Practice Essentials
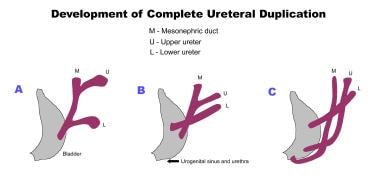
Duplicated collecting systems (also known as duplex collecting systems, duplex kidney, and duplicated ureters) can be defined as renal units containing 2 pyelocaliceal systems that are associated with a single ureter or with double ureters. Duplication occurs when 2 separate ureteric buds arise from a single Wolffian duct. Based on the degree of fusion, it can present as bifid renal pelvis, partial ureteric duplication (Y-shaped ureter), incomplete ureteric duplication with ureters joining near or in bladder wall (V-shaped ureter), and complete ureteric duplication with separate ureteric orifice. [1, 2, 3, 4]
A determination must be made as to whether the duplex kidneys are normal or pathologic. In normal duplex kidneys, the renal pelvises are of normal width, and the upper and lower poles are about the same size. Also, in normal duplex kidneys, the ureters are not dilated, and the upper and lower poles are not altered cystically. In pathologic duplex kidneys, one or both renal pelvises are dilated, and one or both ureters may be dilated. If a megaureter is present, a ureterocele must be ruled out, and a pathologic duplex kidney must always be assumed if one pole of the kidney is hypoplastic. [2]
(See the images of duplicated collecting system below.)
 Excretory urography in an adult patient with bilateral complete ureteral duplication.
Excretory urography in an adult patient with bilateral complete ureteral duplication.
 Ultrasonographic scan of the bladder of a child with bilateral ureteral duplication demonstrates bilateral ureteroceles.
Ultrasonographic scan of the bladder of a child with bilateral ureteral duplication demonstrates bilateral ureteroceles.
Duplex collecting systems can be unilateral or bilateral and can be associated with a variety of congenital genitourinary tract abnormalities. Most patients are asymptomatic, with genitourinary tract abnormalities being detected incidentally on imaging studies performed for other reasons. Symptomatic patients usually have complete ureteric duplication in which the ureters are prone to developing obstruction, reflux, and infection. [5] Ureteropelvic obstruction is more common when a duplex kidney exists and can be inherited in an autosomal dominant pattern. [6]
Duplex collecting systems are the most common variant of renal anatomy. It has a female preponderance and an estimated prevalence ranging between 0.3% and 6% of the population. [7] Diagnosis is important for operative planning and long-term follow up. [8]
When a single ureteral bud bifurcates before the ampulla bifurcates, a duplex kidney with a bifid renal pelvis or bifid ureter results. [9] If 2 ureteral buds arise from the Wolffian duct, a duplex kidney with complete ureteral duplication ensues. The Committee on Terminology, Nomenclature, and Classification of the Section on Urology of the American Academy of Pediatrics suggested the use of the following terms in reference to duplex collecting systems [10] :
-
Duplex kidney - The duplex kidney has a single renal parenchyma that is drained by 2 pyelocaliceal systems.
-
Upper or lower pole - The poles represent one component of a duplex kidney.
-
Duplex system - The kidney has 2 pyelocaliceal systems and is associated with a single ureter or with a bifid ureter (a partial duplication) or, in the case of a complete duplication, with 2 ureters (double ureters) that drain separately into the urinary bladder.
-
Bifid system - Two pyelocaliceal systems join at the ureteropelvic junction (bifid pelvis), or 2 ureters join before draining into the urinary bladder (bifid ureters).
-
Double ureters - Two ureters open separately into the renal pelvis superiorly and drain separately into the bladder or genital tract.
-
Upper and lower pole ureters - Upper and lower pole ureters drain a duplex kidney's upper and lower poles, respectively.
Imaging modalities
A patient's duplex kidney is almost always more elongated than a nonduplex kidney. The kidney may be enlarged when hydronephrotic and can be associated with rotational anomalies. Excretory urographic findings are almost always diagnostic. Difficulty may arise when function is poor or absent in one of the moieties. [11]
Magnetic resonance (MR) urography may be used as the primary diagnostic method for assessing a duplex ectopic ureter, as well as the complications associated with duplex kidneys. [12, 13] Spatial resolution is a limiting factor. The availability of MRI is limited, the procedure is expensive, and it requires the sedation of patients who have claustrophobia. However, MR urography is an extremely useful technique in patients who have the probability of an adverse reaction to radiopaque contrast media. [12]
If vesico-ureteral reflux exists, the presence of an ectopic ureter in a nonfunctioning moiety can best be demonstrated by using a voiding cystourethrogram. [14, 15]
Antegrade pyelography is useful in patients with hydronephrosis, to demonstrate the presence of a second ureter, and to determine the level of ureteric termination.
Computed tomography (CT) scanning with contrast is superior to ultrasonography and excretory urography in diagnosing the nubbin. [16] On excretory urography, an obstructed, nonfunctioning upper or lower pole may mimic a renal mass. On a CT scan, a large column of Bertin can mimic a duplex collecting system. However, CT scanning is valuable in the evaluation of an intravesical ureterocele, either orthotopic or ectopic. [17, 18]
Ultrasonography is a noninvasive and extremely useful examination, particularly in children. The ultrasonographic appearance of a duplex kidney is specific but not sensitive. [19] Ultrasonographic findings provide excellent anatomic information but do not necessarily differentiate a bifid renal pelvis from a bifid ureter or from 2 complete ureters.
Scintigraphy is useful in the assessment of relative renal function and in the detection of renal scars. [20] Scintigraphy can reveal differential functioning. However, if the functioning is markedly depressed, imaging is limited. [21]
Plain radiography makes no major contribution to diagnosis. Plain radiographs can demonstrate a renal mass, which is a nonspecific finding. However, because a patient's duplex kidney is almost always longer than a nonduplex kidney, a renal mass may be apparent on a plain radiograph. Hydronephrotic upper or lower pole moiety in a duplex collecting system also can be observed as a renal mass.
Arteriography is an invasive procedure and is no longer used to diagnose duplex collecting systems. However, it may occasionally be useful in planning nephron-sparing surgery. [22]
Radiography
In almost all patients, the duplex kidney is longer than the opposite, nonduplex kidney. In a duplex collecting system, hydronephrotic upper or lower pole moiety can be observed as a renal mass.
Plain radiographic appearances in a duplex kidney are nonspecific. Urographic findings in a duplex system are almost always diagnostic in patients. Difficulty may arise when one of the moieties is poorly opacified or is not opacified at all. Reflux may occur into the ureter at only 1 pole, into both ureters in the same kidney, or, if the duplication is bilateral, into all 4 ureters. An absence of reflux does not exclude ureteral duplication.
On plain radiographs, depiction of a normal renal outline does not exclude a duplex collecting system. When a duplex kidney has a lower pole nubbin, the resulting image may give the impression that a lower pole mass is present. The upper pole moiety can simulate a renal/adrenal mass. Other causes of lower pole nubbins include parenchymal scarring, infection, and congenital anomalies. A second, nonfunctioning collecting system may not be depicted, leading to an erroneous determination that only a single collecting system exists.
(See the images below of duplicated collecting system on excretory urography.)
 Excretory urography in a woman shows complete ureteral duplication on the right. The upper moiety ureter empties below and medial to the ureter of the lower moiety. Note the duplex collecting system on the left.
Excretory urography in a woman shows complete ureteral duplication on the right. The upper moiety ureter empties below and medial to the ureter of the lower moiety. Note the duplex collecting system on the left.
 Excretory urography in a man shows a blind-ending ureteric bud on the left, arising from the bladder.
Excretory urography in an adult patient with bilateral complete ureteral duplication.
Excretory urography in a man shows a blind-ending ureteric bud on the left, arising from the bladder.
Excretory urography in an adult patient with bilateral complete ureteral duplication.
 Excretory urography in a patient with a duplex right kidney shows hydronephrosis of the lower moiety.
Excretory urography in a patient with a duplex right kidney shows hydronephrosis of the lower moiety.
 Excretory urography in a man shows drooping of the right-sided calyces. No obvious mass is evident in the region of the right upper pole.
Excretory urography in a man shows drooping of the right-sided calyces. No obvious mass is evident in the region of the right upper pole.
Excretory urography shows the following:
-
A patient's duplex kidney is usually longer than a nonduplex kidney.
-
The parenchymal thickness of one of the poles of the duplex kidney is less than that of the other pole.
-
The calyces are asymmetric.
-
An ectopic, upper pole ureteric insertion can produce a nonopacified segment. This mass effect results in the "drooping lily" sign with the depression of the lower pole pelvicaliceal system.
-
If the lower pole of the duplex kidney is functioning poorly or not at all, the lower pole collecting system may not opacify, and no discernible parenchyma will surround it (nubbin sign). The kidney's appearance may consequently resemble that of a nonduplex kidney with a lower polar mass or renal infarct.
-
A reduction in the number of calyces, the depiction of a portion of the collecting system, and the presence of a straight inferior border help differentiate a duplex collecting system from a renal mass.
-
Anomalies of the ureter, such as partial or complete ureteral duplication, may be demonstrated.
The intravesical ectopic ureter of a nonvisualized moiety is better demonstrated using voiding cystourethrogram. In patients with hydronephrosis, antegrade pyelography is useful for demonstrating the presence of a second ureter and for determining the level of termination.
Computed Tomography
Because the intervening renal parenchyma in a duplex kidney lacks a collecting system and major vessels, it is described as having a "faceless kidney" appearance. CT scanning can help determine if an obstruction exists and can aid in assessing the renal parenchyma. CT scanning can also help determine if the insertion of the duplex ureter is intravesical or extravesical. In addition, it can demonstrate the collecting system in the nubbin or the mass effect of tissue at the pole. [16]
Using 16-multidetector computed tomography (16-MDCT) scanning on 126 consecutive potential kidney donors, Raman and colleagues described and quantified renal anatomic variants and looked at the frequency of various findings associated with the renal parenchyma and with the collecting system. [23] CT scan studies were produced prior to contrast injection, as well as after the intravenous power injection of nonionic contrast during the arterial, nephrographic, and excretory phases. The authors focused on the relevance of their results to the preoperative evaluation of potential laparoscopic renal donors. Major and minor arterial and venous variants were confidently identified. Moreover, in 30% of the scanned kidneys, other parenchymal and urothelial abnormalities (for the most part, cysts and calyceal calcifications) were found. Additional relevant findings included focal infarcts, cortical scars, atrophic scarred kidney, and bilateral papillary necrosis. Among the identified urothelial variants were bilateral simple ureteroceles and a right-sided complete duplex collecting system. The authors concluded that MDCT has a potential use in the evaluation of possible laparoscopic renal donors. [23]
CT scanning is superior to ultrasonography and excretory urography in diagnosing the lower pole nubbin. In addition, the modality is helpful when function is poor or absent. Diagnosing a lower pole nubbin is not always possible using CT scan findings, and an erroneous diagnosis may occur. Large cloisons (hypertrophied columns of Bertin) can simulate duplex kidneys on CT scans. [24]
Magnetic Resonance Imaging
MR urography may be used as a primary diagnostic method in assessing a duplex ectopic ureter and complications associated with duplex kidneys. The role of MR in imaging renal duplication anomalies is not yet clearly defined. MR urography can provide information similar to that of excretory urography when renal function is poor or absent. An ectopic ureter extending from a poorly functioning moiety of a duplex kidney, invisible on other imaging, may be observed with MR urography. [12, 13]
Ectopically inserted vaginal ureters generally present with continuous dribbling of urine. Using conventional imaging, Jain describes a case of a young girl with a severe stenosis of the ectopically located ureteric orifice in whom the vaginal insertion of the ectopic ureter could not be seen. However, the collecting system, from the kidney to the point of ureteric insertion, appeared on an MR urogram. [25]
According to Engin and associates, ultrasonography and MR urography depicted the collecting system from the kidney to the distal ureteral insertion in an adult male whose duplex ectopic ureter inserted into the prostatic urethra. [26]
Ultrasonography
The duplex kidney appears as 2 central echo complexes with intervening renal parenchyma. Hydronephrosis at one pole is suggestive of a duplex kidney. [19] Although hydronephrosis can occur at either pole, it is more common in the upper one. Occasionally, 2 distinct collecting systems and ureters can be observed on ultrasonographic images. (See the image below.)
Ultrasonographic scan of the bladder of a child with bilateral ureteral duplication demonstrates bilateral ureteroceles.
The ultrasonographic appearance of a duplex kidney is specific but not sensitive. Differentiating an atrophied lower pole moiety of a duplex kidney (nubbin) from other renal masses is difficult. [16] The nubbin of tissue from the atrophied lower pole of a duplex kidney cannot be confidently differentiated from other masses.
Nabavizadeh et al studied the use of 3-dimensional virtual sonographic cystoscopy (VSC) to characterize ureterocele in duplex collecting systems in 16 children (mean age, 5.1 yr). VSC was well tolerated in all cases, and in 14 cases, VSC had a high accuracy for ureterocele features (93%). Image quality was suboptimal in 2 of 16 patients. [27]
Nuclear Imaging
Duplex kidneys appear as 2 separate collecting systems on the same side of the body. Scintigraphy may demonstrate reflux up the ureter in a nonfunctioning duplex kidney with ureteral duplication.
The presence of a duplex kidney and ureteral duplication, suggested by findings from excretory urographic or ultrasonographic images, can be confirmed with scintigraphy. The use of dimethylsuccinic acid (DMSA) scanning to assess parenchymal function in a duplex kidney is of great value in the management of duplex kidney. [20]
Reflux of activity from the bladder can mimic cortical function in a nonfunctioning moiety. When DMSA scans are to be obtained in a pediatric patient with possible reflux, it is recommended that catheterization be performed prior to the study and that images be produced before the appearance of DMSA in the collecting system.
Smakal and colleagues proposed using DMSA renal scintigraphy to predict irreversible lesions in the upper pole (UP) of duplicated collecting systems. In a study of 23 patients with ureteroceles and 28 patients with ectopic ureters, histologic lesions were irreversible in 20 of 23 patients (87%) with ureteroceles and in 14 of 28 patients (50%) with ectopic ureters. Tc-99m DMSA scintigraphy was used to assess function of the affected UP. Differential function of the UP (the percentage of overall function measured by renal uptake) was determined by using the high-resolution images. The model was able to predict irreversible lesions if an upper pole differential function was 3% or less in patients with ureteroceles and 2% or less in the presence of ectopic ureters. [28]
-
Line diagram shows development of complete ureteral duplication.
-
Excretory urography in a woman shows complete ureteral duplication on the right. The upper moiety ureter empties below and medial to the ureter of the lower moiety. Note the duplex collecting system on the left.
-
Excretory urography in a man shows a blind-ending ureteric bud on the left, arising from the bladder.
-
Excretory urography in an adult patient with bilateral complete ureteral duplication.
-
Excretory urography in a patient with a duplex right kidney shows hydronephrosis of the lower moiety.
-
Excretory urography in a man shows drooping of the right-sided calyces. No obvious mass is evident in the region of the right upper pole.
-
Ultrasonographic scan of the bladder of a child with bilateral ureteral duplication demonstrates bilateral ureteroceles.








