Practice Essentials
Lymphoma is the fifth most common cancer in the United States, with an annual incidence of 74,490 estimated cases. Approximately 88% of these cancers are non-Hodgkin lymphomas (NHLs). The incidence of NHL has doubled over the last 20 years because of the increase in AIDS-related lymphoma and the use of immunosuppressive drugs with organ transplantation and cancer chemotherapy. [1, 2, 3] Several rare congenital immunodeficiency syndromes may result in CNS lymphoma, including Wiskott-Aldrich syndrome, X-linked immunodeficiency, immunoglobulin A deficiency, and severe immunodeficiency syndrome. [4, 5, 6, 7, 8, 9, 10]
Primary lymphoma of the central nervous system is rare, representing about 1% of all lymphomas, less than 5% of all non-Hodgkin lymphoma, and 3-5% of brain tumors. [11, 12]
Magnetic resonance imaging (MRI) is the examination of choice for CNS lymphoma because of its high sensitivity and multiplanar capability. [13, 11, 14, 15] MRI scans typically show a single or multiple poorly demarcated masses, more or less deeply located within the brain parenchyma. These masses demonstrate uniform intense gadolinium enhancement with little or no edema. [16] Although sensitive, MRI characteristics are not specific for CNS lymphoma; however, MRI findings may be suggestive of lymphoma in the proper clinical setting. [17, 18, 19, 20]
(See the image below.)
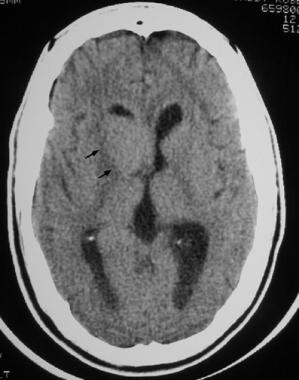 Nonenhanced CT scan of the head on a 56-year-old woman with a change in mental status shows a nodular, moderately hyperattenuating lesion adjacent to the right lateral ventricle, within the head of the caudate nucleus.
Nonenhanced CT scan of the head on a 56-year-old woman with a change in mental status shows a nodular, moderately hyperattenuating lesion adjacent to the right lateral ventricle, within the head of the caudate nucleus.
Approximately 10-30% of patients with systemic lymphoma have secondary CNS involvement [21, 22] ; primary lymphomas represent approximately 70-90% of all CNS lymphomas. Secondary systemic and primary CNS lymphomas have similar imaging characteristics. Meningeal involvement occurs commonly in patients with secondary lymphoma; it occurs less frequently in patients with primary lymphoma. Of patients with primary lymphoma, 75-85% present with supratentorial tumor. As many as 50% of patients present with multiple tumor nodules.
Gadolinium-based contrast agents have been linked to the development of nephrogenic systemic fibrosis (NSF) or nephrogenic fibrosing dermopathy (NFD). NSF/NFD has occurred in patients with moderate to end-stage renal disease after being given a gadolinium-based contrast agent to enhance MRI or MRA scans. NSF/NFD is a debilitating and sometimes fatal disease. Characteristics include red or dark patches on the skin; burning, itching, swelling, hardening, and tightening of the skin; yellow spots on the whites of the eyes; joint stiffness with trouble moving or straightening the arms, hands, legs, or feet; pain deep in the hip bones or ribs; and muscle weakness.
Computed Tomography
Nonenhanced computed tomography (CT) images typically show focal nodular areas of high attenuation, representing high tumor cellularity, with ill-defined margins and little surrounding vasogenic edema (see the first image below). Corresponding contrast-enhanced CT images usually demonstrate marked and diffuse enhancement of the lesions (see the second image below). [23, 24]
Nonenhanced CT scan of the head on a 56-year-old woman with a change in mental status shows a nodular, moderately hyperattenuating lesion adjacent to the right lateral ventricle, within the head of the caudate nucleus.
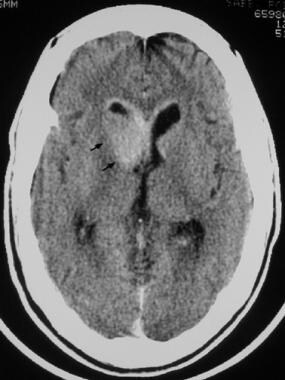 Intravenously contrast-enhanced CT scan of the head demonstrates a uniformly attenuating, enhancing mass lesion adjacent to the right lateral ventricle and ependymal enhancement in the frontal horns of the lateral ventricles.
Intravenously contrast-enhanced CT scan of the head demonstrates a uniformly attenuating, enhancing mass lesion adjacent to the right lateral ventricle and ependymal enhancement in the frontal horns of the lateral ventricles.
In patients with AIDS-related immunocompromise, lymphomas often appear as ring-enhancing lesions (see the image below) because of central areas of necrosis. The enhancing ring typically appears thick and nodular.
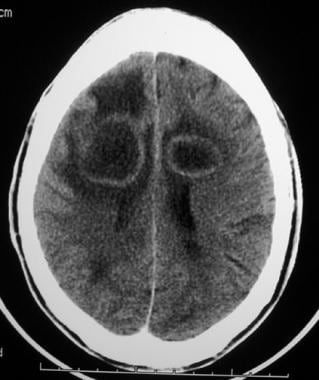 Nonenhanced head CT scan of a 38-year-old African American patient with HIV infection shows 2 bilateral, parietal, white matter lesions with central low attenuation and surrounding vasogenic edema.
Nonenhanced head CT scan of a 38-year-old African American patient with HIV infection shows 2 bilateral, parietal, white matter lesions with central low attenuation and surrounding vasogenic edema.
Calcifications do not occur in lymphoma, except rarely in patients who have undergone prior radiation therapy. Hemorrhage in lymphoma is rare. Contrast-enhancing, thickened ependyma may be seen.
In patients with immunodeficiency or immunosuppression, other lesions, such as toxoplasmosis, cryptococcosis, metastasis, and pyogenic abscess, may have the same ring-enhancing appearance as that of CNS lymphoma. Clinical correlation is necessary in diagnosis.
Although radiographic findings may suggest CNS lymphoma in the proper clinical setting, such findings are often not pathognomonic. Other lesions, such as toxoplasmosis, abscesses, cryptococcoma, glioma, and metastases, may have a similar appearance.
Magnetic Resonance Imaging
The most common locations on MRI include periventricular white matter, basal ganglia, and corpus callosum, while cerebellum, brainstem, and spinal cord are less frequently involved. [25] The classic appearance of CNS lymphoma on nonenhanced T1-weighted MRIs is that of an isointense to isointense to hypointense nodule or mass. On T2-weighted MRIs, the appearance is that of an isointense-to-hyperintense mass. On postgadolinium-enhanced T1-weighted MRIs, lymphoma tends to enhance intensely and diffusely. In patients with AIDS-related immunosuppression, a ringlike enhancing pattern is seen most often (see the images below). Often, little or no surrounding vasogenic edema is demonstrated. [26, 17, 18, 19]
 Axial gadolinium-enhanced T1-weighted MRI reveals the rim-enhancing lesions typical of HIV infection.
Axial gadolinium-enhanced T1-weighted MRI reveals the rim-enhancing lesions typical of HIV infection.
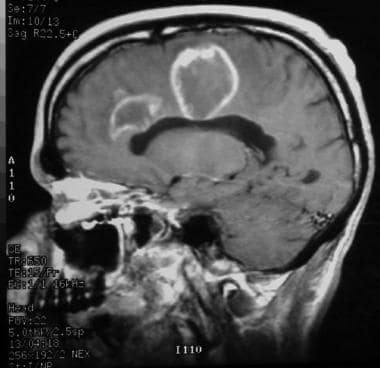 Sagittal T1-weighted contrast-enhanced MRI reveals 2 rim-enhancing lesions in this patient with HIV infection. The lesions extend to involve the corpus callosum.
Sagittal T1-weighted contrast-enhanced MRI reveals 2 rim-enhancing lesions in this patient with HIV infection. The lesions extend to involve the corpus callosum.
Tumor lesions may cross the midline and may appear as a butterfly tumor involving both cerebral hemispheres. In 30% of patients, leptomeningeal involvement is encountered, usually in secondary systemic lymphoma; in such cases, meningeal involvement is typical. Involvement of the perivascular spaces with contrast enhancement is strongly suggestive of CNS lymphoma (in such cases, lymphoma must be differentiated from sarcoidosis and CNS tuberculosis); involvement of the corpus callosum is also strongly suggestive of CNS lymphoma (in such cases, lymphoma must be differentiated from glioma and metastatic neoplasm). Contrast-enhancing, thickened ependyma may be seen. If such findings are seen in patients with AIDS, lymphoma must be differentiated from cytomegalovirus ependymitis; if such findings are encountered in patients who do not have AIDS, lymphoma must be differentiated from metastatic neoplasm, such as carcinoma of the lung or breast. In addition, in patients with these findings, lymphoma must be differentiated from ependymal spread of anaplastic glioma. [17, 18, 19, 27]
Leptomeningeal extension is depicted better on enhanced MRI scans than on CT scans.
Care should be taken, especially in cases involving ring-enhancing lesions, to differentiate lymphoma from other disorders, such toxoplasmosis, cryptococcosis, gliomas, and metastasis; on MRI, the appearance of these disorders may be similar to that of lymphoma.
Involvement of the corpus callosum is highly suggestive of CNS lymphoma, but such involvement also occasionally occurs with anaplastic glioma and metastatic neoplasm.
A study by Xi et al found that arterial spin labeling (ASL) and dynamic contrast-enhanced (DCE)-derived permeability parameters can help differentiate primary central nervous system lymphoma (PCNSL) from high-grade glioma (HGG) and brain metastasis. [28]
Nuclear Imaging
Thallium-201 single-photon emission computed tomography may demonstrate intense uptake of the radiotracer within tumor tissue. Carbon-11 methionine or 18-fluorodeoxyglucose positron emission tomography (18F-FDG PET) may show increased uptake within the tumor tissue. [29, 30] Because FDG-uptake on diffuse large B-cell lymphoma is higher than that on other types of lymphoma, it may be helpful in differentiating between primary central nervous system lymphoma (PCNSL) and gliomas. F18-FDG PET has been shown to have a diagnostic sensitivity in PCNSL of 76-100%. Maximum standardized uptake value (SUVmax) has been shown to be higher in PCNSL than in gliomas. Similarly, 18F-FDG PET can identify degenerative diseases, multiple sclerosis, infectious diseases, and cerebral infarction. [31] F18-FDG PET/CT may have a role in the assessment of extra-cerebral disease. [32, 33]
Angiography
On cerebral angiograms, lymphomas may simulate meningioma, with diffuse vascular staining in the late arterial or early venous phase, as well as meningeal enhancement. Arterial encasement and dilation of the deep medullary veins may be seen.
Angiographic findings are nonspecific for CNS lymphoma.
Questions & Answers
Overview
What is the prevalence of brain and CNS lymphoma?
What is the role of MRI in brain and CNS lymphoma imaging?
Which CT findings are characteristic of brain and CNS lymphoma?
Which MRI findings are characteristic of brain and CNS lymphoma?
How are brain and CNS lymphoma differentiated from other ring-enhancing lesions on MRI?
What is the role of F18-FDG PET scanning in brain and CNS lymphoma imaging?
Which angiography findings are characteristic of brain and CNS lymphoma?
-
Nonenhanced CT scan of the head on a 56-year-old woman with a change in mental status shows a nodular, moderately hyperattenuating lesion adjacent to the right lateral ventricle, within the head of the caudate nucleus.
-
Intravenously contrast-enhanced CT scan of the head demonstrates a uniformly attenuating, enhancing mass lesion adjacent to the right lateral ventricle and ependymal enhancement in the frontal horns of the lateral ventricles.
-
Nonenhanced head CT scan of a 38-year-old African American patient with HIV infection shows 2 bilateral, parietal, white matter lesions with central low attenuation and surrounding vasogenic edema.
-
Axial gadolinium-enhanced T1-weighted MRI reveals the rim-enhancing lesions typical of HIV infection.
-
Sagittal T1-weighted contrast-enhanced MRI reveals 2 rim-enhancing lesions in this patient with HIV infection. The lesions extend to involve the corpus callosum.









