Practice Essentials
Secondary hyperparathyroidism (SHPT) is characterized by pronounced parathyroid gland hyperplasia resulting from end-organ resistance to parathyroid hormone (PTH). The consequent hypersecretion of PTH depresses calcium levels. The most important cause of secondary hyperparathyroidism is chronic renal insufficiency. The clinical manifestations of secondary hyperparathyroidism include bone and joint pain and limb deformities, with symptoms worsening as PTH levels increase. [1, 2, 3] The characteristics of the disease that are displayed radiologically in the skeleton are similar to those of primary hyperparathyroidism.
(See the image below.)
 Radiograph of the left hand of a 6-year-old girl with chronic renal failure shows ulnar bowing of the distal radius and ulna, mild widening of the growth plates associated with a slight irregularity of the metaphyseal margins, coarsening of the trabecular pattern, and periosteal new bone formation around the metaphyses of the metacarpals and phalanges. The appearance is that of rickets and/or renal osteodystrophy. Note that bone aging is retarded.
Radiograph of the left hand of a 6-year-old girl with chronic renal failure shows ulnar bowing of the distal radius and ulna, mild widening of the growth plates associated with a slight irregularity of the metaphyseal margins, coarsening of the trabecular pattern, and periosteal new bone formation around the metaphyses of the metacarpals and phalanges. The appearance is that of rickets and/or renal osteodystrophy. Note that bone aging is retarded.
Imaging modalities
Radiographs are the mainstay of the radiologic diagnosis of secondary hyperparathyroidism, because the predominant changes are skeletal, with abnormal calcifications at various sites; these calcifications are well depicted on conventional radiographs. [4] The changes observed on radionuclide studies are not consistent or specific. The diagnosis is made or incidentally suggested because radionuclide investigation is initially performed for the evaluation of conditions other than secondary hyperparathyroidism, such as bone pain. Similarly, computed tomography (CT) scan findings are usually incidental, and CT scanning is not specifically performed for the diagnosis of secondary hyperparathyroidism. Ultrasonography may be useful in evaluating enlarged parathyroid glands. [5, 6, 7, 8]
Some studies have recommended routine preoperative 99mTc-sestamibi scans, while others have recommended such scanning only for selected patients. [5, 2, 9, 10, 11, 12, 13] In a study of 60 patients with 229 lesions, Zhang et al reported that early 99mTc-MIBI SPECT/CT, to detect hyperplastic parathyroid glands in patients with secondary hyperparathyroidism, was superior to that of ultrasonography, dual-phase 99mTc-MIBI scintigraphy, and delayed 99mTc-MIBI SPECT/CT. [2]
Subperiosteal erosions, periosteal reactions, and several other osseous abnormalities in secondary hyperparathyroidism are not specific for the disease and may occur in other skeletal disorders or conditions, as well as in primary hyperparathyroidism. The exact sensitivity of plain radiography in the diagnosis of secondary hyperparathyroidism is not known, but the fact that biochemical abnormalities may precede radiologic change is well recognized.
Radionuclide findings are not specific, and pure osteomalacia and primary hyperparathyroidism can result in an appearance similar to that of secondary hyperparathyroidism. As with radiographic findings, CT scan depictions of the osseous changes are nonspecific. Ultrasonography may not always show hyperplasia of the parathyroid glands.
Radiography
Radiography is the most important investigational modality in the diagnosis of secondary hyperparathyroidism; radiographs may show several skeletal abnormalities. The radiologic features of secondary hyperparathyroidism are similar to those of the primary form of the disease. The combination of 2 pathologic processes of hyperparathyroidism and osteomalacia and/or rickets is responsible for the osseous abnormalities in renal osteodystrophy. [14]
(See the images below.)
 Radiograph of the dorsal spine shows the classic rugger-jersey spine. This results from ill-defined bands of increased bone density adjacent to the vertebral endplates.
Radiograph of the dorsal spine shows the classic rugger-jersey spine. This results from ill-defined bands of increased bone density adjacent to the vertebral endplates.
 Radiograph of both hands of a 36-year-old woman receiving long-term hemodialysis shows subperiosteal bone resorption affecting the radial aspect of the middle phalanges of the fingers. Note the extensive digital arterial calcification.
Radiograph of both hands of a 36-year-old woman receiving long-term hemodialysis shows subperiosteal bone resorption affecting the radial aspect of the middle phalanges of the fingers. Note the extensive digital arterial calcification.
 Posteroanterior (PA) chest radiograph in a 60-year-old woman shows subligamentous bone resorption of the inferior surface of the lateral ends of the clavicles.
Posteroanterior (PA) chest radiograph in a 60-year-old woman shows subligamentous bone resorption of the inferior surface of the lateral ends of the clavicles.
 Radiograph of the dorsal spine of an adult male shows the classic rugger-jersey spine caused by ill-defined bands of increased bone density adjacent to the vertebral endplates.
Radiograph of the dorsal spine of an adult male shows the classic rugger-jersey spine caused by ill-defined bands of increased bone density adjacent to the vertebral endplates.
 Radiograph of the feet shows fairly large para-articular erosions in the heads of the right third and fourth metatarsal bones. Note the organized periosteal reaction around the shafts of those bones.
Radiograph of the feet shows fairly large para-articular erosions in the heads of the right third and fourth metatarsal bones. Note the organized periosteal reaction around the shafts of those bones.
 Anteroposterior (AP) radiograph of the right knee of a 55-year-old man receiving chronic hemodialysis. The patient presented with a red, hot, painful knee. Microscopic analysis of the joint aspirate revealed pyrophosphate crystals. The diagnosis was pseudogout. The radiograph shows chondrocalcinosis.
Anteroposterior (AP) radiograph of the right knee of a 55-year-old man receiving chronic hemodialysis. The patient presented with a red, hot, painful knee. Microscopic analysis of the joint aspirate revealed pyrophosphate crystals. The diagnosis was pseudogout. The radiograph shows chondrocalcinosis.
In children, widening of the growth plates of the long bones may be present, with irregularity of the metaphyseal margins and disorganization of the growth plate, which is indicative of advanced rickets. These changes of gross disease have been likened to the rotting of a wooden post at its stem.
(See the image below.)
Radiograph of the left hand of a 6-year-old girl with chronic renal failure shows ulnar bowing of the distal radius and ulna, mild widening of the growth plates associated with a slight irregularity of the metaphyseal margins, coarsening of the trabecular pattern, and periosteal new bone formation around the metaphyses of the metacarpals and phalanges. The appearance is that of rickets and/or renal osteodystrophy. Note that bone aging is retarded.
Severe osteopenia may be complicated by pathologic fractures. Epiphyseal displacement of metaphyseal fractures may be present; the most commonly involved sites include the distal radius, the proximal humerus, the distal femur, and the heads of metacarpal and metatarsal bones. [15]
Skeletal maturation may be retarded. Lateral Blount disease may occur as a result of lateral angulation of the proximal tibial epiphysis and genu valgum. Jaw enlargement has been described.
In adults, subperiosteal bone resorption characteristically affects the phalangeal tufts, the radial aspect of the proximal and middle phalanges of the fingers, the metatarsals, the rib margins, the lamina dura, and the medial margins of the proximal humerus, femur, and tibia.
Intracortical bone resorption, which results in a lacy appearance, involves the cortex of the metacarpals. Endosteal resorption may involve the phalanges of the digits. Subligamentous bone resorption affects the tuberosities of the humerus, the ischium, and the greater and lesser femoral trochanters, as well as the inferior surface of the lateral end of the clavicle and the inferior surface of the calcaneus. Subchondral resorption occurs at several sites, including the sternoclavicular and acromioclavicular joints, the symphysis pubis, the sacroiliac joints, and the discovertebral joints. An erosive-type arthropathy is reported with secondary hyperparathyroidism.
Brown tumors occur, but these are less common with secondary hyperparathyroidism than they are with primary hyperparathyroidism. However, as the life expectancy of patients with chronic renal disease has increased, brown tumors have increasingly been identified with renal osteodystrophy. Brown tumors may occur in the spine and form expansile masses, which can be complicated by paraplegia. Brown tumors of the sellar and/or parasellar regions and face may appear as destructive lesions.
(See the images below.)
 Radiograph in a 53-year-old woman with nutritional osteomalacia shows a brown tumor in the region of the tibial tuberosity (left) and healing of the lesion after vitamin D therapy (right). Also note improved mineralization of the bones.
Radiograph in a 53-year-old woman with nutritional osteomalacia shows a brown tumor in the region of the tibial tuberosity (left) and healing of the lesion after vitamin D therapy (right). Also note improved mineralization of the bones.
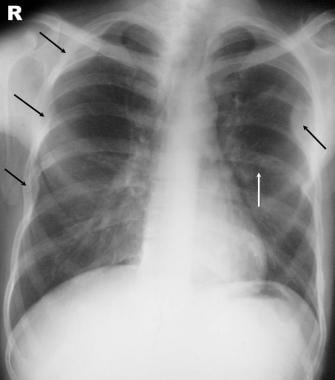 Posteroanterior (PA) chest radiograph shows multiple expansile brown tumors in the medial border of the left scapula and in several of the ribs (black arrows). Also note subperiosteal bone resorption along one of the rib margins (white arrow).
Posteroanterior (PA) chest radiograph shows multiple expansile brown tumors in the medial border of the left scapula and in several of the ribs (black arrows). Also note subperiosteal bone resorption along one of the rib margins (white arrow).
 Radiograph of the pelvis (same patient as in the previous image) shows multiple brown tumors (arrows).
Radiograph of the pelvis (same patient as in the previous image) shows multiple brown tumors (arrows).
The skull may show a granular pattern, which may be associated with thickening, particularly in the inner table (see the image below). Osteomalacia may be predominant in patients with renal osteodystrophy. Associated Looser transformation zones and pathologic fractures, possibly symmetric, can be present. Osteosclerosis may affect the epiphyses, metaphyses, pelvis, and ribs. Frequently, a classic rugger-jersey spine is observed; it is caused by ill-defined bands of increased bone density adjacent to the vertebral endplates.
 Plain radiograph of the skull of a 39-year-old woman demonstrates malabsorption syndrome with the biochemical features of osteomalacia. The image shows a granular pattern of the skull. Note the brown tumor (arrow).
Plain radiograph of the skull of a 39-year-old woman demonstrates malabsorption syndrome with the biochemical features of osteomalacia. The image shows a granular pattern of the skull. Note the brown tumor (arrow).
An organized periosteal reaction (eg, periosteal neostasis) may develop around the metatarsals, femora, and pelvis. This finding, although not typical, is more common in secondary hyperparathyroidism than it is in the primary form of disease. Generalized osteopenia, often severe, may occur. Digital phalangeal brachydactyly secondary to healed renal osteodystrophy may be present. Rarely, kyphoscoliosis may occur.
Extra-osseous calcification is more common in secondary hyperparathyroidism than it is in the primary form of the disease, and it is even more common in long-standing disease. Abnormal calcification and other abnormalities include the following:
-
Tumoral calcification associated with bone erosions
-
Chondrocalcinosis
-
Vascular calcification
-
Calcified pulmonary nodules
-
Cerebral subcortical calcification
-
Calcification within the eyes
-
Layering of soft-tissue calcification
-
Cardiac calcifications
-
Breast calcifications
-
Renal calcification
-
Hepatic calcification
Degree of confidence
In renal osteodystrophy, bone resorption is invariably present. Correlation of findings with the patient's history and biochemical parameters should lead to the correct diagnosis. However, secondary hyperparathyroidism associated with osteomalacia of dietary origin may cause vague symptoms and, sometimes, nonspecific biochemical findings.
The radiologic features of secondary hyperparathyroidism are similar to those of the disease's primary form. The radiologic changes can sometimes mimic those observed in Paget disease.
Computed Tomography
CT scan findings in renal osteodystrophy include the following [16] :
-
Abnormal sacroiliac joints
-
Multiple brown tumors
-
Osteitis fibrosa cystica
-
Prominent Schmorl nodes
-
Periarticular tumoral calcifications
-
Slipped capital femoral epiphyses
Layering of soft-tissue calcification is well demonstrated on CT scans. In general, however, and in comparison with other modalities, CT scanning offers no advantage in the diagnosis of secondary hyperparathyroidism.
Degree of confidence
CT scanning is rarely employed in screening exams for renal osteodystrophy. [16] Nonetheless, knowledge of the CT scan appearances of secondary hyperparathyroidism is important; it helps clinicians avoid confusing the changes associated with secondary hyperparathyroidism with those resulting from other pathologic conditions. On the whole, however, CT scanning is not sensitive in the detection of changes related to secondary hyperparathyroidism.
Soft-tissue calcification is not specific to secondary hyperparathyroidism and has myriad causes. Erosive changes attributable to secondary hyperparathyroidism may easily be confused with changes in rheumatoid arthritis, seronegative spondyloarthropathies, infection, or even malignancy. Brown tumors and amyloid deposition can easily be mistaken for a neoplastic process.
Magnetic Resonance Imaging
Magnetic resonance imaging (MRI) can adequately reveal skeletal deformity, cortical thickening, and irregular trabecular patterns in children with renal osteodystrophy. [16, 17] In addition, MRI shows osteonecrosis and intraosseous soft-tissue masses more conspicuously than do plain radiographs. This modality also shows diffuse, nonspecific marrow changes. [18] One case describes the MRI diagnosis of thoracic myelopathy caused by spinal stenosis secondary to renal osteodystrophy. [19] MRI is also useful in the detection of parathyroid hyperplasia.
Based on current experience, MRI findings in secondary hyperparathyroidism are not specific enough for this modality to replace radiography. Also, MRI has low sensitivity and specificity in the detection of parathyroid hyperplasia.
MRI findings in chronic osteodystrophy can often mimic those of other diseases.
Ultrasonography
Ultrasonography is useful in the detection of parathyroid enlargement. [20, 21] However, the sensitivity of ultrasonography in the detection of parathyroid hyperplasia is low. Imaging modalities in secondary hyperparathyroidism are of a limited value in guiding medical and surgical treatment. However, if percutaneous alcohol ablation is contemplated as an adjunct to medical treatment, ultrasonography may be useful in the initial localization of an abnormal gland.
Ultrasonography has a high rate of false-negative findings in the diagnosis of parathyroid hyperplasia. A thyroid tumor may mimic a parathyroid adenoma.
Nuclear Imaging
Several radionuclide features are reported in secondary hyperparathyroidism (see the images below). A superscan may reveal the following findings [5, 6, 7, 8] :
-
Diffusely increased activity in bones, specifically in the axial skeleton, calvaria, mandible, costochondral junctions, long bones, and sternum
-
An increased bone-to–soft tissue ratio
-
Absent kidney and urinary bladder findings
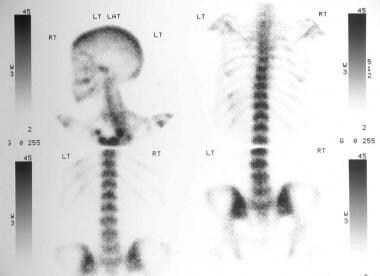 Superscan shows diffusely increased activity in the axial skeleton and perhaps in the calvaria and mandible. The ratio of bone to soft tissue is increased, and the kidneys and urinary bladder are absent.
Superscan shows diffusely increased activity in the axial skeleton and perhaps in the calvaria and mandible. The ratio of bone to soft tissue is increased, and the kidneys and urinary bladder are absent.

Diffuse uptake of a radionuclide (eg, technetium-99m [99mTc] methylene diphosphonate [MDP]) may occur in the lungs. Metaphyseal fractures may be cold on 99mTc MDP scans. Radionuclide uptake may be observed in ectopic calcific deposits. (See the image below.)
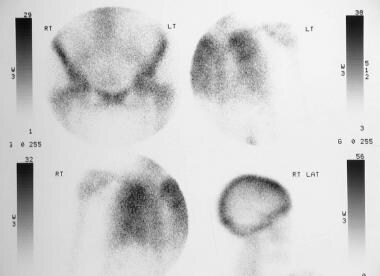 Technetium-99m bone scan in a patient with chronic renal disease shows uptake in the lungs and calvaria. No renal or bladder activity was noted. (The kidneys are not shown.)
Technetium-99m bone scan in a patient with chronic renal disease shows uptake in the lungs and calvaria. No renal or bladder activity was noted. (The kidneys are not shown.)
Technetium-99m sestamibi and subtraction scintigraphy with thallium-201 (201Tl) and 99mTc have been used to localize parathyroid hyperplasia in secondary hyperparathyroidism, but they are of limited value. [21, 22, 23, 24, 25, 26]
Some studies have recommended routine preoperative 99mTc-sestamibi scans, while others have recommended such scanning only for selected patients. [5, 2, 9, 10, 11, 12, 13] In a study of 60 patients with 229 lesions, Zhang et al reported that early 99mTc-MIBI SPECT/CT, to detect hyperplastic parathyroid glands in patients with secondary hyperparathyroidism, was superior to that of ultrasonography, dual-phase 99mTc-MIBI scintigraphy, and delayed 99mTc-MIBI SPECT/CT. [2]
Degree of confidence
Radionuclide bone scans have low sensitivity and specificity in the detection of secondary hyperparathyroidism. The use of radionuclides in the diagnosis of parathyroid hyperplasia also has a limited role.
Besides renal osteodystrophy and/or hyperparathyroidism, the following conditions, displaying the same features as hyperparathyroidism, may appear to be present:
-
Hyperthyroidism
-
Extensive skeletal metastases
-
Aplastic anemia
-
Leukemia
-
Widespread Paget disease
-
Myelofibrosis and/or myelosclerosis
-
Waldenström macroglobulinemia
-
Systemic mastocytosis
Findings on a superscan may be interpreted as normal in patients with poor renal function.
In a study by Taieb et al, the most common causes of false-positive results on parathyroid scintigraphy were the presence of thyroid nodules, thymoma, and metastatic and inflammatory lymph nodes. [2, 9]
-
Radiograph of the left hand of a 6-year-old girl with chronic renal failure shows ulnar bowing of the distal radius and ulna, mild widening of the growth plates associated with a slight irregularity of the metaphyseal margins, coarsening of the trabecular pattern, and periosteal new bone formation around the metaphyses of the metacarpals and phalanges. The appearance is that of rickets and/or renal osteodystrophy. Note that bone aging is retarded.
-
Radiograph of the dorsal spine shows the classic rugger-jersey spine. This results from ill-defined bands of increased bone density adjacent to the vertebral endplates.
-
Radiograph of both hands of a 36-year-old woman receiving long-term hemodialysis shows subperiosteal bone resorption affecting the radial aspect of the middle phalanges of the fingers. Note the extensive digital arterial calcification.
-
Plain radiograph of the skull of a 39-year-old woman demonstrates malabsorption syndrome with the biochemical features of osteomalacia. The image shows a granular pattern of the skull. Note the brown tumor (arrow).
-
Posteroanterior (PA) chest radiograph in a 60-year-old woman shows subligamentous bone resorption of the inferior surface of the lateral ends of the clavicles.
-
Radiograph of the dorsal spine of an adult male shows the classic rugger-jersey spine caused by ill-defined bands of increased bone density adjacent to the vertebral endplates.
-
Radiograph in a 53-year-old woman with nutritional osteomalacia shows a brown tumor in the region of the tibial tuberosity (left) and healing of the lesion after vitamin D therapy (right). Also note improved mineralization of the bones.
-
Posteroanterior (PA) chest radiograph shows multiple expansile brown tumors in the medial border of the left scapula and in several of the ribs (black arrows). Also note subperiosteal bone resorption along one of the rib margins (white arrow).
-
Radiograph of the pelvis (same patient as in the previous image) shows multiple brown tumors (arrows).
-
Radiograph of the feet shows fairly large para-articular erosions in the heads of the right third and fourth metatarsal bones. Note the organized periosteal reaction around the shafts of those bones.
-
Anteroposterior (AP) radiograph of the right knee of a 55-year-old man receiving chronic hemodialysis. The patient presented with a red, hot, painful knee. Microscopic analysis of the joint aspirate revealed pyrophosphate crystals. The diagnosis was pseudogout. The radiograph shows chondrocalcinosis.
-
Occasionally, patients with chronic renal failure may present with biochemical and radiographic features of osteomalacia. This plain radiograph of the pelvis of a 77-year-old woman shows multiple pseudofractures. Note the osteosclerosis and a brown tumor in the region of the intertrochanteric line of the left femur.
-
Superscan shows diffusely increased activity in the axial skeleton and perhaps in the calvaria and mandible. The ratio of bone to soft tissue is increased, and the kidneys and urinary bladder are absent.
-
Technetium-99m bone scan in a patient with chronic renal disease shows uptake in the lungs and calvaria. No renal or bladder activity was noted. (The kidneys are not shown.)






