Practice Essentials
Fibroadenomas are benign tumors composed of stromal and epithelial elements (see the images below) that are commonly seen in young women. Multiple or complex fibroadenomas may indicate a slightly increased risk for breast cancer. The relative risk of breast cancer in patients with such fibroadenomas is approximately twice that of patients of similar age without fibroadenomas. [1]
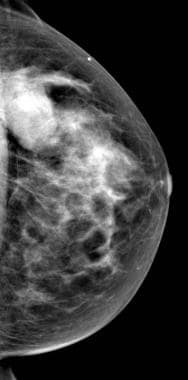 Partially circumscribed oval mass with some obscured margins in upper outer quadrant in craniocaudal view of mammogram in 32-year-old woman with palpable lump in same location.
Partially circumscribed oval mass with some obscured margins in upper outer quadrant in craniocaudal view of mammogram in 32-year-old woman with palpable lump in same location.
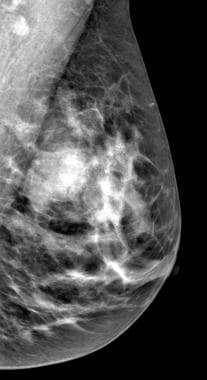 Mediolateral-oblique mammogram view also demonstrates same circumscribed oval mass in same patient. While such a mass is likely a fibroadenoma, mammogram findings are not specific and ultrasound is needed for further evaluation.
Mediolateral-oblique mammogram view also demonstrates same circumscribed oval mass in same patient. While such a mass is likely a fibroadenoma, mammogram findings are not specific and ultrasound is needed for further evaluation.
Preferred examination
A patient's age determines the preferred imaging method. In general, ultrasonography (US) is preferred if a palpable mass is found, if a patient is younger than 30 years, or if the patient is pregnant. Mammography and US are both useful if the patient has a palpable mass, is older than 30 years, and is not pregnant. [2] In patients younger than 30 years, the most appropriate modality is US because the patient is spared radiation exposure and because the likelihood for fibroadenoma is high. Mammography is not indicated as the primary imaging study in women younger than 30 years, unless high-risk factors are present. [3, 4]
Computed tomography (CT) scanning is not initially indicated for assessing a palpable lump in a woman in women younger than 30 years because of radiation exposure, the inability of CT to demonstrate microcalcifications, and the lack of specificity in the findings.
Magnetic resonance imaging (MRI) is not initially indicated for assessing a palpable lump in women younger than 30 years mainly because of its high cost and the high likelihood of false-positive findings. [5, 6, 7, 8, 9]
Positron emission tomography is expensive and is not universally available.
On mammograms, fibroadenomas typically appear as circumscribed oval or round masses, which occasionally have coarse calcifications. On ultrasonograms, fibroadenomas appear as circumscribed, homogeneous, oval, hypoechoic masses that may have gentle lobulations; a smooth, thin, echogenic capsule; variable acoustic enhancement; and homogeneity. On MRIs, fibroadenomas typically appear as smooth masses with high signal intensity on T2-weighted images and enhancement with the administration of gadolinium-based contrast agent.
Limitations of techniques
Mammography cannot be used to distinguish whether a mass is a fibroadenoma, a cyst, or a carcinoma with certainty because of some overlap in the findings. All of the entities may appear as smooth masses.
On ultrasonograms, fibroadenomas often demonstrate a typical appearance and may be distinguished clearly from cysts and carcinomas; however, fibrocystic disease with complicated hypoechoic cysts and, rarely, smooth carcinomas may mimic fibroadenoma. Atypical fibroadenomas, which are inhomogeneous or irregular in shape, may simulate carcinomas.
On MRIs, enhancement characteristics may help distinguish fibroadenomas from carcinomas, although the enhancement kinetics and morphologic features of the 2 tumors overlap. Fibroadenomas are hypointense or isointense lesions as compared with adjacent breast tissue on T1-weighted images, and they are hypointense or hyperintense on T2-weighted images.
With gadolinium, the majority of fibroadenomas are hyperintense, with slow initial contrast enhancement and a persistent delayed phase, but some have rapid enhancement and either a plateau or a washout phase. Large phyllodes tumors may typically have smooth margins, internal cysts, septations, and hemorrhage or perifocal or unilateral edema, but it is not possible to definitely differentiate between phyllodes tumors and fibroadenomas.
Septations occur in about half of fibroadenomas and have been reported to be a strong indicator of this diagnosis, but phyllodes tumors also may have septations.
Fibroadenomas may have a contrast-enhancement pattern suggestive of malignancy in up to one third of cases; on MRIs, they cannot be distinguished from phyllodes tumors with certainty.
Definitive diagnosis often requires palpation or image-guided biopsy.
Patient education
For patient education information, see the Cancer and Tumors Center and Women's Health Center, as well as Breast Cancer, Breast Lumps and Pain, and Breast Self-Exam.
Radiography
On mammograms, a fibroadenoma may be occult or may appear as a smooth-margined oval or round mass that is 4-100 mm in size. Occasionally, tumors contain coarse calcifications, which suggest infarction and involution. Calcifications may be useful in diagnosing the mass, but occasionally, they may mimic malignant microcalcifications. Although fibroadenomas often have coarse calcifications, cystosarcomas rarely have calcifications. The mammographic findings of fibroadenomas with hamartomas, cysts, and carcinomas overlap.
(For mammograms of fibroadenomas, see the images below.)
Partially circumscribed oval mass with some obscured margins in upper outer quadrant in craniocaudal view of mammogram in 32-year-old woman with palpable lump in same location.
Mediolateral-oblique mammogram view also demonstrates same circumscribed oval mass in same patient. While such a mass is likely a fibroadenoma, mammogram findings are not specific and ultrasound is needed for further evaluation.
Magnetic Resonance Imaging
Fibroadenomas appear as round or oval masses that are smooth or gently lobulated and enhance with gadolinium-based contrast material. Internal enhancement in homogeneity may be noted. [10, 11]
Morphology is of utmost importance for correct classification of benign lesions. Fibroadenomas are typically round, ovoid, or lobulated, with smooth margins; however, on early contrast-enhanced images, they may exhibit an irregular shape or margin resulting from the progression of enhancement. Therefore, morphology should be assessed on the noncontrast or late postcontrast images. Nonenhancing internal septa, which are best seen on T2-weighted images, are a specific indicator that a mass is a fibroadenoma; however, they are only seen in a minority of fibroadenomas.
Enhancement kinetics and characteristics are highly variable with fibroadenomas and may be dependent on the degree of fibrosis within the tumor. Enhancement rates of fibroadenomas overlap with those of breast cancers. Mean enhancement is slower in fibroadenomas than in cancers, but this is not useful in assessment of individual cases.
Gadolinium-based contrast agents have been linked to the development of nephrogenic systemic fibrosis (NSF) or nephrogenic fibrosing dermopathy (NFD). The disease has occurred in patients with moderate to end-stage renal disease after being given a gadolinium-based contrast agent to enhance MRI or MRA scans. NSF/NFD is a debilitating and sometimes fatal disease. Characteristics include red or dark patches on the skin; burning, itching, swelling, hardening, and tightening of the skin; yellow spots on the whites of the eyes; joint stiffness with trouble moving or straightening the arms, hands, legs, or feet; pain deep in the hip bones or ribs; and muscle weakness.
When internal septa are present in a smooth mass, the confidence that the mass is a fibroadenoma is high. When septa are not present, the findings of fibroadenomas and carcinomas overlap.
Ultrasonography
Fibroadenomas appear oval on ultrasonograms, and their width is larger than their anteroposterior diameter. Gentle lobulations (typically fewer than 4) may be present, but the margins should be circumscribed. [12, 5, 13, 14, 7, 8, 9]
Internal echogenicity may be homogeneous, and findings may range from isoechoic to lobules of fat to hypoechoic. The through-transmission of the tumor is variable. A thin echogenic capsule is typical of a fibroadenoma and indicates that the lesion is benign. A vague or thick surrounding region of echogenicity may indicate malignancy. Fibroadenomas do not have a true capsule; the thin echogenic capsule seen on ultrasonograms is a pseudocapsule caused by the compression of adjacent tissue.
Cysts seen in a solid mass are suggestive of cystosarcoma phyllodes rather than fibroadenomas.
One study found that histologic type, tumor size, and patient age significantly influence ultrasound characteristics of breast fibroadenomas. [6]
Breast ultrasound elastography is a sonographic imaging technique that may provide information on breast lesions in addition to conventional ultrasonography and mammography. Ultrasound elastography provides a noninvasive evaluation of a the "stiffness" of a lesion. Fibroadenomas have a tendency to have less stiffness and lower vascularity than phyllodes tumors. [15, 16]
Degree of confidence
Of masses with a thin, smooth echogenic capsule, 93% are benign. Of circumscribed masses, 91% are benign. Of masses that are round or oval, 94% are benign. Of fibroadenomas, 60% are oriented parallel to the skin (ie, they appear oval).
Overlap may exist between the US appearances of carcinomas, fibroadenomas, cystosarcoma phyllodes, and complicated cysts.
-
Circumscribed oval hypoechoic mass with gentle lobulation and slight shadowing, typical of fibroadenoma.
-
Partially circumscribed oval mass with some obscured margins in upper outer quadrant in craniocaudal view of mammogram in 32-year-old woman with palpable lump in same location.
-
Mediolateral-oblique mammogram view also demonstrates same circumscribed oval mass in same patient. While such a mass is likely a fibroadenoma, mammogram findings are not specific and ultrasound is needed for further evaluation.






