Practice Essentials
Enchondromas are benign cartilaginous neoplasms that are usually solitary lesions in intramedullary bone occurring most commonly in small bones of the hands and feet. The distal femur and proximal humerus are other, less common locations. Enchondromas constitute 3-10% of all bone tumors and 12-24% of benign bone tumors. They are the second most common benign tumor, after osteochondroma. [1] The primary significant factors of enchondromas are related to their complications, most notably pathologic fracture, and malignant transformation, which may be associated with pathologic fracture. [2, 3]
The lesions replace normal bone with mineralized or unmineralized hyaline cartilage, thereby generating a lytic pattern on radiographs or, more commonly, a lytic area containing rings and arcs of chondroid calcifications. The lesions likely arise from cartilaginous rests that are displaced from the growth plate.
Diagnostic confirmation requires histopathologic examination. Enchondromas are defined by punctate calcifications of the chondroid matrix and are usually smaller than 3 cm. The most common presenting symptoms are pain, swelling, and deformity. Patients with enchondromas are usually 15 to 35 years of age, but enchondromatosis typically presents before the age of 10 years. Management of enchondromas typically consists of simple curettage with bone grafting, with the bone void filled with autograft, allograft, bone substitute, or bone cement. [4, 5, 6]
(See the images below.)
 Enchondroma. Frontal radiograph of the right hand demonstrates a lytic expansile lesion in the fifth metacarpal bone, with thinning of the cortex that has a somewhat scalloped appearance. A pathologic fracture is noted, but no appreciable calcifications are seen in the lesion.
Enchondroma. Frontal radiograph of the right hand demonstrates a lytic expansile lesion in the fifth metacarpal bone, with thinning of the cortex that has a somewhat scalloped appearance. A pathologic fracture is noted, but no appreciable calcifications are seen in the lesion.
 Enchondroma. Frontal radiograph of the left hand demonstrates an expansile lytic lesion in the proximal phalanx of the fifth digit with a distinct zone of transition, thinning of the cortex, and a pathologic fracture. The lesion involves the diaphysis and approaches the end of the bone near the metacarpophalangeal joint. This finding is not uncommon in enchondromas of the small bones. Note the fuzzy calcifications in the matrix of the lesion.
Enchondroma. Frontal radiograph of the left hand demonstrates an expansile lytic lesion in the proximal phalanx of the fifth digit with a distinct zone of transition, thinning of the cortex, and a pathologic fracture. The lesion involves the diaphysis and approaches the end of the bone near the metacarpophalangeal joint. This finding is not uncommon in enchondromas of the small bones. Note the fuzzy calcifications in the matrix of the lesion.
 Enchondroma. 62-year-old woman with enchondroma involving the proximal end of the proximal phalanx of her middle finger. The lesion has a lobular morphology and punctate calcifications. Because of pain, the lesion was curetted and packed with morselized allograft bone.
Enchondroma. 62-year-old woman with enchondroma involving the proximal end of the proximal phalanx of her middle finger. The lesion has a lobular morphology and punctate calcifications. Because of pain, the lesion was curetted and packed with morselized allograft bone.
Enchondromas are the most common tumors of the bones of the hand. In a study of 48 patients by Sollaci et al, tumors more frequently presented in the ulnar side of the hand, in the fifth ray and the proximal bones. [7]
When multiple enchondromas coexist, the diagnosis of enchondromatosis should be considered. Multiple enchondromas may occur in the following distinct disorders:
-
Ollier disease is a nonhereditary disorder characterized by multiple enchondromas with a prevalence of 1 in 100,000. [8] Enchondromas have a predilection for unilateral distribution and frequently affect the long tubular bones, particularly the tibia, the femur, and/or the fibula; flat bones, especially the pelvis, can also be affected. A case of Ollier disease located in the anterior ribs has been reported. [9] The enchondromas can grow large and can be disfiguring. [10, 11, 12, 13]
-
Maffucci syndrome is a congenital nonhereditary condition. It is less common than Ollier disease, and fewer than 200 cases have been reported in the United States. It usually presents before the onset of puberty and is often located within the long bones. [14] This syndrome results in multiple hemangiomas in addition to enchondromas. [15, 16, 17] An estimated 25-30% of enchondromas develop into chondrosarcoma. There is also an increased risk of malignant transformation of hemangiomas into hemangiosarcomas and hemangioendotheliomas. [17]
-
Metachondromatosis is a very rare genetic disorder, with less than 30 reported cases. It is characterized by multiple enchondromas and osteochondromas. It has been linked to mutations in the PTPN11 gene and is inherited in an autosomal dominant manner. [18] The first signs occur before puberty. Osteochondromas most commonly occur in the hands and feet, and enchondromas typically involve the iliac crests and metaphyses of long bones.
-
Spondyloenchondrodysplasia (SPENCD) is a rare autosomal recessive skeletal dysplasia caused by recessive mutations in the ACP5 gene. It is characterized by skeletal anomalies (short stature, platyspondyly, short broad ilia) and enchondromas in the long bones or pelvis. SPENCD has a heterogeneous clinical spectrum, including neurologic involvement or autoimmune manifestations, such as immune thrombocytopenic purpura, systemic lupus erythematosus, hemolytic anemia, and thyroiditis. [19]
-
Dysspondyloenchondromatosis is a nonhereditary skeletal dysplasia characterized by anisospondyly and multiple enchondromas in vertebrae and the metaphyseal and diaphyseal parts of long tubular bones, leading to kyphoscoliosis and lower limb asymmetry. [20]
Imaging modalities
Initially, radiography is the imaging modality of choice. If further characterization is necessary, magnetic resonance imaging (MRI) or computed tomography (CT) scanning is performed. If uncertainty remains, bone scanning may be helpful, but some lesions require biopsy.
Radiographic findings may not demonstrate or adequately characterize subtle calcifications to the extent that CT scans do. When calcifications are not present on either examination, MRI may be performed, which should reveal the classic appearance of noncalcified hyaline cartilage. Dystrophic calcifications in bone infarcts may be difficult to differentiate from chondroid matrix with ionizing radiation, and MRI may be helpful in these cases. When a clearly serpiginous rind of sclerosis encapsulates the lesion, the diagnosis of bone infarct is straightforward; however, when this finding is not present, MRI may be useful in differentiating the 2 entities. CT scans may also demonstrate the presence of calcification not depicted on radiographs. [21, 22, 23, 24, 25]
Chondrosarcoma—in particular, low-grade chondrosarcoma—may be indistinguishable from enchondroma. Certain imaging features may be helpful in distinguishing enchondroma from chondrosarcoma. However, even a lesion with no imaging features suggestive of malignancy and an imaging appearance compatible with an enchondroma should be resected when it is associated with pain. [24, 25]
When the lesion has calcifications, the primary differential diagnoses are bone infarct and chondrosarcoma. When the lesion is purely lytic, as shown on radiographs, the differential diagnosis consists of benign lytic lesions such as nonossifying fibroma, simple bone cyst, fibrous dysplasia, eosinophilic granuloma, and clear cell chondrosarcoma (which tends to involve the end of the bone—in particular, the proximal humerus).
One study concluded that for accurate diagnosis, conventional radiographic examination and, if necessary, contrast-enhanced MRI should be performed; in addition, histologic investigation was determined to be compulsory because of the risk of malignancy. [26]
Angiography is not used in the diagnosis for evaluation of solitary enchondroma. In Maffucci syndrome, angiography may play a secondary role in identifying the extent and origin of the vascular malformation.
Radiography
A classic pattern of calcifications, described as rings and arcs, is pathognomonic for enchondroma when it is seen in the hands. In the long bones, calcifications may be difficult to distinguish from the dystrophic calcifications seen in bone infarction. In addition, radiographs may not depict the rings and arcs of calcifications, particularly in the hands and feet.
(See the radiographic images of enchoncroma below.)
Enchondroma. Frontal radiograph of the right hand demonstrates a lytic expansile lesion in the fifth metacarpal bone, with thinning of the cortex that has a somewhat scalloped appearance. A pathologic fracture is noted, but no appreciable calcifications are seen in the lesion.
 Enchondroma. Detail of a lytic expansile lesion in the fifth metacarpal bone in the right hand (same patient as in previous image). There is thinning of the cortex with a somewhat scalloped appearance. A pathologic fracture is noted, but no appreciable calcifications are seen in the lesion.
Enchondroma. Frontal radiograph of the left hand demonstrates an expansile lytic lesion in the proximal phalanx of the fifth digit with a distinct zone of transition, thinning of the cortex, and a pathologic fracture. The lesion involves the diaphysis and approaches the end of the bone near the metacarpophalangeal joint. This finding is not uncommon in enchondromas of the small bones. Note the fuzzy calcifications in the matrix of the lesion.
Enchondroma. Detail of a lytic expansile lesion in the fifth metacarpal bone in the right hand (same patient as in previous image). There is thinning of the cortex with a somewhat scalloped appearance. A pathologic fracture is noted, but no appreciable calcifications are seen in the lesion.
Enchondroma. Frontal radiograph of the left hand demonstrates an expansile lytic lesion in the proximal phalanx of the fifth digit with a distinct zone of transition, thinning of the cortex, and a pathologic fracture. The lesion involves the diaphysis and approaches the end of the bone near the metacarpophalangeal joint. This finding is not uncommon in enchondromas of the small bones. Note the fuzzy calcifications in the matrix of the lesion.
 Enchondroma. Detail of an expansile lytic lesion in the proximal phalanx of the fifth digit with a distinct zone of transition, thinning of the cortex, and a pathologic fracture (same patient as in previous image).
Enchondroma. Detail of an expansile lytic lesion in the proximal phalanx of the fifth digit with a distinct zone of transition, thinning of the cortex, and a pathologic fracture (same patient as in previous image).
 Enchondroma. Radiograph of the right femur demonstrates a calcified intramedullary lesion in the distal shaft.
Enchondroma. Radiograph of the right femur demonstrates a calcified intramedullary lesion in the distal shaft.
 Enchondroma. Radiograph of the right femur demonstrates a calcified intramedullary lesion in the distal shaft (same patient as in previous image).
Enchondroma. Radiograph of the right femur demonstrates a calcified intramedullary lesion in the distal shaft (same patient as in previous image).
 Enchondroma. Frontal radiograph of the right thigh demonstrates coarse calcifications in the distal femur.
Enchondroma. 62-year-old woman with enchondroma involving the proximal end of the proximal phalanx of her middle finger. The lesion has a lobular morphology and punctate calcifications. Because of pain, the lesion was curetted and packed with morselized allograft bone.
Enchondroma. Frontal radiograph of the right thigh demonstrates coarse calcifications in the distal femur.
Enchondroma. 62-year-old woman with enchondroma involving the proximal end of the proximal phalanx of her middle finger. The lesion has a lobular morphology and punctate calcifications. Because of pain, the lesion was curetted and packed with morselized allograft bone.
On radiographs, the degree of confidence in the diagnosis of an enchondroma depends on the clinical situation and the appearance of the lesion. In the presence of pain, almost regardless of appearance, further investigation is warranted. Lesions that are predominantly lucent or are nonuniformly mineralized often require further investigation as well.
In most cases, enchondroma and a low-grade chondrosarcoma cannot be reliably distinguished on the basis of radiographic findings alone. A calcified enchondroma can also mimic the appearance of a calcified marrow infarct. However, in most cases, chondrosarcoma has certain imaging features that are indicative of its aggressive behavior. Cortical breakthrough, soft-tissue mass, and deep endosteal scalloping of the cortex are 3 features that are described more frequently in chondrosarcoma. Deep endosteal scalloping with consequent pathologic fracture in the small bones of the hands and feet does not imply malignancy, however, because enchondromas are more cellular and expansile in these locations.
In Ollier disease, enchondromas often appear to be larger than they do in other conditions. Because enchondromas occur in young patients and can be large, growth of the affected limbs may be adversely affected, and pathologic fractures may occur. Enchondromatosis can occasionally have the appearance of linear lucencies, in which the chondrocytes appear to line up in a vertical orientation along the length of the bone.
Ollier disease must be differentiated from hereditary multiple exostosis. The osteochondromas seen in hereditary multiple exostosis are located at the bone surface, whereas enchondromas are located in the center of bones
In Maffucci syndrome, associated soft-tissue hemangiomas are seen. Soft-tissue hemangiomas typically have numerous rounded calcifications with central lucencies, which are consistent with phleboliths on plain radiographs. T2-weighted MRIs of these lesions show high-signal-intensity tubular structures, which are consistent with slow flow in vascular channels.
Metachondromatosis has associated osteochondromas, which differ from conventional osteochondromas in that they point toward rather than away from the joint.
Malignant transformation is a major complication of enchondromatosis in approximately 35% of cases. [9, 3] Signs of malignancy include cortical erosion, extension of the tumor into soft tissues, and irregularity or indistinctness of the surface of the tumor. Compared to chondrosarcomas, which show poor demarcation, enchondromas tend to be well circumscribed. Enchondromas normally show a uniform pattern of mineralization. The presence of unmineralized parts in the lesion should raise the suspicion for malignancy. [8]
Computed Tomography
The features of enchondroma on CT scan are the same as those depicted on radiographs (see the image below). Enchondromas are endosteal lesions with a lobular morphology and variable mineralization. Often, the mineralization is in the form of rings and arcs, which correspond to calcification around lobules of cartilage. A pathologic fracture may be present. Sometimes, endosteal scalloping is present, but this feature may be suggestive of degeneration of the enchondroma to a chondrosarcoma. Enchondromas should not penetrate the cortex or extend into the soft tissues. If a densely mineralized or uniformly mineralized lesion has a region that is lucent, degeneration of the enchondroma to a chondrosarcoma is suggested, and biopsy is likely necessary.
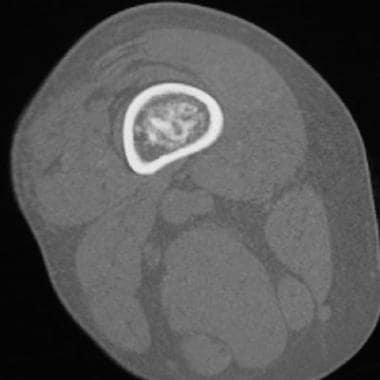 Enchondroma. Axial computed tomography image demonstrates a fluffy calcific matrix within the medullary canal of the distal femur. The surrounding cortex is intact.
Enchondroma. Axial computed tomography image demonstrates a fluffy calcific matrix within the medullary canal of the distal femur. The surrounding cortex is intact.
As with radiographs, the degree of confidence in the diagnosis of an enchondroma with CT scanning depends on the clinical situation and the appearance of the lesion. The absence of pain, uniform or dense mineralization, and endosteal scalloping or cortical penetration are all indications of an enchondroma. However, if the patient lacks any of these features, further investigation may be necessary. Distinguishing an enchondroma from a low-grade chondrosarcoma is often problematic; sometimes, the diagnosis cannot be resolved without a biopsy. Because cartilage lesions are often not uniform at histologic examination, the entire lesion may need to be removed at biopsy.
Magnetic Resonance Imaging
MRI findings may be useful in distinguishing enchondromas in the long bones from bone infarcts (see the images below). Typically, bone infarcts are encapsulated by a serpiginous rind of decreased signal intensity on T1- and T2-weighted images. Frequently, this rind is subtended by a high-signal-intensity line. This finding has been called the double-line sign, and it consists of a high-signal-intensity rind circumscribed by, and immediately adjacent to, a low-signal-intensity rind on T2-weighted images.
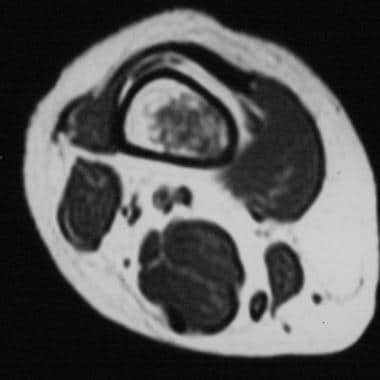 Enchondroma. Axial T1-weighted magnetic resonance imaging study shows an intramedullary lesion with low signal intensity and lobular morphology in the distal femur. The endosteal aspect of the cortex is not affected.
Enchondroma. Axial T1-weighted magnetic resonance imaging study shows an intramedullary lesion with low signal intensity and lobular morphology in the distal femur. The endosteal aspect of the cortex is not affected.
 Enchondroma. Coronal T1-weighted magnetic resonance imaging study demonstrates predominantly decreased signal intensity within a lesion in the distal femur (same patient as in previous image). The lesion has a lobular morphology. No endosteal scalloping is noted.
Enchondroma. Coronal T1-weighted magnetic resonance imaging study demonstrates predominantly decreased signal intensity within a lesion in the distal femur (same patient as in previous image). The lesion has a lobular morphology. No endosteal scalloping is noted.
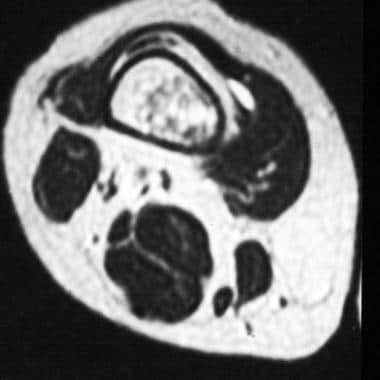 Enchondroma. Axial T2-weighted magnetic resonance imaging study shows regions of high signal intensity in the lesion (same patient as in previous image). No surrounding edema is noted.
Enchondroma. Axial T2-weighted magnetic resonance imaging study shows regions of high signal intensity in the lesion (same patient as in previous image). No surrounding edema is noted.
 Enchondroma. Coronal T2-weighted magnetic resonance imaging study demonstrates small lobulated foci of increased signal intensity separated by a background mesh of decreased signal intensity (same patient as in previous image). The adjacent cortex is intact.
Enchondroma. Coronal T2-weighted magnetic resonance imaging study demonstrates small lobulated foci of increased signal intensity separated by a background mesh of decreased signal intensity (same patient as in previous image). The adjacent cortex is intact.
Conversely, enchondromas tend to have lobulated borders with a cluster of numerous tiny locules of high-signal-intensity foci on T2-weighted images that appear to coalesce with one another and reflect the high fluid content of hyaline cartilage. On T1-weighted images, enchondromas demonstrate low-to-intermediate signal intensity.
When a calcific chondroid matrix is observed on radiographs, decreased signal intensity is expected to occur in those areas on images obtained with all MRI pulse sequences. These areas may become particularly pronounced on gradient-echo images.
When combined with a typical appearance on radiographs and an absence of pain, the diagnosis of enchondroma with MRI findings can be made with a high degree of confidence. Enchondromas may also be incidental findings at routine examination, such as MRI of the knee. If the lesions have a typical appearance, a confident diagnosis may be made; however, the acquisition of correlative radiographic findings is often prudent.
Occasionally, enchondromas can be difficult to distinguish from other intraosseous benign and malignant lesions on the basis of MRI findings alone. Correlation with other results, particularly radiographic results, may help. The presence of bone pain always warrants further investigation.
Nuclear Imaging
With technetium-99m (99mTc) radionuclide bone scanning, findings are typically negative in uncomplicated enchondromas, but the presence of pathologic fracture results in intense activity at the fracture site. In patients with multiple enchondromas or patients in whom an enchondroma is actively calcifying, radionuclide bone scans may show increased activity, but the activity is typically less intense than that of intramedullary chondrosarcomas.
Positron emission tomography (PET) using 18-fluorodeoxyglucose (18-FDG) has been applied increasingly to the evaluation of tumors. Using PET to evaluate enchondromas—particularly to distinguish benign enchondromas from low-grade chondrosarcomas—has been reported in small series.
Feldman et al recommended 18-FDG PET as an adjunct for the evaluation of aggressive cartilage lesions. In their study, 11 enchondromas were studied by PET with 18-FDG; the maximum standard uptake values (SUVs) ranged from 0.8 to 1.8. The authors established a maximum SUV of 2.0 as the cutoff between benign and malignant; 10 of the 11 chondrosarcomas in their study had maximum SUVs, ranging from 2.4 to 12.4. One lesion was considered a borderline chondrosarcoma, having a maximum SUV of 1.4, which was below the value of 2.0 that they used as the cutoff between benign and malignant. [27]
Radionuclide bone scanning is one method used to assess lesions depicted on radiographs or MRIs that are presumed to be enchondromas. If the bone scan results are negative, the possibility of a malignancy (eg, chondrosarcoma) is extremely remote. If the scan results are positive, biopsy is typically necessary. Radionuclide bone scan findings are not reliable in differentiating enchondroma from calcified marrow infarct.
Radionuclide bone scan findings are nonspecific; therefore, one cannot reliably diagnose a focal bone lesion on the basis of these findings alone. However, the physiologic information provided by a bone scan, when combined with information from other imaging modalities, can be helpful.
-
Enchondroma. Frontal radiograph of the right hand demonstrates a lytic expansile lesion in the fifth metacarpal bone, with thinning of the cortex that has a somewhat scalloped appearance. A pathologic fracture is noted, but no appreciable calcifications are seen in the lesion.
-
Enchondroma. Detail of a lytic expansile lesion in the fifth metacarpal bone in the right hand (same patient as in previous image). There is thinning of the cortex with a somewhat scalloped appearance. A pathologic fracture is noted, but no appreciable calcifications are seen in the lesion.
-
Enchondroma. Frontal radiograph of the left hand demonstrates an expansile lytic lesion in the proximal phalanx of the fifth digit with a distinct zone of transition, thinning of the cortex, and a pathologic fracture. The lesion involves the diaphysis and approaches the end of the bone near the metacarpophalangeal joint. This finding is not uncommon in enchondromas of the small bones. Note the fuzzy calcifications in the matrix of the lesion.
-
Enchondroma. Detail of an expansile lytic lesion in the proximal phalanx of the fifth digit with a distinct zone of transition, thinning of the cortex, and a pathologic fracture (same patient as in previous image).
-
Enchondroma. Radiograph of the right femur demonstrates a calcified intramedullary lesion in the distal shaft.
-
Enchondroma. Radiograph of the right femur demonstrates a calcified intramedullary lesion in the distal shaft (same patient as in previous image).
-
Enchondroma. Axial computed tomography image demonstrates a fluffy calcific matrix within the medullary canal of the distal femur. The surrounding cortex is intact.
-
Enchondroma. Frontal radiograph of the right thigh demonstrates coarse calcifications in the distal femur.
-
Enchondroma. Axial T1-weighted magnetic resonance imaging study shows an intramedullary lesion with low signal intensity and lobular morphology in the distal femur. The endosteal aspect of the cortex is not affected.
-
Enchondroma. Coronal T1-weighted magnetic resonance imaging study demonstrates predominantly decreased signal intensity within a lesion in the distal femur (same patient as in previous image). The lesion has a lobular morphology. No endosteal scalloping is noted.
-
Enchondroma. Axial T2-weighted magnetic resonance imaging study shows regions of high signal intensity in the lesion (same patient as in previous image). No surrounding edema is noted.
-
Enchondroma. Coronal T2-weighted magnetic resonance imaging study demonstrates small lobulated foci of increased signal intensity separated by a background mesh of decreased signal intensity (same patient as in previous image). The adjacent cortex is intact.
-
Enchondroma. 62-year-old woman with enchondroma involving the proximal end of the proximal phalanx of her middle finger. The lesion has a lobular morphology and punctate calcifications. Because of pain, the lesion was curetted and packed with morselized allograft bone.



