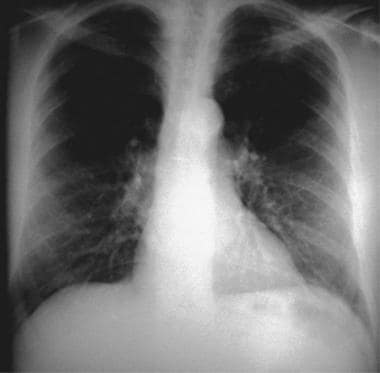
 Bronchogenic cyst. Conventional radiograph demonstrates a right paratracheal mass.
Bronchogenic cyst. Conventional radiograph demonstrates a right paratracheal mass.

 Bronchogenic cyst. Conventional radiograph demonstrates a thin-walled cyst in the left lower lobe with an air-fluid level.
Bronchogenic cyst. Conventional radiograph demonstrates a thin-walled cyst in the left lower lobe with an air-fluid level.
Computed Tomography
CT is the imaging modality of choice. The density of bronchogenic cysts on CT is variable: from typical water density to high density related to blood, increased calcium content, anthracotic pigment, or increased protein content of the fluid. [12, 13, 10]
Bronchogenic cysts are sharply marginated masses demonstrating water or soft-tissue density. [12, 19] Differences in attenuation result from the amount of proteinaceous fluid within the cysts. Cysts do not enhance after administration of IV contrast. An article from the Armed Forces Institute of Pathology documented the appearance of 62 cysts: 40% were water density, 40% were soft-tissue density, 5% contained milk of calcium, 10% were indeterminate from streak artifact, and the remainder were intrapulmonary, either completely air filled or containing an air-fluid level. [20]
In the proper clinical setting, a CT scan finding of a sharply marginated, nonenhancing, water-density mass is diagnostic of a bronchogenic cyst. Nonenhancing masses demonstrating soft-tissue density need further evaluation using MRI. Location is also important. Intrapulmonary cysts are usually difficult to diagnose and usually require aspiration for diagnosis.
Most bronchogenic cysts are relatively characteristic in appearance on CT scan, but in atypical cases with hemorrhage or infection, findings may be confused with those of necrotic adenopathy, cystic lung disease, or lung abscess. [11]
In addition to intrapulmonary and mediastinal locations, bronchogenic cysts have been reported to be located in infradiaphragmatic areas, cutaneous areas, intrapericardial areas, and intramural areas of the esophagus.
(CT scans of bronchogenic cysts are shown below.)
Magnetic Resonance Imaging
MRI is better than CT at delineating anatomic relations and definition of the cyst. On T1-weighted images, the intrinsic signal intensity varies from low to high, depending on the cyst contents. T2-weighted images show high signal intensity. Frequently there is no enhancement with contrast. MRI findings are usually diagnostic for mediastinal cysts. Intrapulmonary cysts are difficult to diagnose and must usually be aspirated to confirm the diagnosis. [12, 13, 15, 16, 17, 18, 10]
Bronchogenic cysts are usually bright on T2-weighted images and dark on T1-weighted images (see the Image below). [19] Cysts do not enhance after administration of IV gadolinium. [18]
On T2-weighted images, the brighter the cyst, the more confident the diagnosis of bronchogenic cyst. Lack of enhancement is also characteristic. Location is important in differentiating bronchogenic cysts from other cysts, such as pericardial cysts.
As with CT scans of typical bronchogenic cysts, MRI findings are very specific and few false-positive or false-negative findings occur. For atypical cysts, the main confusion is with necrotic tumors or infections.
Bronchogenic cyst. Axial T2-weighted MRI demonstrates a high signal mass in the right paratracheal region.
-
Bronchogenic cyst. Anteroposterior view on conventional radiograph demonstrates a mass in the aorto-pulmonary window.
-
Bronchogenic cyst. Lateral view on conventional radiograph demonstrates filling of the retrosternal clear space correlating to the abnormality observed on the frontal view.
-
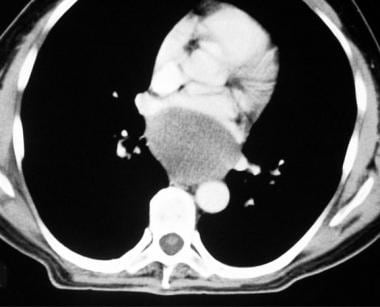
Bronchogenic cyst. Anteroposterior CT demonstrates a mass with fluid density.
-
Bronchogenic cyst. Conventional radiograph demonstrates a right paratracheal mass.
-
Bronchogenic cyst. Axial T2-weighted MRI demonstrates a high signal mass in the right paratracheal region.
-
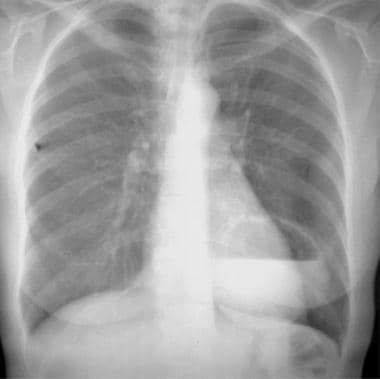
Bronchogenic cyst. Conventional radiograph demonstrates a subcarinal mass.
-
Bronchogenic cyst. Conventional radiograph demonstrates a subcarinal mass.
-
Bronchogenic cyst. CT demonstrates a subcarinal mass with fluid density.
-
Bronchogenic cyst. Conventional radiograph demonstrates a thin-walled cyst in the left lower lobe with an air-fluid level.
-
Bronchogenic cyst. Conventional radiograph demonstrates a thin-walled cyst in the left lower lobe with an air-fluid level.
-
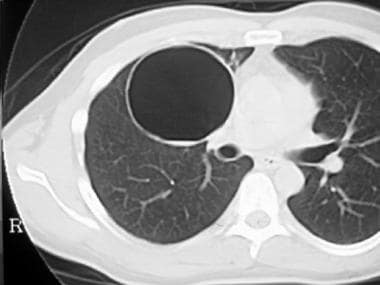
Bronchogenic cyst. CT demonstrates a thin-walled cyst in the right upper lobe.



