Practice Essentials
In many patients with thoracic trauma injury, urgent exploratory thoracotomy or laparotomy may take precedence over imaging, whereas in others, diagnosis and treatment are frequently combined with tube thoracostomy or pericardiocentesis. Imaging studies are an essential part of thoracic trauma care once the patient is stabilized. [1, 2, 3] Imaging has little if any role in the initial treatment of a critically ill and hemodynamically unstable patient.
The first priority in cases of thoracic trauma is the provision of effective therapeutic measures to minimize trauma-related deaths and morbidity. Imaging is not indicated until the airway, breathing, and circulation (ABC) have been secured and stabilized. The initial approach to chest trauma is clinical evaluation, which starts with a thorough examination of the chest after the airway is controlled. Severe internal injury may be present without external tenderness. [4]
A chest radiograph is obtained for every patient who has significant trauma. The primary goals of chest radiography are to confirm support device placement and to identify immediately life-threatening findings, such as tension pneumothorax. [5] The diagnosis is generally obvious with standard chest radiography or CT, but more subtle signs require careful analysis of CT images and examination with MRI in some situations. Previous comparisons have indicated that a majority of thoracic injuries found on CT (in particular, multi-detector CT) may be missed on chest radiography. Multi-detector CT, therefore, has been established as a critical portion of the initial evaluation of patients in blunt thoracic trauma. [5]
Prolonged observation in a monitored setting is usually not required for patients with suspected myocardial contusion. Patients with a normal electrocardiogram (ECG) and a normal echocardiogram are usually discharged home after 12 hours of monitoring. Cardiac complications are rare in cases of cardiac contusion, particularly in the young.
Echocardiography is useful for detecting wall-motion abnormalities and pericardial effusions. In combination with abnormal creatine kinase–MB levels, this may be predictive of complications. Radionuclide angiographic results also may be predictive of complication. Thallium scanning may depict areas of decreased perfusion but are not useful in differentiating an acute lesion from a preexisting lesion.
Ultrasonography, CT, and magnetic resonance imaging (MRI) may all demonstrate pericardial effusions and hemopericardium, but they are rarely indicated in a patient with acute traumatic tamponade. The roles of CT, MRI, and transesophageal ultrasonography in the evaluation of aortic injuries have not been clearly defined, although multisection CT scanning is increasingly used for diagnosis.
Radiography
Chest radiography (see the images below) is indicated in virtually every trauma patient; a series of radiographs are generally obtained to assess the progress and complications of the trauma. They are also used to look for malpositioned lines and tubes; in the stress and confusion of an emergency department, inadequate and inappropriate placement of lines and tubes is common. [6]
 Radiograph of the left shoulder of a 36-year-old man after undergoing a direct blow to the upper thorax shows a fracture of the first rib. The most common injury caused by blunt trauma is a rib fracture, which may be easily missed with suboptimal technique. Overpenetration and a decrease in the kilovolt-peak improve skeletal visualization, although at the expense of lung detail. If available, digital imaging improves visualization, and images may be displayed on a workstation and manipulated. Fractures of the first and second ribs are rare but are often overlooked; they are most often associated with serious vascular and tracheobronchial or spinal injury.
Radiograph of the left shoulder of a 36-year-old man after undergoing a direct blow to the upper thorax shows a fracture of the first rib. The most common injury caused by blunt trauma is a rib fracture, which may be easily missed with suboptimal technique. Overpenetration and a decrease in the kilovolt-peak improve skeletal visualization, although at the expense of lung detail. If available, digital imaging improves visualization, and images may be displayed on a workstation and manipulated. Fractures of the first and second ribs are rare but are often overlooked; they are most often associated with serious vascular and tracheobronchial or spinal injury.
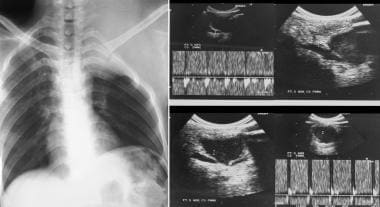 Chest radiograph in a child with a shrapnel injury after the shrapnel was removed surgically. Six months later, the child presented with increasing left supraclavicular soft tissue swelling. Left, a chest radiograph shows a soft tissue mass associated with destruction of the first left rib. Right, 2-dimensional and Doppler sonograms show a pseudoaneurysm of the left subclavian artery.
Chest radiograph in a child with a shrapnel injury after the shrapnel was removed surgically. Six months later, the child presented with increasing left supraclavicular soft tissue swelling. Left, a chest radiograph shows a soft tissue mass associated with destruction of the first left rib. Right, 2-dimensional and Doppler sonograms show a pseudoaneurysm of the left subclavian artery.

A chest radiograph is usually performed initially in the acute setting. Findings on a chest radiograph include pneumothorax (which is difficult to see on a supine image), pneumomediastinum, airspace shadowing (resulting from pulmonary contusion), and pleural hematoma. CT is better for assessing most of these lesions.
Repeat chest radiographs are obtained after any invasive intervention, such as intubation or placement of the central venous pressure catheter or chest tube. Iatrogenic lung trauma may occur after lung biopsy, thoracentesis, cauterization, and other procedures. Mechanical ventilation predisposes the patient to barotrauma and pneumothorax. Lung injuries may result from the inhalation of toxic and inert substances, as well as in association with blast or radiation.
Portable AP radiographs have several limitations when the images are obtained in an emergency situation with the patient in a supine position. Expiratory artifacts and the magnification effect of a short beam distance may make the mediastinum appear widened. Injuries involving the diaphragm are often missed, and preexisting diaphragmatic eventrations or an elevated hemidiaphragm may mimic diaphragmatic injuries.
Radiographic findings associated with aortic transection are nonspecific. They may be seen in a variety of other mediastinal or chest wall injuries, including nonaortic vascular injuries, fractures of the sternum, vertebral fractures, and esophageal rupture. Predictions regarding the presence of mediastinal hemorrhage on supine portable chest radiographs in the setting of trauma are inaccurate. Plain imaging findings of thoracic spinal fractures are often subtle and are difficult to identify because of the limited quality of many trauma radiographs.
Computed tomography
Advancements in CT imaging have changed the management of blunt lung trauma and have permitted the detection of blood in bronchi and interstitial air or blood with greater accuracy. [7, 8] Many centers now screen patients with chest trauma for aortic injuries by using contrast-enhanced CT. CT scans (see the images below) also demonstrate injuries to the lung, pleura, mediastinum, and chest wall better than plain radiographs do. Many serious thoracic injuries may be overlooked on initial chest radiographs; these include tracheobronchial tears, diaphragmatic rupture, esophageal tears, thoracic spine injuries, chest wall and seat-belt injuries, lung contusion, cardiac injuries, pneumothorax, hemothorax, and chest tube complications. [9, 10, 11, 12, 4]
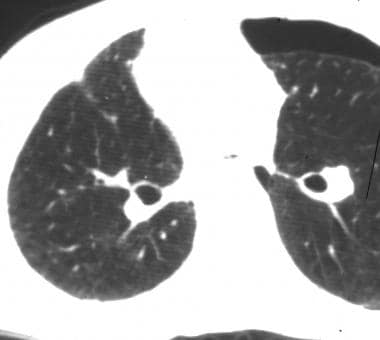 Transaxial, nonenhanced computed tomography scan shows a pneumothorax in a patient in whom the chest radiograph was normal.
Transaxial, nonenhanced computed tomography scan shows a pneumothorax in a patient in whom the chest radiograph was normal.
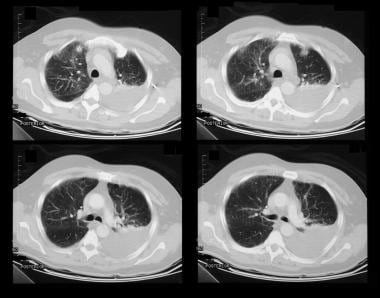
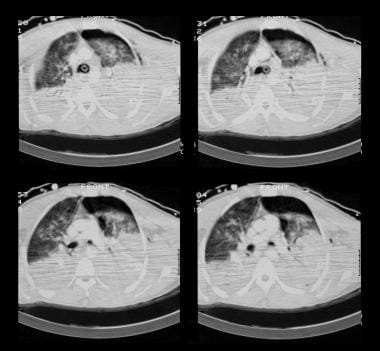 Contrast-enhanced axial computed tomography scan through the thorax of a 20-year-old man after a motorbike accident shows massive, bilateral pulmonary contusions; pneumopericardium; and hemopneumothorax.
Contrast-enhanced axial computed tomography scan through the thorax of a 20-year-old man after a motorbike accident shows massive, bilateral pulmonary contusions; pneumopericardium; and hemopneumothorax.
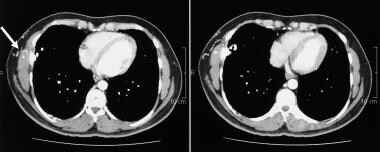
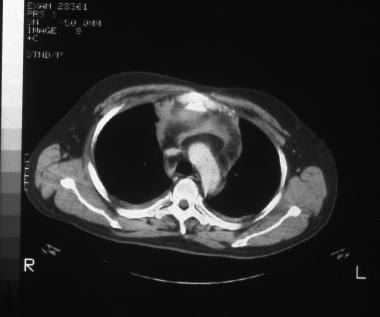 Contrast-enhanced computed tomography scan through the mediastinum shows a pneumopericardium in a 26-year-old man involved in a motorbike accident.
Contrast-enhanced computed tomography scan through the mediastinum shows a pneumopericardium in a 26-year-old man involved in a motorbike accident.
CT images demonstrate fractures of the vertebral bodies with great accuracy and readily show the relationship of fractured fragments and displaced disk material to the cord. Sagittal and coronal reconstructions may provide further exquisite detail.
Multidetector CT (MDCT) using dual-phase scanning protocol is the primary imaging method for the evaluation of the entire chest and abdomen in patients with high-energy blunt trauma and is the primary tool to evaluate patients with suspected acute vascular injuries. Acute vascular injures encompass a wide spectrum of findings—including spasm, intimal tears, intramural hematoma, pseudoaneurysms, arteriovenous fistula (AVF), hemorrhage, and vessel transection and avulsion—and MDCT provides optimal depiction and characterization of all these vascular injuries. [13]
Because of a dramatic reduction in motion and beam-hardening artifacts and significant improvement of spatial resolution, especially along the z-axis, helical and multisection CT scanning allows better demonstration of the most subtle signs of thoracic trauma, such as a focal indentation of the liver or a right-sided collar sign. In addition, helical and multisection CT is a useful tool in the evaluation of patients with multiple traumatic injuries.
Patients with severe trauma are often difficult to scan with CT because of resuscitative equipment. CT is an excellent modality, but patients are required to receive contrast agents and be transported from the protected resuscitation area to the radiology suite. Therefore, CT scanning is difficult to perform in hemodynamically unstable patients.
Magnetic resonance imaging
MRI has many advantages over CT in the evaluation of patients with suspected dorsal spine injuries. It provides excellent detail of intervertebral disks, spinal ligaments, paravertebral soft tissues, and other spinal contents (eg, cord and nerve roots). MRI is particularly useful in evaluating patients with spinal cord injury without radiographic abnormality (SCIWORA) syndrome. MRIs show cord edema or hematoma, which may account for any neurologic deficit the patient may have. MRI is an important diagnostic and prognostic tool in patients with thoracolumbar compression–type fractures.
MRI with breath-hold acquisition permits good visualization of diaphragmatic abnormalities, but this technique cannot be performed in emergency situations. MRI offers a major advantage in exploring the cord, disks, and ligaments and in looking for a hematoma. Nevertheless, the indication is carefully weighed in patients with multiple trauma because of monitoring difficulties during the examination, which may be long.
MRI is expensive and is not universally available in emergency departments. Also, MRI often cannot be used in patients with ferromagnetic foreign bodies or some types of prosthetic cardiac valves, as well as in those with claustrophobia. MRI should be performed only in patients when MRI-compatible resuscitation equipment is readily available.
Echocardiography, ultrasonography, and angiography
Conventional echocardiography has long been used to image the heart, the pericardial space, and the ascending aorta. Transesophageal ultrasonography is an excellent modality for visualizing the aortic arch and the descending aorta and may be used at the patient's bedside. Because ultrasonography is unique in being portable, rapid, and noninvasive, it is particularly suited to the trauma setting and offers immediate feedback that may be incorporated into the management plan for the patient. Ultrasonography is operator dependent and may cause some aortic injuries to be missed.
Conventional or digital subtraction angiography (see the images below) remains the criterion standard for depicting traumatic aortic rupture and aortic pseudoaneurysm. Angiography is invasive and may cause small aortic tears to be missed. Iodinated contrast media are nephrotoxic and pose a risk of anaphylaxis.
 Digital subtraction angiogram shows a pseudoaneurysm of the thoracic aorta in a man after a steering column injury. The site of these pseudoaneurysms is remarkably constant: at or near the aortic attachment of the ligamentum arteriosum; they occur less often just above the heart, at the aortic origin.
Digital subtraction angiogram shows a pseudoaneurysm of the thoracic aorta in a man after a steering column injury. The site of these pseudoaneurysms is remarkably constant: at or near the aortic attachment of the ligamentum arteriosum; they occur less often just above the heart, at the aortic origin.
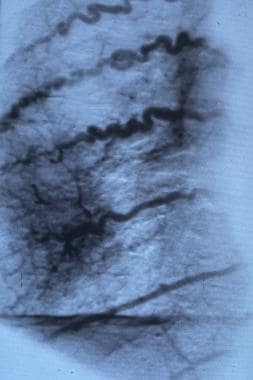
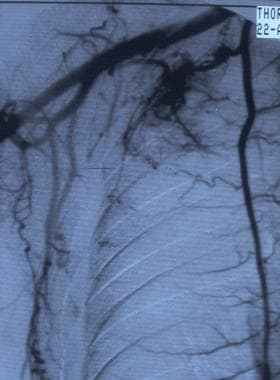 Digital subtraction angiogram shows an arteriovenous malformation at the apex of the right lung with contribution from the right subclavian artery, the intercostal arteries (T7-10), and the right internal mammary artery. Drainage of the arteriovenous malformation was via the pulmonary circulation.
Digital subtraction angiogram shows an arteriovenous malformation at the apex of the right lung with contribution from the right subclavian artery, the intercostal arteries (T7-10), and the right internal mammary artery. Drainage of the arteriovenous malformation was via the pulmonary circulation.
Nuclear medicine study
Thallium and multigated acquisition isotope scans are useful for assessing myocardial damage. Similarly, technetium-99m diphosphonate may be used to assess fracture sites when radiographs are negative and patients are symptomatic.
Injury scoring
The abbreviated injury scale (AIS) and the injury severity score (ISS) are accurate methods for quantifying trauma severity and have many potential applications. The ability to predict morbidity and mortality from trauma by using injury severity scoring is an obvious application. Such scores may be used to inform patients and their families if they desire to know the prognosis and apply the knowledge to end-of-life decision making and resource allocations. However, there is always uncertainty in predicting trauma mortality and morbidity in an individual patient. Decisions for individual patients should never be made solely on the basis of a statistically derived ISS. A variety of anatomic and physiologic trauma scores are used alone or in combination to score the severity of injuries. [14]
The AIS is an anatomic scoring system first introduced in 1969. Since then, it has been revised several times with regard to survival so that it now provides a reasonably accurate means of ranking the severity of injury. A scaling committee of the Association for the Advancement of Automotive Medicine (AAAM) monitors the AIS. The AIS is used to score traumatic injuries in terms of the anatomic location and severity of the injury. Each traumatic injury is assigned a 7-digit number, with the last number representing the severity of the injury to be used in tabulating the ISS. AIS numbers may be found in the AIS Dictionary, distributed by the AAAM.
The ISS is an anatomic scoring system but only recognizes the highest AIS in each of the 6 body regions: head, face, chest, abdomen, extremities, and external. The ISS is used to assess survivability; its results are often compared with various benchmarks (eg, ISS versus length of stay and ISS versus mortality). Only the highest AIS score in each body region is used. The scores for the 3 most severely injured body regions are squared and added to produce the ISS.
Injuries are scored on a scale of 1-6, with 1 being minor, 5 being severe, and 6 being lethal. This score represents the threat to life associated with an injury and is not meant to represent a comprehensive measure of severity. The AIS is not an injury scale in that the difference between an AIS score of 1 and a score of 2 is not the same as that between 4 and 5. The AIS scale and the organ injury scales of the American Association for the Surgery of Trauma have many similarities.
AIS scores for injury are as follows:
-
Minor
-
Moderate
-
Severe
-
Serious
-
Critical
-
Not survivable
Rodriguez et al developed a decision instrument to identify patients with no visible risk of significant trauma in order to allow for more selective chest imaging. [15] Although the instrument needs further validation, it was able to identify significant intrathoracic injury with high sensitivity at three Level 1 trauma centers.
Patient education
For patient care information, see the Lung and Airway Center; the Back, Ribs, Neck, and Head Center; and the Skin, Hair, and Nails Center. Also see Collapsed Lung, Costochondritis, Chest Pain, Puncture Wound, and Lupus (Systemic Lupus Erythematosus).
Radiography
Chest radiography is of paramount importance in thoracic trauma; only attention to life-threatening problems should delay obtaining radiographs. Systematic review of the radiograph may reveal suspected and unsuspected pathology. The bony thorax, including ribs, clavicles, scapulae, and vertebrae, should be examined for fractures. Rib fractures should be taken in context. [16]
(See the radiographic images below displaying thoracic trauma.)
Radiograph of the left shoulder of a 36-year-old man after undergoing a direct blow to the upper thorax shows a fracture of the first rib. The most common injury caused by blunt trauma is a rib fracture, which may be easily missed with suboptimal technique. Overpenetration and a decrease in the kilovolt-peak improve skeletal visualization, although at the expense of lung detail. If available, digital imaging improves visualization, and images may be displayed on a workstation and manipulated. Fractures of the first and second ribs are rare but are often overlooked; they are most often associated with serious vascular and tracheobronchial or spinal injury.
Chest radiograph in a child with a shrapnel injury after the shrapnel was removed surgically. Six months later, the child presented with increasing left supraclavicular soft tissue swelling. Left, a chest radiograph shows a soft tissue mass associated with destruction of the first left rib. Right, 2-dimensional and Doppler sonograms show a pseudoaneurysm of the left subclavian artery.
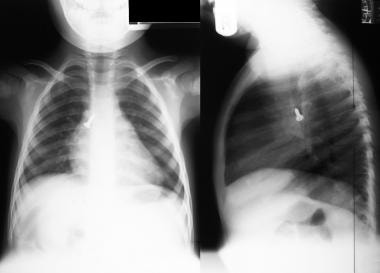
 Chest radiograph in a man with blunt thoracic trauma shows surgical emphysema and pulmonary hemorrhage, left upper lobe. The patient presented with hemoptysis following injury.
Chest radiograph in a man with blunt thoracic trauma shows surgical emphysema and pulmonary hemorrhage, left upper lobe. The patient presented with hemoptysis following injury.
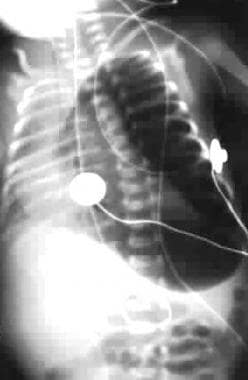
 Bilateral pneumothoraces in an infant with a deep costophrenic sulcus sign, sharp demarcation of the cardiac border, double-diaphragm contour and depression of left hemidiaphragm, and hyperlucency in lower thorax and upper abdomen.
Bilateral pneumothoraces in an infant with a deep costophrenic sulcus sign, sharp demarcation of the cardiac border, double-diaphragm contour and depression of left hemidiaphragm, and hyperlucency in lower thorax and upper abdomen.
 A 32-year-old man with gunshot wounds. Multiple lead pellets are noted in the pleura, adjacent to the thoracic aorta, spleen, and left kidney. Note the hemothorax and splenic laceration.
A 32-year-old man with gunshot wounds. Multiple lead pellets are noted in the pleura, adjacent to the thoracic aorta, spleen, and left kidney. Note the hemothorax and splenic laceration.
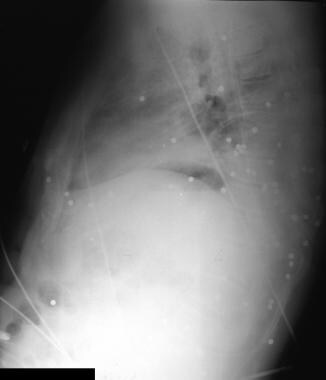
 Supine chest radiograph in a man who was stabbed. The knife has been left in the thorax. Note the associated left hemothorax and pulmonary laceration.
Supine chest radiograph in a man who was stabbed. The knife has been left in the thorax. Note the associated left hemothorax and pulmonary laceration.

 Standard chest radiograph shows mediastinal fibrosis after mediastinal radiotherapy for Hodgkin lymphoma.
Standard chest radiograph shows mediastinal fibrosis after mediastinal radiotherapy for Hodgkin lymphoma.
 Supine chest radiograph shows a misplaced jugular venous pressure line in the azygos vein.
Supine chest radiograph shows a misplaced jugular venous pressure line in the azygos vein.
 Upper gastrointestinal barium series in a patient who had accidentally swallowed his partial dentures. Upper esophagus was obstructed. Note the sharp cutoff (upper arrow) and the dentures (lower arrow). The patient inhaled the barium as a result of esophageal obstruction.
Upper gastrointestinal barium series in a patient who had accidentally swallowed his partial dentures. Upper esophagus was obstructed. Note the sharp cutoff (upper arrow) and the dentures (lower arrow). The patient inhaled the barium as a result of esophageal obstruction.
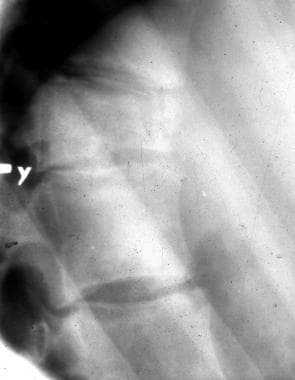 Lateral radiograph of the dorsal spine shows a wedge fracture of the tenth dorsal vertebral body after a steering column injury.
Lateral radiograph of the dorsal spine shows a wedge fracture of the tenth dorsal vertebral body after a steering column injury.
Flail chest
Flail chest is present when there are 5 or more rib fractures in a row or when 3 or more segmental fractures (2 fractures in 1 rib) are present. The significance of recognizing a flail chest is that respiratory failure may develop from paradoxical movement of the flail segment.
The soft tissues should be evaluated for surgical emphysema or opacification. The lung fields may likewise demonstrate pneumothorax, hemothorax, and consolidation suggestive of lung contusion. Radiographic abnormalities of the mediastinum, particularly pneumomediastinum, widening of the mediastinum, or shift of the mediastinum, suggest airway rupture, aortic disruption, and tension pneumothorax. Finally, assessment of the cardiac silhouette may aid in the diagnosis of blunt myocardial injury, including tamponade.
Chest wall injuries
Chest wall injuries may give clues to associated injuries. Fractures of the first 3 ribs, in particular, indicate significant trauma. Subclavian vascular injury should be suspected in patients with fractures of the first 3 ribs, the clavicle, and the scapula, particularly when they are associated with significant fracture displacement, extrapleural hematoma, brachial plexus neuropathy, or radiologic evidence of mediastinal hemorrhage. Thoracic outlet fractures may be associated with brachial plexus or vascular injuries.
Fractures of the sternum are rare; lateral and oblique thoracic views are required for diagnosis. The presence of a fractured sternum and an abnormal mediastinal contour should prompt a search for injury to the great vessels.
Pneumomediastinum
A pneumomediastinum is usually the result of a disruption of the parenchyma, with interstitial tracking of air secondary to momentary marked chest compression and reexpansion. On a chest radiograph, it is most obvious along the left heart border, outlining the parietal pleura, but the presence of visible air under the cardiac shadow — the so-called continuous diaphragm — also is a useful sign. Subcutaneous emphysema, extending into the soft tissues of the neck, often accompanies a pneumomediastinum.
The parietal pleura may be visible along the left mediastinal border. A sharply defined edge may be observed to the descending aorta. This may often be followed into the upper abdomen. Subcutaneous, retroperitoneal, or intraperitoneal emphysema may be present.
Pneumopericardium
Findings of pneumopericardium may include air lucency around the heart that does not rise above the level of pericardial reflection at the root of the great vessels.
Hemopericardium
Rapid accumulation of blood in the pericardial space often causes cardiac tamponade without altering the appearance of the cardiac silhouette.
Pulmonary contusion
The radiographic picture of pulmonary contusion is variable. Airspace opacification is present without any evidence of an air bronchogram, because the small airways are filled with blood. Depending on the extent and force of the trauma, the shadowing may be patchy or extensive and confluent; solitary, multifocal or diffuse; and unilateral or bilateral. Focal hematomas may become cavitated as they begin to organize. An air bronchogram is rare, owing to the fact that there is blood in the small airways. The distribution of the consolidation is nonsegmental and often progresses rapidly over the first 1-2 days.
Pulmonary contusion may be associated with adjacent rib fractures and homogeneous infiltrates, which tend to be peripheral and nonsegmental.
Resolution is usually rapid; the lung often returns to normal within a week. Failure of resolution usually suggests superimposed infection, atelectasis, aspiration, or a blood clot in a laceration. Contusions are generally associated with the area of maximal impact, but countercoup injuries may occur. Fractures in the overlying area of impact may be seen.
Pulmonary laceration or traumatic pneumatocele is often present in association with contusion but may not be identifiable on the radiograph. CT is more sensitive than radiography. Lacerations usually appear as oval cavities. They have a pseudomembrane a few millimeters thick. An air-fluid level may be present because of hemorrhage into the cavity, or a crescent sign may be present as a result of air outlining a hematoma. These are slowly resolving lesions; residual opacities may persist for several months.
Hemorrhage into the alveolar or bronchiolar cavities spreads and fills other normal alveoli; because these alveoli may clear themselves, impressive resolution of pulmonary contusion is frequently seen on the radiograph within 6 days. Contusion may be complicated by the spread of venous thrombosis from the site of injury during the first few days after trauma.
Pleural effusion
Pleural effusion may be associated with uniformly increased opacity over the hemithorax and a pleural cap.
Diaphragmatic rupture
Diaphragmatic rupture is diagnosed with chest radiographs. Loss of the diaphragmatic contour, an elevated asymmetric or irregular diaphragm, the presence of bowel or a nasogastric tube within the chest (U-shaped course of the nasogastric tube), and a shift of the mediastinum to the opposite side or elevation of the hemidiaphragm are findings suggestive of a diaphragmatic rupture.
Diaphragmatic injuries should be suspected in any case involving a penetrating, left-sided thoracic wound below the fourth intercostal space anteriorly, the sixth intercostal space laterally, or the eighth intercostal space posteriorly. Serial chest images may show progressive changes diagnostic of diaphragmatic rupture. Associated atelectasis, pleural effusions, lung contusions, or phrenic nerve paralysis may mask or mimic traumatic diaphragmatic tears.
Ruptured hemidiaphragm is more common on the left side than on the right. Nonspecific signs include apparent elevation of the hemidiaphragm, obliteration or distortion of the contour of the hemidiaphragm, contralateral displacement of mediastinum, and pleural effusion. The presence of gas-containing viscera in the thorax, particularly with a focal constriction across gas-containing bowel, is pathognomonic.
Hemopneumothorax may be misdiagnosed in cases involving a dilated stomach in which a horizontal air-fluid interface is seen on erect chest radiographs. In the absence of a right rib, a small right hemothorax with a high right diaphragm is suggestive of a ruptured diaphragm. Findings are initially absent in 25-50% of patients.
Pneumothorax
A high index of suspicion for the presence of a pneumothorax must be maintained in all cases of blunt trauma. Auscultation may be difficult in the emergency department. Other signs of tension pneumothorax, tracheal deviation, hypotension, or hypoxemia should trigger chest decompression before chest radiography.
If the patient is stable, radiography may precede thoracostomy. Patients with multiple rib fractures may have a subclinical pneumothorax and may require prophylactic thoracostomy.
Findings in pneumothorax include the following:
-
Deep costophrenic sulcus
-
Double-diaphragm contour with or without depression of the hemidiaphragm
-
Hyperlucency in the lower thorax and upper abdomen
-
Sharp demarcation of the cardiac apex
-
Possible outlining of the visceral pleura at the base of the lung
Bronchial tear
Evidence of a bronchial tear should be sought on plain radiographs when one or more of the following factors are present: a pneumothorax persists despite adequate placement of chest drains; there is increasing subcutaneous emphysema; a pneumomediastinum is present; or a pneumothorax is present. Tracheal transection may occur in the setting of neck trauma.
Radiographic findings include elevation of the hyoid bone on lateral cervical spine radiographs. The hyoid bone may lie above the level of the C3 vertebral body or greater cornu, less than 2 cm from the angle of the mandible. The elevation of the hyoid bone is said to be related to rupture of the infrahyoid muscles with unopposed action of the suprahyoid muscles.
Aortic injury
Aortic injury should be suspected on chest radiographs showing mediastinal widening of more than 8 cm, loss of definition of the aortic knuckle, displacement of the nasogastric tube to the right of the T4 spinous process, and a left apical pleural cap. Further evidence is gained from widened paraspinal lines, a right paratracheal stripe widened by more than 5 mm, and loss of the descending aorta line. The negative predictive value of a normal chest radiograph is 98%.
Esophageal rupture
A large left pneumothorax, extensive pneumomediastinum, subcutaneous emphysema, left pleural effusion, left lower-lobe atelectasis, and the V sign of Naclerio on a plain radiograph suggest an esophageal rupture.
Thoracic spinal fracture
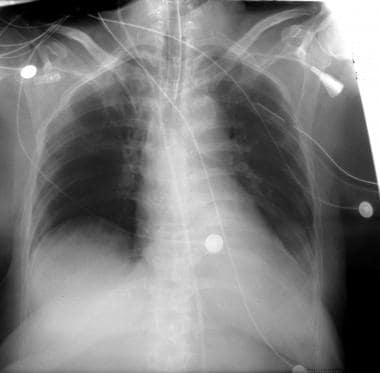
Radiographic findings of thoracic spinal fractures include widening of the paraspinal lines; mediastinal widening; loss of height of the vertebral body or obscuration of a pedicle or pedicles; a left apical cap; and deviation of the nasogastric tube.
Despite the serious clinical implications of fractures of the thoracic spine, such fractures often go undetected during the initial critical hours of patient evaluation and treatment. This is often related to the fact that the thoracic spine is infrequently examined radiologically in the acute setting. A deliberate and meticulous search should be made on the initial supine chest radiograph for spinal fractures.
Findings of a thoracic spinal fracture include a cortical breach; abnormality of shape; and paraspinal soft tissue swelling, which appears as widening of the right or left paravertebral stripe (produced by an associated paravertebral hematoma).
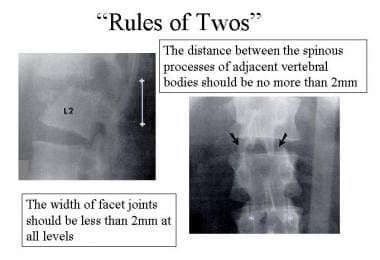
The rules of 2s provide further evidence of vertebral fractures (see the images below).
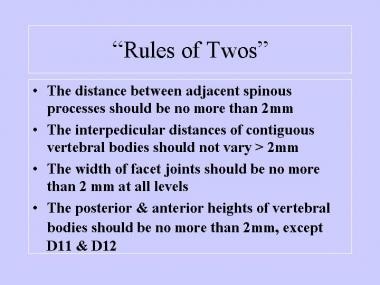
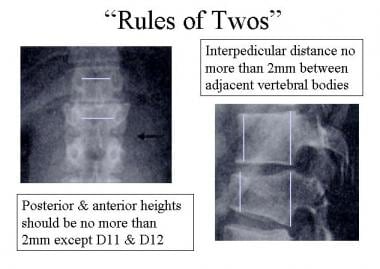 Rules of 2s: (1) The distance between adjacent spinous processes should be no more than 2 mm. (2) The interpedicular distances of contiguous vertebral bodies should not vary more than 2 mm. (3) The width of facet joints should be no more than 2 mm at all levels. (4) The posterior and anterior heights of vertebral bodies should be no more than 2 mm, except at D11 and D12.
Rules of 2s: (1) The distance between adjacent spinous processes should be no more than 2 mm. (2) The interpedicular distances of contiguous vertebral bodies should not vary more than 2 mm. (3) The width of facet joints should be no more than 2 mm at all levels. (4) The posterior and anterior heights of vertebral bodies should be no more than 2 mm, except at D11 and D12.
 Rules of 2s: (1) The distance between adjacent spinous processes should be no more than 2 mm. (2) The interpedicular distances of contiguous vertebral bodies should not vary more than 2 mm. (3) The width of facet joints should be no more than 2 mm at all levels. (4) The posterior and anterior heights of vertebral bodies should be no more than 2 mm, except at D11 and D12.
Rules of 2s: (1) The distance between adjacent spinous processes should be no more than 2 mm. (2) The interpedicular distances of contiguous vertebral bodies should not vary more than 2 mm. (3) The width of facet joints should be no more than 2 mm at all levels. (4) The posterior and anterior heights of vertebral bodies should be no more than 2 mm, except at D11 and D12.
The rules state the following:
-
The distance between the spinous processes of adjacent vertebral bodies should not vary by more than 2 mm from the interspinous distance, as measured below and above.
-
The interpedicular distance of contiguous vertebral bodies should not vary by more than 2 mm
-
The vertical distance between the pedicles of contiguous vertebral bodies should not vary by more than 2 mm from the interpedicular distance between adjacent pairs of vertebral bodies immediately above and below the level of concern
-
The width of facet joints should be less than 2 mm at all levels
-
The posterior height of a thoracic vertebral body should not be over 2 mm greater than the anterior height except at D11 and D12, where the vertebral bodies are inherently wedged anteriorly
Discovery of a fracture of the spine should prompt a search for others because 10% of spinal fractures are multiple. Examination of the whole of the spine is necessary because 80% of spinal fractures are not contiguous.
Impalement injuries
With impalement injuries, a chest radiograph may show the intrathoracic foreign body, particularly if the foreign body is metallic and there are associated pneumothorax/pleural effusions and lung lacerations; a chest radiograph may also show the proximity of the foreign body to vital intrathoracic structures. If time allows, CT scanning may depict vascular injuries more clearly. Aortography also may be useful when hematomas lie close to the aorta or when an aortic or major arterial leak is suspected.
Degree of Confidence
Hehir and colleagues assessed the accuracy of the initial chest radiograph in diagnosing moderate to severe chest injuries. [17] The prospective Westmead Trauma Registry identified 100 patients as having a chest injury with an AIS score of 3 or greater. The male-to-female ratio was 4.9:1; the age range was 5-74 years. Interpretations of the initial chest radiograph were compared with the chest injuries as finally diagnosed. In 19 of 77 survivors and in 8 of 17 patients who underwent radiography before death, significant abnormalities (primarily pneumothorax, hemothorax, and spinal and sternal injuries) went undiagnosed on the basis of the initial chest radiograph.
A standard posteroanterior chest radiograph and lateral projections are said to accurately show most major intrathoracic pathology. However, initial chest radiographs of trauma patients are often obtained with the patient supine, suboptimally, and soon after arrival, even though a chest injury may not be immediately apparent. The limitations of a mobile chest radiograph must be appreciated; more formal chest radiography, with posteroanterior and lateral imaging, is advised at a later stage if the clinical situation permits.
False Positives/Negatives
Several technical factors regarding the AP portable radiograph that is obtained in the emergency setting may cause the mediastinum to appear widened. These factors are the supine position, the expiratory image, and the magnification effect of a short beam distance.
Diaphragmatic injuries are often missed on plain radiographs. Preexisting conditions, such as diaphragmatic eventrations or an elevated hemidiaphragm, may mimic diaphragmatic injuries. Most plain imaging findings associated with aortic transection are nonspecific. They may be seen in a variety of mediastinal or chest wall injuries, including nonaortic vascular injuries, fractures of the sternum, vertebral fractures, and esophageal ruptures.
Radiographic findings of thoracic spinal fractures are often subtle and difficult to identify because of the limited quality of many trauma radiographs. In one series, only 51% of spinal fractures were identified on the initial chest radiograph. Many plain radiographic findings are not specific for vertebral body injury and may be seen with other mediastinal injuries, including traumatic aortic rupture. In fact, 69% of patients with thoracic spine fractures have chest imaging findings suggestive of aortic transection.
In about 78% of patients whose chest radiographs are abnormal and show signs of mediastinal widening, findings on CT scans are normal; in 80%, angiograms do not show evidence of aortic injury. In the trauma setting, predictions of the presence of mediastinal hemorrhage on supine portable chest images are inaccurate.
Computed Tomography
The advent of fast scanning helical and multisection CT scanning has changed the management of blunt lung trauma; these modalities permit the detection of blood in the bronchi, as well as interstitial air or blood, with greater accuracy. Many centers now screen chest trauma patients for aortic injuries by use of CT scanning of the chest. [9, 10, 11, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27]
See the CT scans below displaying thoracic trauma injuries.
Transaxial, nonenhanced computed tomography scan shows a pneumothorax in a patient in whom the chest radiograph was normal.
 A 32-year-old man with gunshot wounds. Multiple lead pellets are noted in the pleura, adjacent to the thoracic aorta, spleen, and left kidney. Note the hemothorax and splenic laceration.
A 32-year-old man with gunshot wounds. Multiple lead pellets are noted in the pleura, adjacent to the thoracic aorta, spleen, and left kidney. Note the hemothorax and splenic laceration.
 Coronal reconstruction of contrast-enhanced computed tomography scan shows the omentum occupying the left hemithorax because of a diaphragmatic rupture.
Coronal reconstruction of contrast-enhanced computed tomography scan shows the omentum occupying the left hemithorax because of a diaphragmatic rupture.
 Contrast-enhanced axial computed tomography scan through the mid-thorax in a 36-year-old man with a history of blunt thoracic trauma shows thickening of the right anterior serratus muscle associated with an arteriovenous extrathoracic-intrathoracic communication.
Contrast-enhanced axial computed tomography scan through the mid-thorax in a 36-year-old man with a history of blunt thoracic trauma shows thickening of the right anterior serratus muscle associated with an arteriovenous extrathoracic-intrathoracic communication.
 Coronal computed tomography scan of the thorax seen on a soft-tissue window, showing a stab-wound defect in the left anterior chest wall. Note the left upper lobe contusion/laceration and a large pneumothorax.
Coronal computed tomography scan of the thorax seen on a soft-tissue window, showing a stab-wound defect in the left anterior chest wall. Note the left upper lobe contusion/laceration and a large pneumothorax.
CT scans demonstrate lung, pleural, mediastinal, and chest wall injuries better than radiographs do. About 90% of patients do not have aortic injuries, but many other serious, unsuspected injuries may be identified on chest CT scans, and with greater frequency. Many serious thoracic injuries may be overlooked on initial chest radiographs; these include tracheobronchial tears, diaphragmatic rupture, esophageal tears, thoracic spine injuries, chest wall and seat-belt injuries, lung contusion, cardiac injuries, pneumothorax, hemothorax, and complications related to chest tubes. [28, 29]
Chest wall trauma
Rib fractures are common in blunt chest trauma (60%). When they occur, the rib fracture fragments can transform a blunt injury mechanism into a local penetrating injury. Consideration should be given to adjacent soft tissue structures and how the fracture fragments may cause associated injury, such as lacerations to the adjacent pleura or lung. Fractures of the lower ribs can be associated with injury to abdominal organs, whereas upper rib fractures, while rare, may be associated with injuries to adjacent vessels or the brachial plexus. [5] Portable supine chest images are insensitive and depict only about 20% of all rib fractures. Fractures of the first rib are an indication of severe blunt chest trauma and may be associated with aortic tears, bronchial tears, and injuries to the subclavian vessels.
Other conditions resulting from chest wall trauma include soft tissue hematomas and contusions. These are often evident on CT scans of the chest; CT scanning often shows the region of primary impact. The presence of overlying soft tissue edema or hematoma on CT scans often indicates injury to an underlying rib or other bony injury; these injuries should be sought by reviewing the images using bone window settings that have been reformatted using an edge-enhancing algorithm. Using the cine or paging mode facilitates bone-image review. Lacerations of chest-wall arterial vessels may result in massive chest-wall hematomas.
Seat-belt injuries related to a 3-point restraint may cause bruises in the subcutaneous tissues and fat of the anterior chest wall. These may be identified on CT scans. Seat-belt injuries severe enough to cause skin abrasions are associated with significant internal injuries in 30% of patients. Thus, the identification of seat-belt bruises on CT scans should prompt a careful search for the following:
-
Fractures of the sternum, ribs, clavicles, and transverse processes of C7 or T1
-
Aortic transection
-
Cardiac contusions or ventricular rupture
-
Vascular injuries to the subclavian artery or superior vena cava
-
Tracheal or laryngeal tears
-
Diaphragmatic rupture
The incidence of sternal fractures is actually higher in seat-belt users than in nonusers; most fractures occur within 2 cm of the manubrium-sternum junction.
CT scanning often reveals unsuspected sternal fractures in blunt thoracic trauma, sternoclavicular dislocations, unsuspected rib and vertebral body fractures, and unrecognized scapular and shoulder injuries. These injuries are usually difficult to identify on hard-copy images and are more easily seen on a monitor in cine or paging mode. Two-dimensional coronal and sagittal reconstructed images often demonstrate sternal fractures and sternoclavicular dislocations better than transaxial images do.
Fractures of the thoracic spine occur in 3% of patients with blunt thoracic trauma; a high percentage are associated with spinal cord injury. The site most vulnerable to fractures is the thoracoabdominal junction involving the T9-T11 vertebral bodies. Sternal fractures are often associated with thoracic spinal fractures.
Signs of vertebral body fractures on CT scans include the following:
-
Paraspinal hematoma
-
Disruption or fracture of the vertebral body, pedicle, and/or spinous processes
-
Mediastinal hematoma confined to the posterior mediastinum, which often suggests a vertebral body fracture
-
Compression fractures, which may be easily overlooked on axial CT scans of the chest unless bone windows are used
Reconstructed sagittal and coronal multiplanar images are often useful in confirming the presence of a simple compression fracture. One may also verify compression fractures by reviewing the lateral CT scanogram.
Pneumothorax and hemothorax
Small to moderate pneumothoraces may not be appreciated on plain chest radiographs but are readily identified on CT scans. CT is also more specific than plain radiography in characterizing pleural effusions. Hemothoraces often show areas of high CT attenuation as a result of the presence of blood. A rapidly accumulating pleural effusion in the setting of trauma may be caused by a hemothorax or a chylothorax resulting from a ruptured thoracic duct.
A persistent or increasing pneumothorax or hemothorax may have a variety of causes, including bronchial tears, vascular injuries, and malfunctioning or malpositioned chest tubes. Hemothorax is more common in penetrating injuries to the chest than in nonpenetrating injuries. If the hemorrhage is severe, hypovolemic shock and respiratory distress may result from compression of the lung on the involved side.
A tension pneumothorax develops when air enters the pleural space but cannot leave. The consequence is progressively increasing intrathoracic pressure in the affected side, resulting in mediastinal shift. The patient will become short of breath and hypoxic. Urgent needle decompression is required before the insertion of an intercostal drain. The trachea may be displaced (late sign) and is pushed away from the midline by the air under tension.
Lung contusion and laceration
CT scanning often shows more extensive edema and hemorrhage than are seen on the chest radiograph. A plain chest radiograph also causes gross underestimation of the frequency of lung laceration in the lung contusion.
A common finding on CT scans is an irregular lucency within the contusion, which is often adjacent to the area of rib injury. A lung laceration often becomes visible on a chest radiograph when the contusion regresses. The appearance of a laceration is variable and depends on the substance filling the laceration. When full of blood, the laceration may appear as an oval opacity; when full of air, it may appear as a lucency; when both air and fluid are present, it may appear as an air-fluid level; and when air and a blood clot are present, it may appear as a mass within a lucency.
Lacerations may have a more complex appearance. Many lacerations show several appearances during the course of their resolution. Regression often takes weeks, and residual nodules or scars may persist for weeks or months. In severe blunt chest trauma, one may see pulverized lung on CT scans or an area of airspace opacification with multiple, small (5 mm to 1 cm) air cysts disrupting the lung parenchyma. For the detection of contusions and lacerations, CT is more sensitive than plain radiography by a factor of 3 to 1.
Pulmonary contusion is a potentially life-threatening condition. The onset of symptoms may be slow and may progress for 24 hours after the injury. Pulmonary contusion is likely to occur in cases of high-speed accidents, falls from great heights, and injuries caused by high-velocity bullets. Symptoms and signs include dyspnea, hypoxemia, tachycardia, rare or absent breath sounds, rib fractures, and cyanosis.
Multi-detector computed tomography (MDCT) is a superior imaging modality in diagnosing and evaluating pulmonary contusion. Contusions on MDCT appear as crescentic ground-glass opacities (opacities through which lung interstitium and vasculature are still visible) and areas of consolidation that often do not respect the anatomic boundaries of the affected lobes. Small pulmonary contusions may exhibit subpleural sparing and may distinguish contusion from pneumonia or other lung pathology. Although pulmonary laceration is typically the result of penetrating trauma, laceration may also be caused by displaced rib fractures or significant shearing forces on the lung without penetrating injury. Because of elastic recoil of the normal pulmonary parenchyma surrounding the injury, pulmonary lacerations may present as late as 48 to 72 hours after injury. Pulmonary lacerations may appear similar to pulmonary contusions on chest radiography initially and will require MDCT for definitive diagnosis. [30]
Several other causes of airspace opacification may be seen on plain radiographs and on CT scans in the setting of thoracic trauma. These include aspiration pneumonia; atelectasis, caused by splinting or mucous plugs; and cardiogenic and noncardiogenic pulmonary edema. After 24 hours, one must also consider fat embolism and ARDS, particularly in cases of severe trauma with long bone fractures.
Tracheobronchial tears
Tears or fractures of the airways occur in approximately 1.5% of cases of blunt chest trauma. They frequently go unrecognized on initial examination, and delayed diagnosis is common. Bronchial fractures occur within 2.5 cm of the carina in 80% of patients.
CT findings of bronchial fractures include the following:
-
A large pneumothorax despite adequate placement of one or more chest tubes
-
Massive pneumomediastinum and subcutaneous emphysema
-
Focal peribronchial collections of air
-
Discontinuity or irregularity of the bronchial wall
-
Drooping, or collapsed lung or lobe of the lung
The fallen-lung sign refers to the unusual appearance of a collapsed lung or lobe in the setting of bronchial injury. A fallen-lung sign is thought to result from disruption of the normal hilar attachments of the lung, causing the collapsed lung to droop peripherally rather than centrally.
Another clue to tracheal tears seen on plain radiographs and CT scans is abnormality in the appearance or position of the endotracheal tube (ET). Abnormalities include overdistention of the ET cuff, protrusion of the ET tube wall beyond the expected margins of the tracheal lumen, and an extraluminal position at the tip of the tube. Associated fractures of the upper thorax—including fractures of the first 3 ribs, the clavicle, the sternum, and the scapula—occur in 40% of patients with tracheobronchial injuries. Suspected tracheobronchial tears are confirmed with bronchoscopy.
Esophageal rupture
CT findings of esophageal rupture include focal extraluminal air collections at the site of tear and a hematoma of the mediastinal or esophageal wall. Occasionally, a tract at the site of the tear can be identified on CT scans. In the setting of severe blunt chest trauma, the esophagus may also be obstructed and entrapped by fracture-dislocations of the thoracic spine, as demonstrated on chest or thoracic spinal CT scans. The diagnosis of esophageal rupture is usually confirmed with a swallow study involving nonionic oral contrast material.
Cardiac injury
On the basis of autopsy data, the frequency of cardiac injury from blunt trauma is estimated to be 10%. In patients with blunt chest trauma, myocardial contusion is associated with fractures of the sternum or ribs. Cardiac contusion may simulate a myocardial infarction. This type of injury is more common than has been realized; it may cause sudden death well after the accident. Cardiac injuries resulting from blunt chest trauma include cardiac contusions, cardiac rupture, pneumopericardium and hemopericardium, cardiac tamponade, and cardiac valve dysfunction.
The diagnosis of cardiac contusion is supported by abnormalities on ECG and elevation of serial cardiac enzyme levels, if these measurements are available. Cardiac injury is suspected when abnormal ECG tracings are recorded and when hemopericardium is recognized on CT scans. Hemopericardium is evinced by the presence of air or high-attenuation blood in the pericardial sac; both may cause cardiac tamponade and may require emergent pericardial drainage. Constrictive pericarditis may develop as a long-term complication of hemopericardium.
Echocardiography is often used at the bedside to evaluate the patient for cardiac injuries; however, hemopericardium, in particular, may be missed on echocardiograms because of the change in the echo properties of hemorrhagic fluid.
Pericardial tamponade
Penetrating cardiac injuries are a leading cause of death in urban areas. It is rare to have pericardial tamponade with blunt trauma.
Pericardiocentesis must be undertaken early if this injury is considered likely. Pericardial tamponade should be suspected in patients presenting with shock; distended neck veins; cool extremities in the absence of a pneumothorax; or muffled heart sounds.
Injury to the pulmonary veins and arteries is often fatal; it is one of the major causes of on-site death.
Aortic injury
Historically, conventional angiography was considered the criterion standard for the diagnosis of blunt traumatic aortic injury (TAI); however, CT has evolved as the preferred screening and diagnostic modality for TAI because of its availability, rapidity, and ability to diagnose additional intra-thoracic injuries. The practice managment guidelines published by the Eastern Association for the Surgery of Trauma (EAST) include a strong recommendation for the use of a CT scan of the chest with intravenous contrast for the diagnosis of clinically significant blunt TAI. [31]
CT angiography is increasingly being used as the investigational modality of choice to exclude aortic injury. Emergent treatment depends on accurate, early diagnosis. Direct findings include presence of an intimal flap, pseudoaneurysm, abnormal aortic contour due to mural hematoma, and contrast extravasation. A periaortic hematoma is a sensitive finding of aortic injury. [32]
Diaphragm rupture
Diaphragm rupture occurs in 0.8-8% of cases of blunt thoracic trauma. The plain chest radiograph is abnormal in 77% of patients, but the findings are nonspecific and the diagnosis is initially missed in most cases. Mortality in unrecognized cases is 30%; death occurs as a result of delayed herniation of abdominal viscera and bowel strangulation. Early recognition and repair of diaphragmatic tears improves the prognosis.
In recognized cases, diaphragmatic rupture is more common on the left side (77-90%) than on the right. Most tears are large (>10 cm) and occur in a radial orientation in the posterolateral location. The diaphragm is the weakest at this location because this is where the pleuroperitoneal membrane finally closes during embryogenesis. Visceral herniation occurs in 32-58% of patients with diaphragmatic tears; the stomach is the most common abdominal viscus to become herniated. About 72% of patients with diaphragmatic rupture have other intra-abdominal injuries; 42% have pelvic fractures, which are indicative of the severity of trauma in these cases.
The helical scanning technique should include thin, overlapping sections acquired during a single breath-hold; multiplanar reconstructions in the sagittal and coronal plane may be generated to detect discontinuities of the diaphragm. The reported sensitivity and specificity of CT scanning for the detection of diaphragmatic rupture are 61% and 87%, respectively. Sagittal and coronal reformations are superior to axial images in detecting tears and the herniation of abdominal contents into the thorax.
Normal discontinuities in the posterior aspects of the diaphragm are identified in approximately 6-11% of patients with no history of trauma; these discontinuities may be related to congenital Bochdalek hernias. Moreover, with aging, acquired diaphragmatic humps and bumps become more prevalent; they have been reported in 35% of patients in their 70s.
CT findings of diaphragmatic rupture include the following:
-
Discontinuity of the diaphragm (73-82%)
-
Herniation of peritoneal fat, bowel, or abdominal organs into the chest (55%)
-
Collar sign or a waistlike constriction of bowel (27%)
-
Peritoneal fat, bowel, or viscera lateral to the lung or diaphragm or posterior to the crus of the diaphragm
-
Absent diaphragm sign
-
Concurrent pneumothorax and pneumoperitoneum
-
Concurrent hemothorax and hemoperitoneum
Dependent viscera sign
Bergin and colleagues coined the phrase "dependent viscera sign" to describe CT findings associated with a ruptured diaphragm. [33] Besides noting discontinuity of the diaphragm, intrathoracic herniation of abdominal contents, and waistlike constriction of bowel (the collar sign), they also assessed whether the upper one third of the liver abutted the posterior right ribs or whether the bowel or stomach was in contact with the posterior left ribs. Either of the last 2 findings was referred to as the dependent viscera sign.
Using CT, the authors observed the dependent viscera sign in 100% of patients with a left-sided diaphragmatic rupture and in 83% of patients with a right-sided diaphragmatic rupture. Using the dependent viscera sign, the radiologists' overall detection rate for diaphragmatic rupture was 90%.
False positives/negatives
When data from multiple studies are combined, the false-positive rate for CT scanning with a variety of techniques is estimated to be 0 to 39%; the false-negative rate is estimated to be 0.7%.
False-positive results arise from mimics of mediastinal hemorrhage; these include residual thymic tissue, periaortic atelectasis, volume averaging of the pulmonary artery, and pleural effusions adjacent to the descending aorta. False-positive findings may also result from image degrading caused by patient motion; streak artifacts from ECG leads and other monitoring devices; and streak artifacts from opaque intravenous contrast material.
Atherosclerotic plaques may cause interpretation difficulties, and a prominent ductus arteriosus remnant may mimic a traumatic pseudoaneurysm. False-positive diagnoses of intimal flaps have been caused by crossing vessels and volume averaging of the left brachiocephalic vein as it crosses in front of the aortic arch, the left superior intercostal vein, and the right bronchial arteries coming off the descending aorta.
Aortic injuries in certain anatomic locations may be missed, such as injuries near the root of the aorta (these injuries may be missed as a result of cardiac pulsation). False-negative results may also occur in cases involving small tears that are confined to the distal aortic arch at the transition point between the distal arch, because of the obliquity of the scanning plane. [34]
Magnetic Resonance Imaging
MRI is usually reserved for the evaluation of stable patients in whom CT scanning results are equivocal or nondiagnostic. MRI is also an excellent tool in the diagnosis of vascular injuries in stable patients. MRI is a sensitive technique in the diagnosis of vertebral, sternal, and scapular fractures and may be valuable in documenting disruption of the diaphragm. Coronal and sagittal T1-weighted images may be used to trace the course of the diaphragm from its insertion sites to the dome of the hemidiaphragm on the suspected side. [35, 36, 37, 38, 39]
MRI may be particularly helpful in difficult cases in which the differential diagnosis is between diaphragmatic injury and eventration or preexisting elevation of the hemidiaphragm. The hemidiaphragm may be visualized with MRI as a hypointense band throughout its course; it is outlined by hyperintense abdominal and mediastinal fat on the left and by the liver on the right. Also, low tears involving the crus of the diaphragm are more convincingly displayed with coronal T1-weighted images than with axial CT scans.
MRI has many advantages over CT scanning in the evaluation of patients with suspected dorsal spine injuries. MRI provides excellent detail of intervertebral discs, spinal ligaments, paravertebral soft tissues, and other spinal contents (eg, cord and nerve roots). This study is particularly useful in evaluating patients with spinal cord injury without radiographic abnormality (SCIWORA) syndrome. The images show cord edema or hematoma to account for any neurologic deficit the patient may have. Diaphragmatic injuries occur in 0.8-8% of patients after blunt trauma.
The ability to directly acquire coronal, axial, and sagittal images is a major advantage of MRI in evaluating diaphragmatic injuries. MRI accurately depicts the anatomy of the diaphragm. MRI may be used for late diagnosis or for the evaluation of a patient in stable condition whose diagnosis is equivocal and for whom there is no need for laparotomy (as would be needed for some penetrating injuries).
Ultrasonography
A targeted ultrasonographic examination is a quick and noninvasive procedure that may be performed at the patient's bedside. This study may also be used as a part of a clinical examination of a patient with severe trauma. [40, 41, 42, 43, 44, 45, 46, 47, 48, 49]
Focused assessment for the sonographic examination of the trauma patient (FAST) may be completed in about 2.5 minutes by use of a 3.5-MHz transducer. A sequential examination is performed, beginning with the pericardial area, the right and left upper quadrants, and the pelvis. The pericardial area is scrutinized for the presence of blood for the detection hemopericardium. A prompt evacuation of pericardial blood through a pericardiocentesis, under ultrasonographic guidance, is mandatory for cardiac tamponade. Thoracic sonograms are obtained by moving the transducer slightly cephalad when the right and left upper quadrants of the abdomen are evaluated during FAST, with scanning performed through the intercostal spaces along the anterolateral thoracic wall. If initially negative, the FAST can be repeated as clinically indicated. [50]
Sisley and colleagues compared the speed and accuracy of sonography with those of supine portable chest radiography in patients with blunt and penetrating thoracic injuries. [51] Thoracic sonography demonstrated 97.5% sensitivity and 99.7% specificity, similar to portable chest radiography's 92.5% sensitivity and 99.7% specificity. Performance times, however, were faster for thoracic ultrasonography than for portable chest radiography.
If pleural fluid is detected, sonography-guided thoracentesis may be performed immediately, and the diagnosis of hemothorax may be confirmed. Quick confirmation of a hemothorax is important. A simple pneumothorax is frequently treated with the insertion of a chest tube into the second intercostal space in the midclavicular line, and a hemothorax is best treated with the placement of a large-caliber chest tube into the fourth or fifth intercostal space, anterior to the midaxillary line, to evacuate blood. Evacuation of blood with a well-positioned chest tube reduces the risk of clotted hemothorax and pleural empyema.
Ultrasonography has a high specificity in the diagnosis of pulmonary contusion, which is often misinterpreted on chest radiographs as pleural effusion. The sonographic characteristics are those of a hypoechoic, irregular, heterogeneous interior lesion with irregular posterior shadowing.
Ultrasonography is a useful, simple technique in the diagnosis of diaphragmatic injury. These injuries may be missed if the radiograph is misinterpreted as indicating acute gastric dilatation, an elevated diaphragm, a loculated pneumothorax, or a subpulmonary hematoma. The diaphragmatic areas are scanned in transverse and longitudinal planes, with the depth of the sound beam focused on the echogenic line representing the diaphragmatic layers. The most important element is the visualization of an interruption in this echogenic line or the appearance of bowel or stomach in the thoracic cavity during the chest examination; the presence of an ipsilateral hemoperitoneum and pleural effusion increases the likelihood that the diaphragm is injured.
Ultrasonography is also used to evaluate patients who have undergone stab wounds to the thoracoabdominal area; it is employed to delineate the subcutaneous and fascial layers, to identify the wound tract, and to detect wounds that violate the peritoneum or the parietal pleura. Rib fractures are common in cases of blunt thoracic trauma, although ultrasonography does not replace chest radiography.
Ultrasound examination with a high-frequency probe may be guided by localized pain, tenderness on palpation, and crepitus, which reflect the rib fracture. Sonography may also be used to visualize a subperiosteal hematoma in the absence of fracture; such a hematoma is seen as an area of low echogenicity corresponding to a well-defined painful zone. Ultrasonography also aids in diagnosis of a fracture of anterior cartilages or separation of costochondral junctions — injuries that are usually not seen on radiographs. Sternal fractures are often associated with pulmonary contusion and a blunt cardiac injury; therefore, its detection is important. Sternal fractures may be detected by use of a high-frequency linear scanner.
Fenkl and colleagues performed ultrasonographic examinations of sternal fractures in 16 patients, detecting all of the fractures in less than 1 minute. [52]
Degree of confidence
Ultrasonography is a rapid, sensitive, and specific diagnostic test for the detection of pericardial tamponade, hemothorax, and sternal fracture, and it provides guidance for placement of intravenous catheters and pericardial and pleural drains. Thus, sonography may help reduce complications from malpositioned tubes.
Ultrasonography of the anterior and lateral chest identifies pneumothorax and hemothorax with greater sensitivity and specificity than supine chest radiography. [50]
Transesophageal sonography is an excellent technique for visualizing aortic injuries, particularly in the region of the aortic arch and the descending thoracic aorta. Most traumatic aortic lacerations occur at these sites, which are difficult to image with traditional methods.
Ultrasonography provides a virtually infinite number of available imaging planes; it is ideal for visualizing the diaphragm directly, and it may be used to noninvasively demonstrate diaphragmatic disruption. It is particularly useful in right diaphragmatic rupture because the liver provides an excellent acoustic window. Obese patients, patients with wound dressings or extensive surgical emphysema, and patients with painful soft tissue injuries or painful thoracic wall injuries cannot be adequately scanned.
Thoracic wall injuries and spinal injuries are difficult to detect on sonograms. The appearances of diaphragmatic rupture on sonograms are nonspecific, and diaphragmatic disruption has many causes.
Nuclear Imaging
For symptomatic patients whose radiographs are negative, skeletal scintigraphy with technetium-99m diphosphonate is an effective means of diagnosing fractures that are too subtle to be seen on radiographs. The 3-phase bone scan increases sensitivity in cases of acute injury; histamine release induces hyperemia as the first response.
Thallium-201 chloride myocardial scintigraphy may be used to detect areas of decreased perfusion, and it can differentiate an acute lesion from a preexisting one. The use of other myocardial perfusion agents, as in indium-111 antimycin scintigraphy, has shown the potential of this modality as a second-line test. These studies can contribute to one's understanding of the underlying pathophysiology of blunt cardiac injury, but they are neither widely available nor useful in the evaluation of patients in stable condition.
Radionuclide angiography has been evaluated extensively in patients with blunt chest trauma. Studies suggest that in 20-70% of patients with multiple injuries, the ejection fraction is decreased. These functional abnormalities are not correlated with ECG or enzyme changes, right-sided ECG abnormalities, or the development of cardiac complications.
Skarzynski and colleagues described a case in which a fat embolism in a ventilation/perfusion scan showed a matched defect. [53] Forty-eight hours after suffering a fracture of the tibia and fibula, a 27-year-old man developed the triad of findings — neurologic changes, respiratory distress, and petechiae — characterizing the fat embolism syndrome. Chest radiography was normal initially but progressed to show bilateral, fluffy, diffuse infiltrates, which aided the diagnosis. Ventilation/perfusion lung images were obtained when the radiographic changes appeared; these images showed matching defects. The cause was considered to be the transcapillary passage of lipid breakdown products. The upper half of the lung fields was the most greatly affected region, although a reduction in ventilation/perfusion was observed in all parts of the lung. In contrast, emboli of venous origin most often involve the lung bases.
Degree of confidence
Many report that the sensitivity of radionuclide bone scans for acute fractures is 100% 3 days after injury in young adults; in the elderly, the sensitivity is 95-98%. Thus, a fracture should not be excluded in any age group earlier than 72 hours after injury.
Radionuclide cardiac imaging has not been shown to be useful on a routine basis, and in several studies, it has been shown to add no benefit over ECG or echocardiography. Radionuclide angiography appears to possess high sensitivity but to have low predictive value. It has the additional disadvantage of being invasive, and it has not been extensively studied in a stable population. Radionuclide imaging should not be viewed as a screening tool in patients with thoracic trauma.
Multigated acquisition scans have not been shown to be useful in predicting complications from blunt cardiac injury. Abnormal thallium-201 uptake correlates with abnormal ECG findings, but it is no better than echocardiography with respect to the prediction of complications from blunt cardiac injury.
Single-photon emission CT has been shown to be a useful predictor of the development of arrhythmias secondary to blunt cardiac injury. However, ECG findings, which are acquired noninvasively, may be predictive of the same outcome.
False positives/negatives
The detection rate for acute fractures decreases drastically in elderly osteoporotic patients, in patients using steroids (which suppress the osteoblastic response), and in patients with stable fractures. Movement must be present at the fracture site to incite an osteoblastic reaction and hence provoke a positive response to bone-seeking radionuclides. Thus, stable spinal fractures and nondisplaced skull fractures may be missed on radionuclide scans.
With bone scanning, factors and conditions that may lead to false-positive results for fractures include the following: healing soft tissue wounds; rhabdomyolysis; intramuscular injection sites; hematoma; myocardial contusion; and heterotopic ossification sites.
Thallium scanning and radionuclide angiography cannot be used to differentiate cardiac contusion from other cardiac pathologies, such as cardiac sarcoidosis, cardiac amyloid, myocardial malignancy, and myocardial infarction.
Angiography
Contrast-enhanced angiography remains the criterion standard for diagnosis, but it is not without risks. The major problem is that of logistics, because with its use, other diagnostic and therapeutic procedures are disrupted, and the patient must be transported from the protected resuscitation area to a specialized aortography suite. The procedure is also invasive and time consuming, and consultation with another specialist is required. In cases in which an angiogram is requested on the basis of findings of a widened mediastinum on chest radiography, only 3% of the aortograms are positive. (See the images below.)
Digital subtraction angiogram shows an arteriovenous malformation at the apex of the right lung with contribution from the right subclavian artery, the intercostal arteries (T7-10), and the right internal mammary artery. Drainage of the arteriovenous malformation was via the pulmonary circulation.
 Digital subtraction angiogram shows an arteriovenous malformation at the apex of the right lung with contribution from the right subclavian artery, the intercostal arteries (T7-10), and the right internal mammary artery. Drainage of the arteriovenous malformation was via the pulmonary circulation.
Digital subtraction angiogram shows an arteriovenous malformation at the apex of the right lung with contribution from the right subclavian artery, the intercostal arteries (T7-10), and the right internal mammary artery. Drainage of the arteriovenous malformation was via the pulmonary circulation.
 Digital subtraction angiogram shows an arteriovenous malformation at the apex of the right lung with contribution from the right subclavian artery, the intercostal arteries (T7-10), and the right internal mammary artery. Drainage of the arteriovenous malformation was via the pulmonary circulation.
Digital subtraction angiogram shows an arteriovenous malformation at the apex of the right lung with contribution from the right subclavian artery, the intercostal arteries (T7-10), and the right internal mammary artery. Drainage of the arteriovenous malformation was via the pulmonary circulation.
Because of the high mortality rates associated with missed aortic injuries, most thoracic trauma surgeons have a low threshold for performing aortic angiography and accept a negative examination rate of more than 90%. Findings on chest radiographs are traditionally used to select patients to undergo angiography in the setting of high-speed blunt chest trauma. With chest radiographs as the screening tool, angiography depicts aortic or branch vessel injury in only 10-20% of cases.
Angiographic findings of a ruptured aorta include the presence of a transverse radiolucent line caused by rolled-up edges of a lacerated intima and media. A false aneurysm is depicted as an irregular dilatation, and extravasation of contrast agent may occur at the site of rupture. Occasionally, there is disruption of one or more brachiocephalic vessels. The common sites of aortic injury are just beyond the origin of the left subclavian artery, at the level of the diaphragm, and just above the aortic valve (with patients seldom surviving a rupture in this location).
Chen and colleagues reviewed thoracic aortograms of 166 patients after blunt thoracic trauma. They examined the aortic arch and its branch vessels and detected 24 injuries. In 22 cases, a wide mediastinum was demonstrated on plain radiographs; in the remaining cases, mechanisms of injury were identified that were conducive to aortic injury. Injuries to the aortic arch or to arch branch vessels were found in 24 patients (16 men, 8 women; mean age, 50 yr); in 15 patients (9%), an isolated aortic injury was identified. Injury to the branch vessel occurred in 9 patients (5%). A total of 10 isolated branch vessel injuries were found in 7 of these patients, with 2 more patients having a total of 3 branch vessel injuries associated with aortic injury. [54]
In the Chen et al study, the injured branch vessels comprised the brachiocephalic artery (4 cases), the left common carotid artery (4 cases), the left subclavian artery (3 cases), the right internal mammary artery (1 case), and the left vertebral artery (1 case). Among the branch vessel injuries found were intimal tears (9 vessels, 69%) and transection (resulting in a pseudoaneurysm; 4 vessels, 31%). Seven of the patients had a revised trauma score of 12; an eighth patient had a score of 11; and a ninth had a score of 4. The authors emphasized that angiographic findings may be subtle and that awareness of the incidence of branch injuries, either in isolation or in association with aortic injury, has implications for the evaluation of patients with branch injury using less invasive techniques, including CT and TEE. [54]
Reports have suggested that TEE may be used as the primary imaging modality in patients with a suspected traumatic rupture of the thoracic aorta. However, a segment of the aorta and branches of the aortic arch cannot be adequately evaluated in all patients by means of TEE.
To gauge the impact of TEE's limitations, Ahrar and colleagues looked at the clinical and imaging features of 89 patients who had at one time suffered blunt chest trauma and had displayed angiographic evidence of traumatic damage to the thoracic aorta or to its branches. [55] Seventy-two (81%) of these patients had suffered aortic rupture alone. One (1%) of these ruptures existed at a potential TEE blind spot, the distal ascending aorta. A total of 24 injuries in 17 patients (19%) occurred at the aortic arch branches. The aorta was found to be intact in 14 of these patients; 3 of these patients also had aortic rupture.
In the Ahrar et al study, 70% of aortic arch branch injuries were not suspected on physical examination. The authors concluded that in 20% of patients, traumatic involvement of aortic arch branches or of the distal ascending aorta had occurred. The investigators made a point that these vascular injuries may not be optimally assessed or may be overlooked entirely if TEE is the only imaging modality used to evaluate patients with blunt chest trauma. [55]
Munoz and colleagues described a case of acute traumatic rupture of the thoracic aorta that was diagnosed by means of dynamic CT scanning. [56] Because angiographic confirmation was needed, surgical repair was delayed — a factor that contributed to the patient's death. For cases in which CT scanning shows reliable findings of acute traumatic rupture of the thoracic aorta, Munoz questioned the usefulness of angiographic confirmation.
Spouge and colleagues undertook a retrospective review to determine the incidence of aortic rupture resulting from blunt chest trauma in children and to describe the radiologic findings. [57] They reviewed records and imaging data of 54 consecutive pediatric patients admitted over a 2-year period to a pediatric trauma center after undergoing blunt chest trauma. An aortic tear had been documented in 4 (7.4%) of the 54 patients. Plain radiographs were evaluated for 7 radiographic signs that, according to the literature with regard to adult patients, are sensitive indicators of aortic rupture. These indicators included abnormal aortic contour and mediastinal widening.
The investigators divided the patients into 2 groups. [57] Members of group 1 (n = 4) had aortic rupture, as revealed through angiography or surgery; patients in group 2 (n = 50) had undergone no angiographic investigation. Mediastinal widening and abnormal aortic contour were found in all group 1 patients; however, similar findings were discovered in half of the second group as well. CT scans of the thorax were reviewed for 1 patient from group 1 and for 6 patients from group 2. The aortic tear was well demonstrated in the group 1 patient, but the other scans could not reliably be used to exclude significant aortic injury. The researchers obtained similar results when reviewing plain chest radiographic findings in 5 consecutive children—including 2 additional patients with aortic rupture—who had undergone aortography in the 2 years subsequent to this series.
Traumatic aortic rupture may occur more frequently in the pediatric population than has previously been reported. Plain imaging findings of aortic rupture in children, which are similar to such findings in adult patients, are sensitive but nonspecific. The authors commented that this injury may be underinvestigated, at least in their institution. They stated that, in their opinion, angiography was still the modality of choice for the diagnosis of aortic tears in children. [57]
Sturm and colleagues retrospectively reviewed the records of 314 patients (aged 7-84 yr; mean, 37.7 yr; 255 male, 59 female) who had blunt chest trauma and had undergone thoracic aortography. [58] Most injuries were the result of motor vehicle accidents. The most common indication for aortography was a widened mediastinum on chest radiographs (83.4%). The aortogram was positive for cardiovascular injury in 19.7% of cases. A total of 47 patients had aortic rupture, 15 had subclavian artery disruption, and 1 had traumatic aortic insufficiency.
Complications occurred in 1.7%. Two patients had groin hematomas, and 1 had an intimal tear of the ascending aorta from the angiographic catheter. None of the complications required treatment. An aberrant origin of the arch vessels was found in 0.96% of patients, and ductus diverticulum was found in 0.64%. Two false-positive and no false-negative aortograms were reported. The authors concluded that thoracic aortography after trauma is accurate and safe. [58]
Degree of Confidence
Conventional or digital subtraction angiography remains the criterion standard for depicting traumatic aortic rupture and aortic pseudoaneurysm. Aortography should be performed for any patient suspected of having aortic rupture, because additional trauma results from unnecessary surgical exploration in patients who already have severe trauma. Even in urgent cases, aortography may be performed while other resuscitative measures are undertaken.
Improvements in catheter technology and safer contrast media make the procedure safe.
In his review of 314 patients with blunt chest trauma who underwent thoracic aortography, Sturm found 2 false-positive and 0 false-negative aortograms. He concluded that thoracic aortography after trauma is accurate and safe. [58]
Von Oppell and colleagues describe a case of a ruptured heart in which a false-positive angiographic diagnosis of aortic rupture resulting from ductal diverticulum was made. [59]
Echocardiography
Echocardiography is an excellent means of evaluating acute blunt cardiac injury. Although blunt cardiac injury may result in chamber disruption, valvular incompetence, coronary artery thrombosis, or ventricular aneurysm formation, the most common blunt cardiac injury in treatable patients is myocardial contusion. Its clinically important sequelae are dysrhythmias and cardiac dysfunction. Echocardiography may provide information about cardiac function, motion abnormalities of the cardiac wall, pericardial effusions, and valvular injury.
A traumatic thoracic aortic rupture requires expeditious diagnosis and surgical intervention. About 85% of patients with aortic injury are dead at the scene. If the injury is left untreated, 40% of survivors die within the first 24 hours after injury.
Several groups have evaluated the efficacy of transesophageal echocardiography (TEE) in the diagnosis of traumatic aortic rupture. It appears to be safe, and it is portable and can be brought to the bedside, obviating transport of the patient. TEE may be performed during resuscitative and life-saving procedures. Because of the proximity of the esophagus to the thoracic aorta, TEE allows excellent resolution of structures of the vessel wall. The most important obstacle to the use of ultrasonography in a patient with a thoracic trauma is the presence of massive subcutaneous emphysema, as occurs in cases involving rupture of the tracheobronchial tree.
-
Radiograph of the left shoulder of a 36-year-old man after undergoing a direct blow to the upper thorax shows a fracture of the first rib. The most common injury caused by blunt trauma is a rib fracture, which may be easily missed with suboptimal technique. Overpenetration and a decrease in the kilovolt-peak improve skeletal visualization, although at the expense of lung detail. If available, digital imaging improves visualization, and images may be displayed on a workstation and manipulated. Fractures of the first and second ribs are rare but are often overlooked; they are most often associated with serious vascular and tracheobronchial or spinal injury.
-
Chest radiograph in a child with a shrapnel injury after the shrapnel was removed surgically. Six months later, the child presented with increasing left supraclavicular soft tissue swelling. Left, a chest radiograph shows a soft tissue mass associated with destruction of the first left rib. Right, 2-dimensional and Doppler sonograms show a pseudoaneurysm of the left subclavian artery.
-
Multiple left rib fractures, pulmonary contusion, and hemothorax in an elderly man after a motor vehicle accident.
-
Chest radiograph shows rib fractures and a left-sided hemothorax.
-
Chest radiograph in a man with blunt thoracic trauma shows surgical emphysema and pulmonary hemorrhage, left upper lobe. The patient presented with hemoptysis following injury.
-
Chest radiograph in a man shows a lung contusion (C) after blunt trauma.
-
Transaxial, nonenhanced computed tomography scan shows a pneumothorax in a patient in whom the chest radiograph was normal.
-
Bilateral pneumothoraces in an infant with a deep costophrenic sulcus sign, sharp demarcation of the cardiac border, double-diaphragm contour and depression of left hemidiaphragm, and hyperlucency in lower thorax and upper abdomen.
-
Left-sided tension pneumothorax in an infant.
-
Contrast-enhanced axial computed tomography scan through the thorax of a 20-year-old man after a motorbike accident shows massive, bilateral pulmonary contusions; pneumopericardium; and hemopneumothorax.
-
Contrast-enhanced computed tomography scan through the mediastinum shows a pneumopericardium in a 26-year-old man involved in a motorbike accident.
-
A 32-year-old man with gunshot wounds. Multiple lead pellets are noted in the pleura, adjacent to the thoracic aorta, spleen, and left kidney. Note the hemothorax and splenic laceration.
-
A 32-year-old man with gunshot wounds. Multiple lead pellets are noted in the pleura, adjacent to the thoracic aorta, spleen, and left kidney. Note the hemothorax and splenic laceration.
-
A 32-year-old man with gunshot wounds. Multiple lead pellets are noted in the pleura, adjacent to the thoracic aorta, spleen, and left kidney. Note the hemothorax and splenic laceration.
-
A 32-year-old man with gunshot wounds. Multiple lead pellets are noted in the pleura, adjacent to the thoracic aorta, spleen, and left kidney. Note the hemothorax and splenic laceration.
-
A 32-year-old man with gunshot wounds. Multiple lead pellets are noted in the pleura, adjacent to the thoracic aorta, spleen, and left kidney. Note the hemothorax and splenic laceration.
-
A 32-year-old man with gunshot wounds. Multiple lead pellets are noted in the pleura, adjacent to the thoracic aorta, spleen, and left kidney. Note the hemothorax and splenic laceration.
-
A 32-year-old man with gunshot wounds. Multiple lead pellets are noted in the pleura, adjacent to the thoracic aorta, spleen, and left kidney. Note the hemothorax and splenic laceration.
-
Supine chest radiograph in a man who was stabbed. The knife has been left in the thorax. Note the associated left hemothorax and pulmonary laceration.
-
Chest radiograph in a male patient with a bullet injury (left) shows no thoracic sequelae. No bullet is identified, but a lateral radiograph shows the bullet lodged in the posterior aspect of the lung.
-
Supine chest radiograph shows an endotracheal tube advanced into the right main bronchus. Note the loss of volume in the left lung.
-
Standard chest radiograph shows methotrexate toxicity.
-
Standard chest radiograph shows mediastinal fibrosis after mediastinal radiotherapy for Hodgkin lymphoma.
-
Supine chest radiograph shows a misplaced Ryle tube in the left main bronchus.
-
Chest radiograph in a child shows an inhaled metal screw.
-
Supine chest radiograph shows a misplaced jugular venous pressure line in the azygos vein.
-
Value of inspiratory/expiratory radiographs in the assessment of bronchial obstruction from a foreign body. Right, inspiratory image in an 8-year-old boy shows no abnormality. Left, at full expiration, volume in the right lung has changed little, but the mediastinum has shifted to the left. The findings are those of a ball-valve obstruction of the right main bronchus. A peanut was removed from the right main bronchus during bronchoscopy.
-
Upper gastrointestinal barium series in a patient who had accidentally swallowed his partial dentures. Upper esophagus was obstructed. Note the sharp cutoff (upper arrow) and the dentures (lower arrow). The patient inhaled the barium as a result of esophageal obstruction.
-
Barium inhalation in a man with a neurologic swallowing problem. Note the subsegmental right lower collapse after the inhalation.
-
Tracheal stenosis in a 36-year-old woman after prolonged endotracheal intubation.
-
Left, supine chest radiograph shows a pneumothorax after attempted placement of a right subclavian line. Right, sonogram shows echogenic fluid within the right costophrenic angle; this is suggestive of a hemothorax.
-
Radiograph of a male subject's thorax shows a diaphragmatic rupture after a motor vehicle accident. Rupture and laceration of the diaphragm occurs more frequently on the left because of the protection of liver on the right. However, in cases of delayed diagnosis, the right side is initially missed more often. The chest radiographic findings may not be diagnostic. Computed tomography scans or gastrointestinal contrast-enhanced studies may be indicated.
-
Barium enema study in a patient with a delayed diagnosis of a right diaphragmatic rupture after a steering column injury. Note the hepatic flexure of the colon extending into the thorax.
-
Coronal reconstruction of contrast-enhanced computed tomography scan shows the omentum occupying the left hemithorax because of a diaphragmatic rupture.
-
Digital subtraction angiogram shows a pseudoaneurysm of the thoracic aorta in a man after a steering column injury. The site of these pseudoaneurysms is remarkably constant: at or near the aortic attachment of the ligamentum arteriosum; they occur less often just above the heart, at the aortic origin.
-
Chest radiograph in a 57-year-old man with a history of blunt thoracic trauma 6 years before shows a well-defined opacity overlying the aortic knuckle.
-
Nonenhanced computed tomography scan through the upper thoracic aorta shows an aneurysmal dilatation of the aortic knuckle suggestive of a pseudoaneurysm (which was confirmed at surgery). The patient was allergic to radioiodinated contrast material.
-
Digital subtraction angiogram shows an arteriovenous malformation at the apex of the right lung with contribution from the right subclavian artery, the intercostal arteries (T7-10), and the right internal mammary artery. Drainage of the arteriovenous malformation was via the pulmonary circulation.
-
Digital subtraction angiogram shows an arteriovenous malformation at the apex of the right lung with contribution from the right subclavian artery, the intercostal arteries (T7-10), and the right internal mammary artery. Drainage of the arteriovenous malformation was via the pulmonary circulation.
-
Digital subtraction angiogram shows an arteriovenous malformation at the apex of the right lung with contribution from the right subclavian artery, the intercostal arteries (T7-10), and the right internal mammary artery. Drainage of the arteriovenous malformation was via the pulmonary circulation.
-
Contrast-enhanced axial computed tomography scan through the mid-thorax in a 36-year-old man with a history of blunt thoracic trauma shows thickening of the right anterior serratus muscle associated with an arteriovenous extrathoracic-intrathoracic communication.
-
Axial, contrast-enhanced computed tomography scan (lung window) shows communication with the right lower pulmonary vein.
-
Lateral radiograph of the dorsal spine shows a wedge fracture of the tenth dorsal vertebral body after a steering column injury.
-
Rules of 2s.
-
Rules of 2s: (1) The distance between adjacent spinous processes should be no more than 2 mm. (2) The interpedicular distances of contiguous vertebral bodies should not vary more than 2 mm. (3) The width of facet joints should be no more than 2 mm at all levels. (4) The posterior and anterior heights of vertebral bodies should be no more than 2 mm, except at D11 and D12.
-
Rules of 2s: (1) The distance between adjacent spinous processes should be no more than 2 mm. (2) The interpedicular distances of contiguous vertebral bodies should not vary more than 2 mm. (3) The width of facet joints should be no more than 2 mm at all levels. (4) The posterior and anterior heights of vertebral bodies should be no more than 2 mm, except at D11 and D12.
-
Axial, nonenhanced computed tomography scan with sagittal reconstruction shows a vertebral fracture in a man after a motor vehicle accident.
-
Coronal computed tomography scan of the thorax seen on a soft tissue window, showing a stab-wound defect in the left anterior chest wall. Note the left upper lobe contusion/laceration and a large pneumothorax.
-
Coronal computed tomography scan of the thorax seen on a soft-tissue window, showing a stab-wound defect in the left anterior chest wall. Note the left upper lobe contusion/laceration and a large pneumothorax.
-
Coronal computed tomography scan of the thorax seen on a mediastinal window, showing a large left hemothorax and pneumomediastinum following a stab wound.
-
Axial computed tomography scan of the thorax seen on a mediastinal window, showing a large left hemothorax and pneumomediastinum following a stab wound.
-
Three-dimensional reconstruction of the heart showing pericardial injury along the left heart border just below the pulmonary conus.
-
Rib fracture. Courtesy of Ravi Devidas Kadasne, MBBS, MD, Specialist in Radiology, Emirates International Hospital, UAE.
-
Rib fracture. Courtesy of Ravi Devidas Kadasne, MBBS, MD, Specialist in Radiology, Emirates International Hospital, UAE.
-
Rib fracture. Courtesy of Ravi Devidas Kadasne, MBBS, MD, Specialist in Radiology, Emirates International Hospital, UAE.
-
Rib fracture. Courtesy of Ravi Devidas Kadasne, MBBS, MD, Specialist in Radiology, Emirates International Hospital, UAE.
-
Scapula fracture; diagnosis was doubtful on radiographs but confirmed by ultrasound. Courtesy of Ravi Devidas Kadasne, MBBS, MD, Specialist in Radiology, Emirates International Hospital, UAE.
-
Scapula fracture; diagnosis was doubtful on radiographs but confirmed by ultrasound. Courtesy of Ravi Devidas Kadasne, MBBS, MD, Specialist in Radiology, Emirates International Hospital, UAE.







