Practice Essentials
In the past, multilocular cystic renal tumors were considered to be lesions of developmental origin, hamartomas, or hamartomas with malignant potential (see the images below). In 1956, Boggs and Kimmelstiel first proposed the true neoplastic nature of the lesions in a case report, suggesting the term benign multilocular cystic nephroma (MLCN) for this condition. [1, 2, 3] Joshi and Beckwith proposed a modification to the existing terminology. [4] Their modification emphasized a neoplastic rather than a developmental or hamartomatous origin. First, they recommended that the term cystic nephroma be used to describe a multicystic tumor lacking blastemal or other embryonal elements. Second, they suggested that the term cystic partially differentiated nephroblastoma (CPDN) be used to denote a predominantly cystic lesion without nodular solid regions and in which the septa contain blastemal or other embryonal elements. Furthermore, they proposed that both terms be used as subsets of the category term multilocular cystic renal tumor.
Multilocular cystic nephroma is a benign mixed mesenchymal and epithelial neoplasm of the kidney and is classically described as a benign slow-growing renal tumor. [5]
Patients who have multilocular cystic nephroma present with palpable mass, abdominal pain, and hematuria, as in renal cell carcinoma. Radiologically, multilocular cystic nephroma usually presents as a solitary, centrally located cystic lesion. It is difficult to differentiate multilocular cystic nephroma from multilocular cystic renal cell carcinoma with ultrasonography. Therefore, biopsy or excision is suggested for definitive diagnosis. [6] If left untreated, these tumors progressively increase in size and can become massive. [7, 5, 8, 9, 10]
Ultrasonography (US) is the first radiologic examination performed for the evaluation of any abdominal mass. US can provide the imaging results necessary for diagnosing multilocular cystic nephroma. The diagnosis may be confirmed by using either CT or MRI. Together, US and CT may be the studies of choice because they enable the evaluation of cystic lesions, stromal tissue, and the perfusion of this stroma. No flow is seen within the cystic lesions. [11, 12, 13, 14, 15, 8, 9]
The precision and accuracy of US depends on, and therefore is limited by, the operator's skill. CT may not be chosen if the patient has a severe allergy to the contrast medium. Compared with US and fast CT, MRI is limited by the need for sedation in some patients.
Multilocular cystic renal cell carcinoma cannot reliably be distinguished from cystic nephroma by physical or radiologic exam; immunohistochemical staining assay is often necessary for a definitive diagnosis. The Bosniak criteria is considered the reference standard for diagnosis and classification of cystic renal masses. [8, 9, 10]
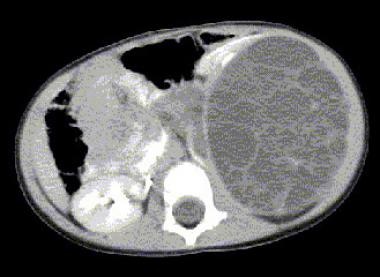 Multilocular cystic nephroma. CT shows a normal right kidney and an enlarged left kidney with a large well-defined mass, with several hypoattenuating cysts. No enhancement or septation is noted.
Multilocular cystic nephroma. CT shows a normal right kidney and an enlarged left kidney with a large well-defined mass, with several hypoattenuating cysts. No enhancement or septation is noted.
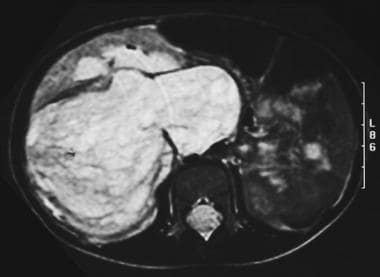 Multilocular cystic nephroma. Axial MRI shows a large multilocular cystic nephroma involving the right kidney and crossing the midline.
Multilocular cystic nephroma. Axial MRI shows a large multilocular cystic nephroma involving the right kidney and crossing the midline.
Radiography
On plain radiographs, cystic nephroma and cystic partially differentiated nephroblastoma (CPDN) cannot be distinguished, just as they cannot be distinguished by their gross anatomic appearances. However, in either type of multilocular cystic renal tumor, radiography does reveal displacement of the bowel and adjacent structures if the lesion is of sufficient size. Calcification, although uncommon, can be present and is defined as curvilinear and peripheral localizations. [16]
On excretory urography, the kidneys function normally with multilocular cystic renal tumors. Because the mass is rarely suspected on the basis of the clinical findings, excretory urography reveals nonspecific stretching, displacement, extension of the tumor to the renal pelvis, and attenuation of the renal collecting system by the mass. Delayed or absent excretion is also demonstrated.
A general nonspecific renal tumor can be identified by using radiography, with some degree of confidence. However, the use of radiography to diagnose multilocular cystic nephroma specifically results in a low degree of confidence. On plain radiographs, multilocular cystic renal tumor appears similar to other renal tumors because plain radiography cannot be used to differentiate between cystic and solid lesions.
Computed Tomography
CT findings are dependent on the size of the cyst and the amount of stromal tissue (see the images below). [13] In most cases, the mass is identified with the following CT findings [17] :
-
Well-defined margins
-
Multicystic architecture
-
Enhancing septa
-
Herniation into the renal collecting system
 Multilocular cystic nephroma. CT shows a normal right kidney and an enlarged left kidney with a large well-defined mass, with several hypoattenuating cysts. No enhancement or septation is noted.
Multilocular cystic nephroma. CT shows a normal right kidney and an enlarged left kidney with a large well-defined mass, with several hypoattenuating cysts. No enhancement or septation is noted.
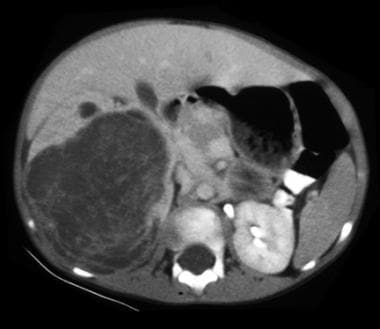
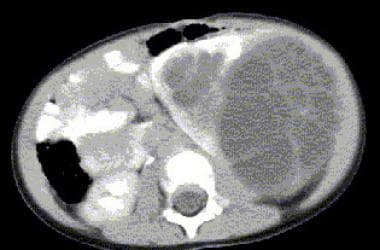 Multilocular cystic nephroma. CT shows a normal right kidney and an enlarged left kidney with a large well-defined mass, with several cysts with hypoattenuation. No enhancement or septation is noted. Perfusion can be seen crossing the midline on part of the remaining left kidney.
Multilocular cystic nephroma. CT shows a normal right kidney and an enlarged left kidney with a large well-defined mass, with several cysts with hypoattenuation. No enhancement or septation is noted. Perfusion can be seen crossing the midline on part of the remaining left kidney.
 Multilocular cystic nephroma. CT shows a normal right kidney and an enlarged left kidney with a large well-defined mass, with several cysts with hypoattenuation. No enhancement or septation is noted. Perfusion is seen crossing the midline on part of the remaining left kidney, with some signs of dilatation of the collecting system.
Multilocular cystic nephroma. CT shows a normal right kidney and an enlarged left kidney with a large well-defined mass, with several cysts with hypoattenuation. No enhancement or septation is noted. Perfusion is seen crossing the midline on part of the remaining left kidney, with some signs of dilatation of the collecting system.
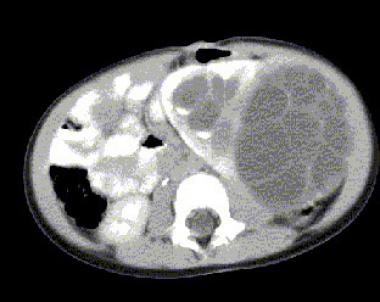 Multilocular cystic nephroma. CT shows a normal right kidney and an enlarged left kidney with a large well-defined mass, with several cysts with hypoattenuation. No enhancement or septation is noted. Perfusion is seen crossing the midline on part of the remaining left kidney, with some signs of dilatation of the collecting system.
Multilocular cystic nephroma. CT shows a normal right kidney and an enlarged left kidney with a large well-defined mass, with several cysts with hypoattenuation. No enhancement or septation is noted. Perfusion is seen crossing the midline on part of the remaining left kidney, with some signs of dilatation of the collecting system.
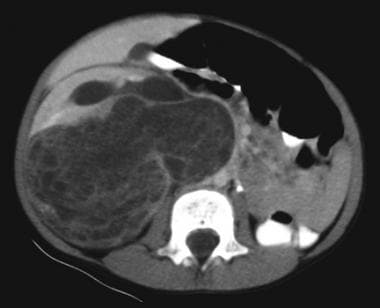
 Multilocular cystic nephroma. CT shows a large multilocular cystic nephroma involving the right kidney and crossing the midline.
Multilocular cystic nephroma. CT shows a large multilocular cystic nephroma involving the right kidney and crossing the midline.
 Multilocular cystic nephroma. CT shows a large multilocular cystic nephroma involving the right kidney and crossing the midline.
Multilocular cystic nephroma. CT shows a large multilocular cystic nephroma involving the right kidney and crossing the midline.





Cystic spaces are not enhancing and demonstrate CT numbers slightly higher than those of water. In some cases, the entire mass or portions of the mass may appear solid because of smaller closely spaced cysts.
CT results in a high degree of confidence in the diagnosis of multilocular cystic nephroma. CT images define the structures of lesions on the kidneys well.
False-positive and false-negative rates are low because of the accuracy of the method.
Magnetic Resonance Imaging
MRI demonstrates the low signal intensity of the tumor capsule (see the images below). MRI has a high degree of confidence in the diagnosis of multilocular cystic nephroma. MRI images define the structures of lesions on the kidneys well. False-positive and false-negative rates are low because of the accuracy of the method.
Observations of nonenhanced MRIs have shown encapsulated masses with dividing septa between cystic spaces.
Kettritz et al [18] found the following:
-
On T1-weighted sequences, signal intensity varied from low to very high and from low to intermediate.
-
T2-weighted sequencing resulted in low signal intensity in the tumor capsule and the intermediate septations.
-
The signal intensity of the cysts was high in all cases.
-
Variable signal intensity from the cyst contents was attributed to differing concentrations of old hemorrhage and protein.
Multilocular cystic nephroma. Axial MRI shows a large multilocular cystic nephroma involving the right kidney and crossing the midline.
 Multilocular cystic nephroma. Axial MRI shows a large multilocular cystic nephroma involving the right kidney and crossing the midline.
Multilocular cystic nephroma. Axial MRI shows a large multilocular cystic nephroma involving the right kidney and crossing the midline.
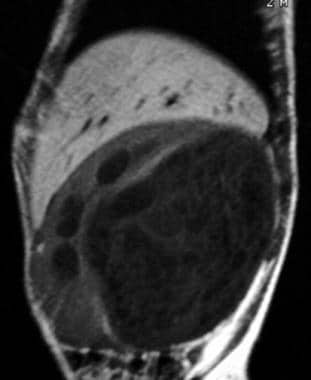 Multilocular cystic nephroma. Sagittal MRI shows a large multilocular cystic nephroma involving the right kidney.
Multilocular cystic nephroma. Sagittal MRI shows a large multilocular cystic nephroma involving the right kidney.
Ultrasonography
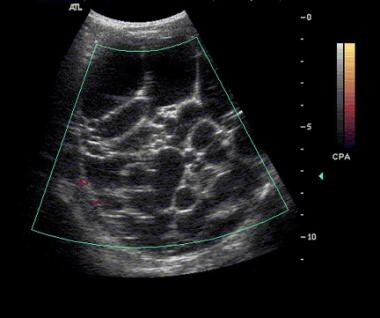
Results of ultrasonography depend on the amount of stroma and the size of the loculi (see the images below). [19, 14] The appearance of multilocular cystic renal tumor includes multiple anechoic spaces separated by hyperechoic septa. This pattern is similar to that of multilocular cystic nephroma; however, if the loculi are small, the tumor mimics an echogenic solid mass. US can be used with a high degree of confidence. A diagnosis can be made with high precision because sonograms clearly depict the structure of the lesions. False-positive and false-negative rates are low because of the accuracy of the method.
In most patients, the renal origin of the mass can be confirmed by identifying a beak or claw of normal renal parenchyma around the periphery of a well-defined mass, by the splaying or displacement of the renal collecting system, and by synchronous motion of the mass and kidney with respiratory excursion.
Color Doppler US can also be used to evaluate tumors and can provide a noninvasive assessment of lesion vascularity. [6] This is possible because of the Doppler-shifted signals of abnormally high velocity emitted by low-resistance neovascularity in some neoplasms.
 Multilocular cystic nephroma. Sonograms show a normal right kidney and, within an enlarged left kidney, multiple anechoic cystic changes separated by hyperechoic septa.
Multilocular cystic nephroma. Sonograms show a normal right kidney and, within an enlarged left kidney, multiple anechoic cystic changes separated by hyperechoic septa.
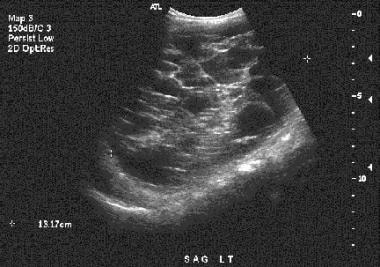 Multilocular cystic nephroma. Sonogram shows multiple anechoic cystic changes separated by hyperechoic septa within an enlarged left kidney.
Multilocular cystic nephroma. Sonogram shows multiple anechoic cystic changes separated by hyperechoic septa within an enlarged left kidney.
 Multilocular cystic nephroma. Sonogram shows multiple anechoic cystic changes separated by hyperechoic septa within an enlarged left kidney.
Multilocular cystic nephroma. Sonogram shows multiple anechoic cystic changes separated by hyperechoic septa within an enlarged left kidney.
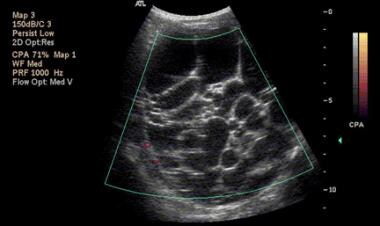 Multilocular cystic nephroma. Color Doppler sonogram shows multiple anechoic cystic changes separated by hyperechoic septa within an enlarged left kidney without Doppler flow.
Multilocular cystic nephroma. Color Doppler sonogram shows multiple anechoic cystic changes separated by hyperechoic septa within an enlarged left kidney without Doppler flow.
 Multilocular cystic nephroma. Color Doppler sonogram shows multiple anechoic cystic changes separated by hyperechoic septa within an enlarged left kidney without Doppler flow.
Multilocular cystic nephroma. Color Doppler sonogram shows multiple anechoic cystic changes separated by hyperechoic septa within an enlarged left kidney without Doppler flow.
Angiography
On angiographic examination, multilocular cystic renal tumors usually appear hypovascular, although they may also be avascular or hypervascular. Angiography may reveal features that are not specific for differential diagnosis. Magnetic resonance angiography may help if a preoperative evaluation of the vascular anatomy is needed.
Angiography has a high degree of confidence. The structures of lesions on the kidneys are well differentiated with this method, which results in a precise diagnosis. As a result, angiography has low false-positive and false-negative rates.
-
Multilocular cystic nephroma. CT shows a normal right kidney and an enlarged left kidney with a large well-defined mass, with several hypoattenuating cysts. No enhancement or septation is noted.
-
Multilocular cystic nephroma. CT shows a normal right kidney and an enlarged left kidney with a large well-defined mass, with several cysts with hypoattenuation. No enhancement or septation is noted. Perfusion can be seen crossing the midline on part of the remaining left kidney.
-
Multilocular cystic nephroma. CT shows a normal right kidney and an enlarged left kidney with a large well-defined mass, with several cysts with hypoattenuation. No enhancement or septation is noted. Perfusion is seen crossing the midline on part of the remaining left kidney, with some signs of dilatation of the collecting system.
-
Multilocular cystic nephroma. CT shows a normal right kidney and an enlarged left kidney with a large well-defined mass, with several cysts with hypoattenuation. No enhancement or septation is noted. Perfusion is seen crossing the midline on part of the remaining left kidney, with some signs of dilatation of the collecting system.
-
Multilocular cystic nephroma. CT shows a large multilocular cystic nephroma involving the right kidney and crossing the midline.
-
Multilocular cystic nephroma. CT shows a large multilocular cystic nephroma involving the right kidney and crossing the midline.
-
Multilocular cystic nephroma. Sonograms show a normal right kidney and, within an enlarged left kidney, multiple anechoic cystic changes separated by hyperechoic septa.
-
Multilocular cystic nephroma. Sonogram shows multiple anechoic cystic changes separated by hyperechoic septa within an enlarged left kidney.
-
Multilocular cystic nephroma. Sonogram shows multiple anechoic cystic changes separated by hyperechoic septa within an enlarged left kidney.
-
Multilocular cystic nephroma. Color Doppler sonogram shows multiple anechoic cystic changes separated by hyperechoic septa within an enlarged left kidney without Doppler flow.
-
Multilocular cystic nephroma. Color Doppler sonogram shows multiple anechoic cystic changes separated by hyperechoic septa within an enlarged left kidney without Doppler flow.
-
Multilocular cystic nephroma. Axial MRI shows a large multilocular cystic nephroma involving the right kidney and crossing the midline.
-
Multilocular cystic nephroma. Axial MRI shows a large multilocular cystic nephroma involving the right kidney and crossing the midline.
-
Multilocular cystic nephroma. Sagittal MRI shows a large multilocular cystic nephroma involving the right kidney.



