Practice Essentials
Thoracic trauma may present as an isolated rib fracture, a chest contusion, or a laceration; however, significant thoracic trauma often involves multiple organ systems and several anatomic regions. [1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11] The chest trauma that results from a motor vehicle accident may result in injury to the sternum, the ribs, and the heart, aorta, and lungs. Multiple injuries often occur in people who are involved in traffic accidents, and rib fractures are among the most common of these injuries, with an occurrence as high as 60%. Radiography of the chest should be a routine part of autopsies of patients who die of injuries that result from traffic accidents. [12]
Radiographs can depict bony trauma, and rib fractures are among the most commonly identified injuries to the chest. Injuries to the chest wall may involve the pleural space, lungs, extrapleural space, mediastinum, heart and great vessels, spine, and shoulders. [13]
The American College of Radiology has published the following guidelines regarding rib fracture imaging [14] :
-
A radiograph of the chest is usually appropriate for the initial imaging of suspected rib fractures from minor blunt trauma (injury confined to ribs).
-
A radiograph of the chest is usually appropriate for the initial imaging of suspected rib fractures after cardiopulmonary resuscitation.
-
A radiograph of the chest is usually appropriate for suspected pathologic rib fracture, with CT chest without IV contrast or technetirum-99m (Tc-99m) bone scan whole body as complementary to the chest radiography.
Chest CT is considered the gold standard of detecting rib fractures, but the fractures may not be clinically significant. Chest CT is more important in general assessment of trauma for other injuries. Whole-body CT has become standard practice in the management of severely injured trauma patients, but it is necessary to improve rib fracture diagnosis accuracy on CT. Significant progress has been made in clinical applications based on deep learning techniques for medical image interpretation, such as algorithms based on deep convolutional neural networks (DCCN) for CT. [1, 15, 16, 17, 18, 19, 20, 21, 22]
The location of specific rib fractures is an important indicator of related injury. Rib fractures can be studied as 3 distinct patterns according to their location (see the images below): (1) fractures of the first rib and those of the second to fourth ribs, (2) fractures of the fifth to ninth ribs, and (3) fractures of the 10th to 12th ribs. These 3 distinct patterns of rib fractures represent unique pathophysiology and associated morbidity. A rib score may be used to predict adverse pulmonary outcomes. [11]
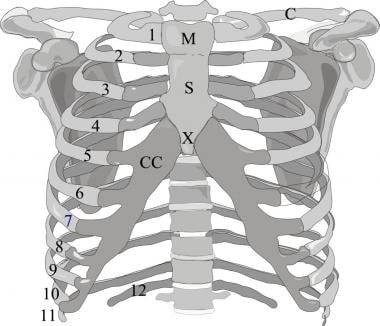 Frontal image of the rib cage. Ribs 1-12 demonstrate the variable shape of the upper 9 ribs. The 12th rib does not articulate anteriorly. The sternum consists of the manubrium (M), the body (S), and the xiphoid (X). The ribs articulate with the sternum via the costochondral (CC) junction. C = clavicle.
Frontal image of the rib cage. Ribs 1-12 demonstrate the variable shape of the upper 9 ribs. The 12th rib does not articulate anteriorly. The sternum consists of the manubrium (M), the body (S), and the xiphoid (X). The ribs articulate with the sternum via the costochondral (CC) junction. C = clavicle.
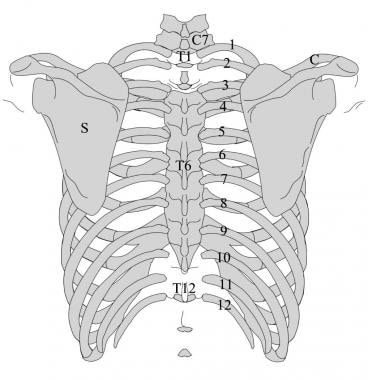 Posterior image of the thorax. The ribs are numbered 1-12. The clavicle (C) and scapula (S) are often involved in injuries that include rib fractures.
Posterior image of the thorax. The ribs are numbered 1-12. The clavicle (C) and scapula (S) are often involved in injuries that include rib fractures.
Pathophysiology
Fractures of the first rib
Fractures of the first rib are rare. The significance of a first rib fracture is the association with cervical spine trauma, multiple rib fractures, or life-threatening vascular injuries. Historically, fractures of ribs 1-3 have been associated with injuries of the brachial plexus and major vessels. CT angiography (CTA) should be considered in stable patients with first rib fractures if there are absent or decreased upper extremity pulses, regional hemorrhage, and/or brachial plexus injury. Additional criteria for angiography include displacement of bone fragments and multiple thoracic injuries.
Fractures of the first rib imply a violent force; this pattern of fractures may signify injury to the adjacent subclavian vein and brachial plexus. Isolated first rib fractures are seen in association with cranial and maxillofacial injuries and are probably secondary to avulsion of the first rib by its muscular attachment rather than direct trauma to the rib, which is relatively protected. Surfer's rib is an isolated first-rib fracture and occurs in surfers who perform the lay-back maneuver.
Fractures of the fifth to ninth ribs
Fractures of the fifth to ninth ribs can be single or multiple. Multiple fractures can present as flail chest, which is present when paradoxical respiratory movement occurs in a segment of the chest wall. This type of fracture requires at least 2 segmental fractures in each of 3 adjacent ribs, the costal cartilages, or the sternum (see the image below). Posterior flail segments are easier to manage clinically because of the presence of strong muscular and scapular support and because of a patient's natural tendency to lie with his or her back against the mattress.
(See the images below.)
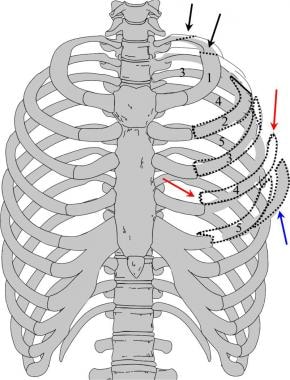 Image depicting multiple fractures of the left upper chest wall. The first rib is often fractured posteriorly (black arrows). If multiple rib fractures occur along the midlateral (red arrows) or anterior chest wall (blue arrows), a flail chest (dotted black lines) may result.
Image depicting multiple fractures of the left upper chest wall. The first rib is often fractured posteriorly (black arrows). If multiple rib fractures occur along the midlateral (red arrows) or anterior chest wall (blue arrows), a flail chest (dotted black lines) may result.
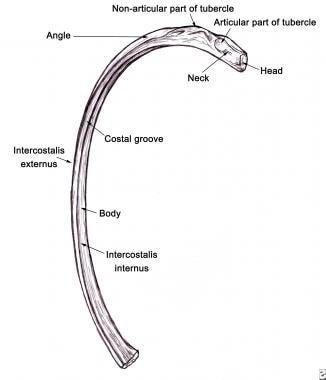 Image of the common middle rib. The common middle rib consists of the neck that is closest to the thoracic spine with an articular tubercle, the angle of which is a curved portion of the rib, and the distal body.
Image of the common middle rib. The common middle rib consists of the neck that is closest to the thoracic spine with an articular tubercle, the angle of which is a curved portion of the rib, and the distal body.
An inward displacement of the rib fracture fragments at the time of the injury may lacerate the lung parenchyma and produce a pneumothorax, with a possible hemothorax. Although lung trauma is generally seen immediately, the occurrence of a pneumothorax and hemothorax may be delayed for hours after the injury. Hemothorax of a significant degree secondary to rib fractures is usually the result of laceration of an intercostal artery rather than bleeding from the lung. The hemothorax resulting from a laceration of an intercostal artery can be life threatening.
A spontaneous fracture of a midthoracic rib should alert the clinician for an underlying metastasis, multiple myeloma, or hyperparathyroidism.
Fractures of the tenth to the twelfth ribs
Hemorrhage around and within the adrenal glands represents a risk that is associated with fractures of the lower ribs. Fractures of the lower ribs are also commonly associated with visceral injury to the kidneys and the spleen. Associated lumbar and thoracic vertebral spinal injuries occur because of the proximity of the transverse spinous processes to the lower thoracic and upper lumbar spine. [2, 23, 3]
Pneumothorax
A pneumothorax is a common sequela of blunt trauma. Fracture fragments that lacerate the lung parenchyma can cause bleeding into the pleural cavity and result in a pneumothorax (see the image below).
 Semi-erect anteroposterior (AP) chest radiograph in a patient with a nondisplaced posterior fracture of the left 10th rib. A small, apical pneumothorax (black arrow) is present on the left, and there is volume loss in the left lower lobe (white arrow).
Semi-erect anteroposterior (AP) chest radiograph in a patient with a nondisplaced posterior fracture of the left 10th rib. A small, apical pneumothorax (black arrow) is present on the left, and there is volume loss in the left lower lobe (white arrow).
The incidence of a pneumothorax is not as high with one rib fracture, but the risk increases as the number of broken ribs increases (see the images below).
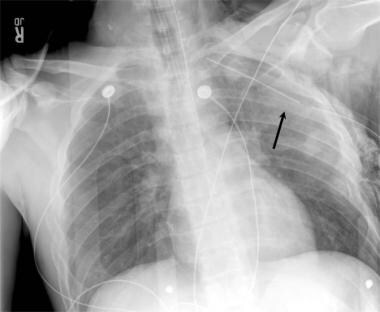
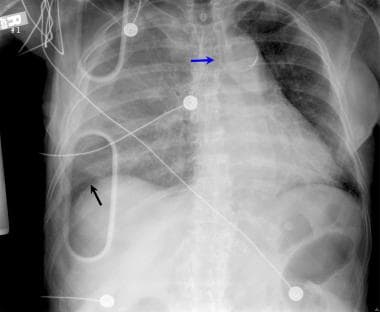 Supine anteroposterior (AP) chest radiograph shows the presence of a right tension pneumothorax, which has displaced the trachea to the right (blue arrow). A displaced right lower rib fracture is present in the right posterolateral aspect of the chest (black arrow).
Supine anteroposterior (AP) chest radiograph shows the presence of a right tension pneumothorax, which has displaced the trachea to the right (blue arrow). A displaced right lower rib fracture is present in the right posterolateral aspect of the chest (black arrow).
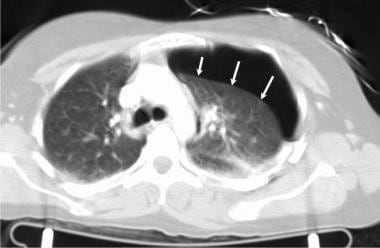 Axial computed tomography image of the chest in a patient with multiple left posterior rib fractures. A large left pneumothorax is present (arrows).
Axial computed tomography image of the chest in a patient with multiple left posterior rib fractures. A large left pneumothorax is present (arrows).
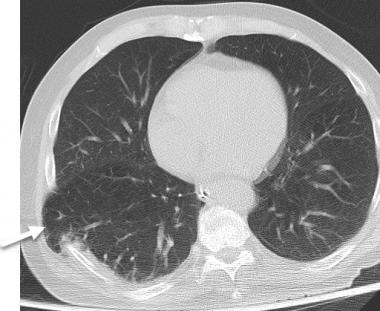
 Axial computed tomography image of the chest in a patient with left posterior rib fractures. The left pneumothorax (white arrows) is associated with a displaced posterior left rib fracture (black arrow). Secondary effects on the left lung include a pulmonary contusion and volume loss.
Axial computed tomography image of the chest in a patient with left posterior rib fractures. The left pneumothorax (white arrows) is associated with a displaced posterior left rib fracture (black arrow). Secondary effects on the left lung include a pulmonary contusion and volume loss.
In a retrospective study, Miller and Ghanekar found that significant solid organ injury was 3.5 times more common in patients who suffered blunt trauma and had a pneumothorax than in patients without a pneumothorax. In addition, the authors found that the association of rib fractures with a pneumothorax resulted in a larger number of visceral lacerations by fragments of bone. They recommended that because a large proportion of pneumothoraces found with CT scanning are not visualized on a portable chest radiograph, clinicians should look for indirect signs of pneumothorax, such as the presence of rib fractures and subcutaneous air. [23]
Hemothorax
The incidence of hemopneumothoraces in patients with rib fractures is 30%. A hemothorax is usually the result of a lacerated intercostal artery; however, bleeding from broken ribs usually stops before a sufficient volume is lost and before emergency thoracotomy is required. Note, however, that about 400-500 mL of blood may be hidden by the diaphragm on an upright chest radiograph, and 1 L or more of blood may be overlooked on a supine image.
The bleeding may be delayed or may recur after several days. In a review by Simon et al, 12 cases of delayed hemothorax were identified, and 92% of those occurred in patients with multiple or displaced rib fractures. [24] The presentation of hemothorax in these cases occurred between 18 hours and 6 days after the injury. Eleven of the affected patients complained of new-onset pleuritic chest pain and dyspnea; the symptoms were similar to those of a pulmonary embolism.
Pulmonary contusion
Rib fractures are associated with pulmonary contusions in 20-40% of cases. The injury is characterized by capillary disruption that results in the presence of intra-alveolar and interstitial hemorrhage, edema, protein, and fluid obstruction of the small airways with leukocyte infiltration. Serial chest radiographs obtained beginning right after the injury show a fluffy infiltrate that progresses in extent and opacity over 24-48 hours.
Pulmonary contusions are often a part of a major chest injury that includes one or more fractures of the thoracic cage, a pneumothorax, and a hemothorax. The contusions may occur by the transmission of force through the chest wall with minimal fractures of the ribs or sternum; this mechanism is especially seen in the young in whom there is greater flexibility of the rib articulations allowing for more lung compression in the absence of a fracture. In middle-aged or elderly patients, pulmonary contusions are usually accompanied by multiple rib fractures. A rib score may be used to predict adverse pulmonary outcomes. [11]
Aortic injuries
The idea that thoracic cage injuries are predictive of acute traumatic aortic tears is controversial. A study by Lee et al concluded that no clinically relevant correlation exists between these injuries and acute traumatic aortic tears. [25] The authors also concluded that isolated upper rib fractures are not an indication for aortic angiography; however, first rib and second rib fractures may indicate a severity of trauma associated with facial, spinal, and brachial injuries.
An aortic injury that is related to blunt trauma is usually due to the transmission of a shearing force at the ligamentum arteriosum or due to the forceful compression of the aortic root. However, there have been case reports that describe fractured ribs puncturing the aorta. One such case involved a posterior fracture of the left sixth rib that lacerated the aorta 3 days after the trauma occurred. [4, 5]
Flail chest
A flail chest is present when a paradoxical respiratory movement occurs in a segment of the chest wall, the result of at least 2 segmental fractures in each of 3 adjacent ribs or costal cartilages (see the images below). The incidence of flail segments is 10-15% in patients with major chest trauma. More severe injuries, such as closed head injury and intrathoracic injury, are common in the presence of a flail chest.
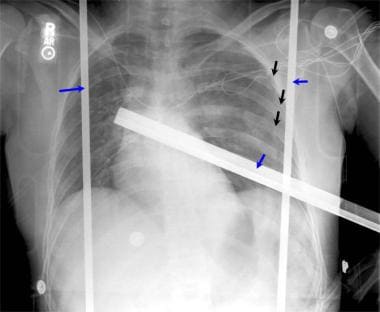 Anteroposterior (AP) supine chest radiograph that was obtained upon a patient's arrival in the emergency department after a serious automobile accident. Although rib fractures are identified along the left lateral chest wall (black arrows), the transportation bed created superimposed metal artifacts (blue arrows) that obscure visualization of possible other rib fractures along the chest wall.
Anteroposterior (AP) supine chest radiograph that was obtained upon a patient's arrival in the emergency department after a serious automobile accident. Although rib fractures are identified along the left lateral chest wall (black arrows), the transportation bed created superimposed metal artifacts (blue arrows) that obscure visualization of possible other rib fractures along the chest wall.
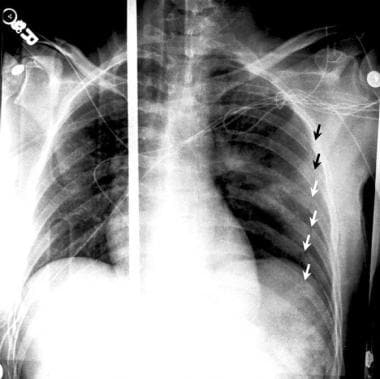 Supine anteroposterior (AP) chest radiograph that was obtained after the removal of metal artifacts along the left chest wall. Multiple posterolateral rib fractures are noted on the left (arrows; Note: White and black arrows were used for easy visualization due to the dark and light areas of the lungs).
Supine anteroposterior (AP) chest radiograph that was obtained after the removal of metal artifacts along the left chest wall. Multiple posterolateral rib fractures are noted on the left (arrows; Note: White and black arrows were used for easy visualization due to the dark and light areas of the lungs).
Multiple fractures of the upper chest with a dislocation of the clavicle are also associated with extrathoracic lung herniation. [6] However, in most cases, no chest wall defects are present. Flail chest may lead to respiratory failure secondary to the pulmonary contusion and pain during inspiration.
Clinical details
First rib fractures have often been described as having a high association with serious or lethal spinal or vascular injuries. While first rib fractures have a high association with spinal fractures and are associated with multisystem injuries, the occurrence of first rib fractures is not always associated with increased morbidity and mortality. The presence of a first rib injury requires a multidisciplinary approach. CT of the spine and chest allows for an early diagnosis. Appropriate treatment and observation in the intensive care unit may prevent further morbidity and/or mortality. [26]
The number of rib fractures correlates with mortality in adult trauma patients, rising sharply in patients with more than 6 fractured ribs. In a study of pediatric patients (< 21 yr) with rib fractures, using information from the National Trauma Data Bank, mortality increased from 1.79% in pediatric patients with zero rib fractures to 5.81% for patients with 1 rib fracture, up to 8.23% for patients with 7 rib fractures. [27]
The association of lower rib fractures with pelvic fractures has been associated with a higher incidence of solid organ injury. [7]
Imaging modalities
The patient's medical history and physical examination findings should suggest the diagnosis of a rib fracture. The primary signs and symptoms are a pleuritic-type chest pain and tenderness over fracture site. When 2 or more adjacent ribs are fractured, especially if they are broken in more than one place, examination alone should be enough to enable a presumptive diagnosis of a rib fracture.
The standard chest radiograph is useful in the recognition of preexistent or coexistent disease. The routine radiographic examination of the sternum includes the frontal prone and rotated views in an off-lateral projection. However, approximately 50% of all rib fractures go undetected during screening chest radiography (see the first 2 images below). [28, 29] The examination of suspected rib fractures should include the acquisition of erect posteroanterior (PA) and oblique radiographs of the chest (see the third image below). An erect frontal examination of the chest is useful in the detection of a pneumothorax, pulmonary contusion, or pleural effusion. [30]
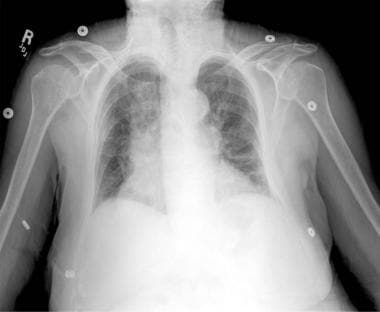 Anteroposterior (AP) chest radiograph in a patient who presented with severe left chest wall pain after a minor fall. No rib injury is apparent.
Anteroposterior (AP) chest radiograph in a patient who presented with severe left chest wall pain after a minor fall. No rib injury is apparent.
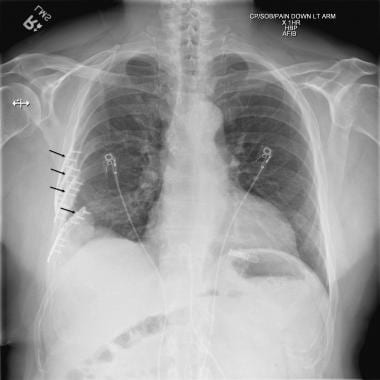
 Anteroposterior (AP) radiograph of an elderly female patient with severe left chest wall pain after a minor fall. This image demonstrates a left lateral rib fracture (arrow) that is not seen on the standard AP chest radiograph.
Anteroposterior (AP) radiograph of an elderly female patient with severe left chest wall pain after a minor fall. This image demonstrates a left lateral rib fracture (arrow) that is not seen on the standard AP chest radiograph.
 This detailed oblique radiograph shows 2 rib fractures (arrows) that are not depicted on anteroposterior (AP) chest radiographs.
This detailed oblique radiograph shows 2 rib fractures (arrows) that are not depicted on anteroposterior (AP) chest radiographs.
Each oblique projection is intended to depict the entire rib. The PA chest radiograph alone is ineffective in the identification of incomplete or minimally displaced rib fractures; the lower ribs may be obscured by the upper abdominal organs. If a lower rib fracture is suspected, a radiographic technique is required that centers an AP radiograph of the lower portion of the chest and upper abdomen on the upper lumbar spine film.
If the patient remains symptomatic despite a negative initial radiograph, a repeat radiograph of the ribs, acquired with a standard technique, often demonstrates the signs of early healing of a rib fracture. If the identification of occult rib fractures is clinically important, as in a case of suspected child abuse or for medicolegal reasons, radionuclear bone scanning with technetium-99m methylene diphosphonate (99mTc MDP) is often successful. A delay of several days should be allowed after an acute trauma to increase the sensitivity of radionuclear imaging for a rib fracture.
Rib fractures may be seen by using bone window settings on a chest CT scan; however, an occult rib fracture is not an indication for thoracic CT scanning. [31, 32, 33, 34, 35]
Chest CT is considered the gold standard of detecting rib fractures, but the fractures may not be clinically significant. Chest CT is more important in general assessment of trauma for other injuries. Significant progress has been made in clinical applications based on deep learning techniques for medical image interpretation, such as algorithms based on deep convolutional neural networks (DCCN) for CT.
Limitations of techniques
In obese patients and in older patients with osteoporosis, the evaluation for uncomplicated rib fractures is often difficult to perform with standard radiographs.
Greenstick fractures may not be seen on initial chest radiographs because of the nondistracted nature of the injury.
Cartilage fractures and costochondral separations are not seen on routine chest radiographs; several weeks may pass before such injuries are visible on chest radiographs. However, the fractures may be indirectly seen following the development of periosteal reaction around the fractures.
Radiologic intervention
Radiologic intervention in cases of rib trauma generally represents emergency treatment of the complications of chest wall injuries (pneumothoraces) or the control of hemorrhage. Angiography may be used as a diagnostic technique in cases in which findings in the aortic arch and anterior mediastinum remain in doubt.
Treatment
Bansidhar et al found that 93% of patients with clinical rib fractures are able to resume their daily activities without disability. [29] As a result, the authors did not recommend routine chest radiographic follow-up in addition to physical examination except in the presence of clinical deterioration.
Adequate pain control, rapid mobilization, and meticulous respiratory care can prevent respiratory complications in patients with rib fractures. An adequate oral analgesic or an intercostal nerve block plus an oral analgesic should provide reasonable pain relief.
In a study in which morphine patient-controlled analgesia (PCA) was compared with thoracic epidural analgesia involving bupivacaine and fentanyl, the latter provided more adequate pain control. [36] In another study regarding the effectiveness of intrapleural analgesia for blunt trauma of the chest wall, this treatment did not significantly differ from placebo. [37] Furthermore, the investigators did not recommend intrapleural analgesia for pain management in patients with rib fractures.
Rapid mobilization can include oscillation therapy or body positioning in patients who are on bed rest or are intubated. This mobilization can involve the patient's ambulating, sitting up in bed, or getting out of bed to move into a chair. Respiratory care entails incentive spirometry, pulmonary toilet, and even mechanical ventilation, when indicated. In splinting the rib fractures, adhesive strapping or chest binders should be avoided in all patients except the very young.
(See the images below.)
 If the management of multiple rib fractures is complicated by reducing lung function, the chest wall can be stabilized by the use of plates held in position by multiple screws (black arrows).
If the management of multiple rib fractures is complicated by reducing lung function, the chest wall can be stabilized by the use of plates held in position by multiple screws (black arrows).
 The treatment of multiple rib fractures includes the option of alignment and fixation of the fractures if respiration is compromised. After alignment, a plate was applied to each of four displaced rib fractures, held in position by multiple screws (white arrows).
The treatment of multiple rib fractures includes the option of alignment and fixation of the fractures if respiration is compromised. After alignment, a plate was applied to each of four displaced rib fractures, held in position by multiple screws (white arrows).
Radiography
The most common radiographic presentation of rib fractures is that of a minimally displaced, irregular lucent line across the cortex of the involved rib. Secondary findings of rib fractures include a localized extrapleural hematoma, which is seen as a focal pleural opacity. Most rib fractures are better seen on a tangent. The formal rib radiographic series that includes posterior and anterior oblique projections using bone exposure and bone filter represents the most sensitive radiographic test. The sensitivity of an ordinary portable chest radiograph for the detection of a nondisplaced rib fracture may result in a missed diagnosis (see the images below). [30]
Anteroposterior (AP) chest radiograph in a patient who presented with severe left chest wall pain after a minor fall. No rib injury is apparent.
Anteroposterior (AP) radiograph of an elderly female patient with severe left chest wall pain after a minor fall. This image demonstrates a left lateral rib fracture (arrow) that is not seen on the standard AP chest radiograph.
This detailed oblique radiograph shows 2 rib fractures (arrows) that are not depicted on anteroposterior (AP) chest radiographs.
A small focal pneumothorax or the presence of subcutaneous air (see the first 2 images below) may be the only initial radiographic sign of a rib fracture. A large pneumothorax may result in the shift of the trachea or other mediastinal structures away from the injury (see the third image below).
 This anteroposterior (AP) chest radiograph demonstrates a left lateral lower rib fracture (white arrow). In addition, there is an associated left subcutaneous gas pattern that dissects along the left chest wall (black arrow).
Semi-erect anteroposterior (AP) chest radiograph in a patient with a nondisplaced posterior fracture of the left 10th rib. A small, apical pneumothorax (black arrow) is present on the left, and there is volume loss in the left lower lobe (white arrow).
Supine anteroposterior (AP) chest radiograph shows the presence of a right tension pneumothorax, which has displaced the trachea to the right (blue arrow). A displaced right lower rib fracture is present in the right posterolateral aspect of the chest (black arrow).
This anteroposterior (AP) chest radiograph demonstrates a left lateral lower rib fracture (white arrow). In addition, there is an associated left subcutaneous gas pattern that dissects along the left chest wall (black arrow).
Semi-erect anteroposterior (AP) chest radiograph in a patient with a nondisplaced posterior fracture of the left 10th rib. A small, apical pneumothorax (black arrow) is present on the left, and there is volume loss in the left lower lobe (white arrow).
Supine anteroposterior (AP) chest radiograph shows the presence of a right tension pneumothorax, which has displaced the trachea to the right (blue arrow). A displaced right lower rib fracture is present in the right posterolateral aspect of the chest (black arrow).
A fracture of the manubrium may be accompanied by presternal hematoma. Injury to the sternum is best evaluated with lateral and oblique views that are centered on the sternum.
After calcification, fractures of the costal cartilages may be detected by radiographs obtained in an anterior oblique projection.
Widening of the mediastinum suggests the possibility of both an aortic injury and associated rib or sternal fractures. In cases of suspected mediastinal bleeding, a lateral radiograph of the sternum can help to confirm a serious chest injury.
Blunt trauma to the chest may result in incomplete or nondisplaced rib fractures. Such injuries may not be visible on the initial chest radiographs. AP supine chest radiographs often fail to demonstrate rib detail. Approximately 10-15% of rib fractures are not visible on the standard chest image.
AP supine chest radiographs often fail to demonstrate rib detail. False-positive readings for rib fractures are associated with superimposed bowel gas over the lower ribs, resulting in the appearance of a lucent line that is not the result of a rib fracture. The costal-cartilage junction is often misinterpreted as a fracture. Artifacts due to clothing, skin folds, and intravenous (IV) lines can also lead to false suggestions of rib fractures.
Sano studied 217 rib fractures in 75 patients who underwent both chest CT and rib radiography. Rib radiography missed 43 fractures in 24 patients, with causes being overlap with organs in 15 cases, trivial fractures in 21 cases, and injury outside the imaging range in 7 cases. CT missed 21 rib fractures in 17 patients, with causes being horizontal fractures in 10 cases, trivial fractures in 9 cases, and insufficient breath holding in 1 case. [38]
Computed Tomography
Each thoracic CT examination that is performed for the evaluation of trauma offers an opportunity to diagnose rib fractures (see the images below). A direct sign of a rib fracture on an axial CT scan of the chest is the separation of 2 rib fragments with the associated sharp edges. The secondary findings related to rib fractures include a hemothorax, pneumothorax, and lung contusion. These findings are more easily seen on chest CT scans than on chest radiographs. [33, 34, 35]
(See the images below.)
Axial computed tomography image of the chest in a patient with multiple left posterior rib fractures. A large left pneumothorax is present (arrows).
Axial computed tomography image of the chest in a patient with left posterior rib fractures. The left pneumothorax (white arrows) is associated with a displaced posterior left rib fracture (black arrow). Secondary effects on the left lung include a pulmonary contusion and volume loss.
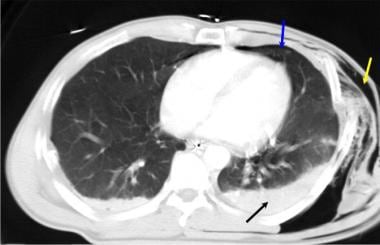 Axial computed tomography image of the chest in a patient with trauma to the left chest wall, where air (yellow arrow) is noted. A small left pneumothorax (blue arrow) is present, and the posterior left lung and the pleural space are opacified due to the combination of a left hemothorax and a left pulmonary contusion.
Axial computed tomography image of the chest in a patient with trauma to the left chest wall, where air (yellow arrow) is noted. A small left pneumothorax (blue arrow) is present, and the posterior left lung and the pleural space are opacified due to the combination of a left hemothorax and a left pulmonary contusion.
 Supine anteroposterior (AP) chest radiograph. This image demonstrates increased opacity of the left lateral upper lobe (arrow), a finding that is consistent with a pulmonary contusion after left chest wall trauma and rib fractures.
Supine anteroposterior (AP) chest radiograph. This image demonstrates increased opacity of the left lateral upper lobe (arrow), a finding that is consistent with a pulmonary contusion after left chest wall trauma and rib fractures.
All chest CT scans should be reviewed with a bone window setting, one that emphasizes the internal lung detail. The application of a bone CT scan algorithm increases the likelihood of finding fractures. Every effort should be made to decrease patient movement and breathing-related artifacts. The areas contiguous with pulmonary contusions and localized bleeding should be carefully examined for rib fractures as well.
With improvements in the resolution of CT scanners, the thoracic spine can be examined for fractures by using chest CT images (see the images below). Gas in the epidural space can arise via a thoracic spinal fracture that is associated with a pneumothorax. Associated injuries to the internal organs of the upper abdomen should be considered in all cases of lower rib fractures; posterior lower rib fractures are often complicated by splenic injury. Fractures of the posterior upper thorax may be complicated by associated scapular fractures.
(See the images below.)
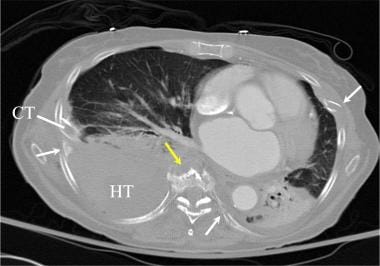 Axial computed tomography image of the chest in a patient with a complex, unstable, thoracic spinal fracture. Multiple rib fractures (white arrows) are shown. In addition, the midthoracic spine is fractured (yellow arrow), and a large right hemothorax (HT) is present. CT = chest tube.
Axial computed tomography image of the chest in a patient with a complex, unstable, thoracic spinal fracture. Multiple rib fractures (white arrows) are shown. In addition, the midthoracic spine is fractured (yellow arrow), and a large right hemothorax (HT) is present. CT = chest tube.
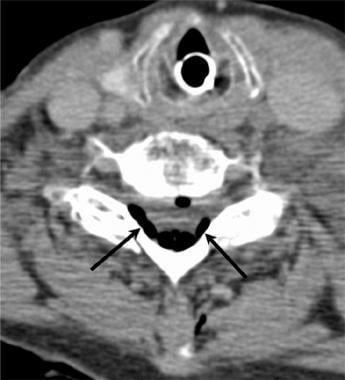 Axial computed tomography image of the lower cervical spine in a patient with multiple rib fractures and an unstable fracture of the thoracic spine. Air has dissected into the epidural space posterior to the cervical dura (arrows).
Axial computed tomography image of the lower cervical spine in a patient with multiple rib fractures and an unstable fracture of the thoracic spine. Air has dissected into the epidural space posterior to the cervical dura (arrows).
 Sagittal reformatted computed tomography image of the cervical spine in a patient with multiple rib fractures and an unstable thoracic spinal injury. Epidural gas is noted dorsally in the spinal canal (arrows).
Sagittal reformatted computed tomography image of the cervical spine in a patient with multiple rib fractures and an unstable thoracic spinal injury. Epidural gas is noted dorsally in the spinal canal (arrows).
 Abdominal radiograph. This image demonstrates moderate gaseous distention. The distended stomach was associated with a hemoperitoneum.
Abdominal radiograph. This image demonstrates moderate gaseous distention. The distended stomach was associated with a hemoperitoneum.
 Axial computed tomography image of the chest in a patient with both anterior and posterior thoracic injuries. A fracture of the sternum (white arrow) and a posterior left rib fracture (yellow arrow) are present.
Axial computed tomography image of the chest in a patient with both anterior and posterior thoracic injuries. A fracture of the sternum (white arrow) and a posterior left rib fracture (yellow arrow) are present.
 Axial computed tomography image of the lower thorax in a patient with multiple trauma. A left lower posterior rib fracture has resulted in a splenic contusion (arrow).
Axial computed tomography image of the lower thorax in a patient with multiple trauma. A left lower posterior rib fracture has resulted in a splenic contusion (arrow).
 Axial computed tomography image in a patient with a severe thoracic injury. Rib fractures and a complex left scapular fracture (arrows) are present.
Axial computed tomography image in a patient with a severe thoracic injury. Rib fractures and a complex left scapular fracture (arrows) are present.
In severe motor vehicle accidents, both anterior and posterior rib fractures may be seen in the same patient (see the images below). Multiple systemic trauma may lead to prolonged hypotension or hypoxia. Multiple cerebral infarcts may result from cerebral hypoxia or as a complication of direct cranial trauma (see the second image below).
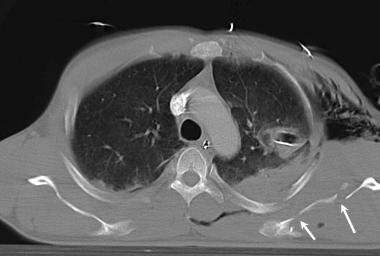
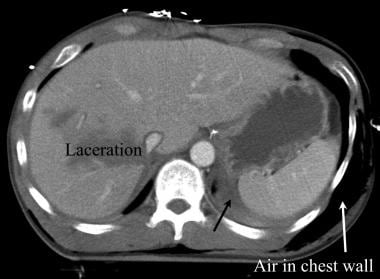 Axial computed tomography image of the chest in a patient with multiple anterior and posterior rib fractures. A liver laceration is present. Air is noted in the subcutaneous space surrounding the left ribs (white arrows), blood is in the perisplenic space (black arrow), and a subcutaneous emphysema is present along the left chest wall. The patient was also treated for a large left pneumothorax.
Axial computed tomography image of the chest in a patient with multiple anterior and posterior rib fractures. A liver laceration is present. Air is noted in the subcutaneous space surrounding the left ribs (white arrows), blood is in the perisplenic space (black arrow), and a subcutaneous emphysema is present along the left chest wall. The patient was also treated for a large left pneumothorax.
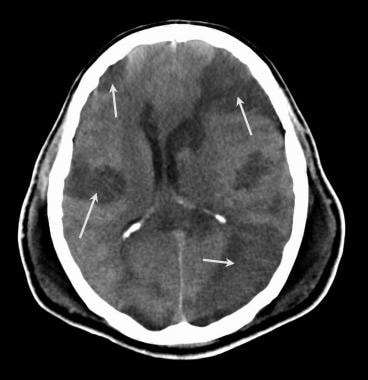 Axial computed tomography image of the brain in a patient with multiple rib fractures and a tension pneumothorax. Multiple bilateral cerebral infarcts are present (arrows). The direct injury to the brain was less complicated by hypoxia.
Axial computed tomography image of the brain in a patient with multiple rib fractures and a tension pneumothorax. Multiple bilateral cerebral infarcts are present (arrows). The direct injury to the brain was less complicated by hypoxia.
Sternal fractures require special care. A clinically important fracture of the sternum may be seen on just a single axial CT image of the chest (see the first image below). Secondary findings of bleeding in the anterior mediastinum and possible aortic injury are important related patterns (see the second image below).
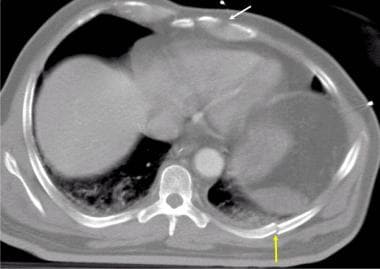
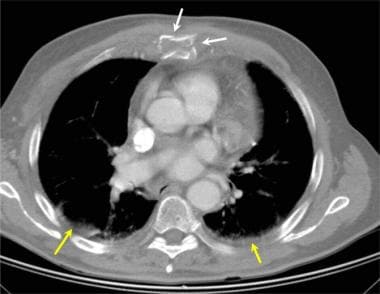 Axial computed tomography image of the chest. This image demonstrates a comminuted fracture of the body of the sternum (white arrows). The aorta was intact in this case. Note the bilateral posterior pulmonary contusions (yellow arrows).
Axial computed tomography image of the chest. This image demonstrates a comminuted fracture of the body of the sternum (white arrows). The aorta was intact in this case. Note the bilateral posterior pulmonary contusions (yellow arrows).
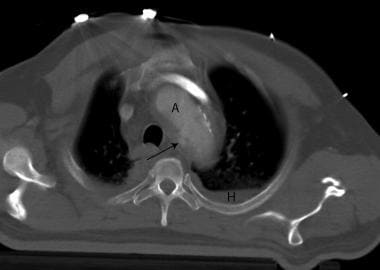 Axial computed tomography image of multiple left upper rib fractures and a traumatic aortic rupture. The contour of the aorta (A) is distorted (arrow) at the site of the aortic rupture. The rib fractures are also associated with a left hemothorax (H).
Axial computed tomography image of multiple left upper rib fractures and a traumatic aortic rupture. The contour of the aorta (A) is distorted (arrow) at the site of the aortic rupture. The rib fractures are also associated with a left hemothorax (H).
The occurrence of multiple rib fractures may be associated with critical vascular injuries to the aorta and, less commonly, the heart. Aortic tears are most commonly seen in the region of the ductus arteriosus or near the root of the aorta. Cardiac rupture has been diagnosed postmortem most often associated with sternal fractures or multiple rib fractures. Rupture of the heart has been reported in living patients. [8]
Delayed complications of multiple contiguous rib fractures may include heniation of a portion of the lung throught the chest wall defect. CT scan shown below demonstrates such a pulmonary herniation, which occurred on a delayed basis.
 A portion of the right lung has herniated through the right chest wall (white arrow) due to multiple contiguous right rib fractures.
A portion of the right lung has herniated through the right chest wall (white arrow) due to multiple contiguous right rib fractures.
Degree of confidence
Rib fractures that are seen on standard radiographs obtained with a rib detail protocol are not always clearly demonstrated on CT images viewed with a soft tissue window. CT scans obtained for trauma evaluation should be viewed using a bone window. CT scans can be reformatted into 2-mm-thick scan sections with a bone technique, which will demonstrate nearly all rib fractures. CT examinations performed with a multiple detectors allow faster scans, thinner sections, and less severe motion artifacts. In selected cases, multiplanar reformatted (MPR) images may be helpful.
Because the ribs lie in the axial plane, axial CT scans may not depict fractures that are otherwise easily seen on conventional radiographs. If the axial CT sections are obtained with scan thicknesses greater than 4 mm, nondisplaced fractures can be missed due to partial volume averaging. On the other hand, partial volume averaging may occasionally cause a depiction that suggests a rib fracture that is not present.
Anomalies of the ribs that thin, twist, or otherwise distort the ribs further contribute to possible false-positive diagnoses of rib fractures.
Small, loculated areas of pneumothorax and hemothorax can occur in the absence of rib fractures.
Artifacts caused by electrocardiograph (ECG) leads, IV tubing, and other devices may result in false-negative CT angiography studies.
The failure to correctly time the IV contrast bolus may result in a low Hounsfield unit (HU) value within the aorta. Dense contrast within the superior vena cava may generate a streak artifact near the ascending aortic root, which may falsely suggest a rib fracture.
Although intravenous contrast is not necessary for the diagnosis rib fractures, contrast-enhanced CT of the chest is recommended in order improve the sensitivity for the diagnosis of associated vascular injuries. [8]
Chest CT is considered the gold standard of detecting rib fractures, but the fractures may not be clinically significant. Chest CT is more important in general assessment of trauma for other injuries. Whole-body CT has become standard practice in the management of severely injured trauma patients, but it is necessary to improve rib fracture diagnosis accuracy on CT. Significant progress has been made in clinical applications based on deep learning techniques for medical image interpretation, such as algorithms based on deep convolutional neural networks (DCCN) for CT. [1, 15, 16, 17, 18, 19, 20]
Sano studied 217 rib fractures in 75 patients who underwent both chest CT and rib radiography. Rib radiography missed 43 fractures in 24 patients, with causes being overlap with organs in 15 cases, trivial fractures in 21 cases, and injury outside the imaging range in 7 cases. CT missed 21 rib fractures in 17 patients, with causes being horizontal fractures in 10 cases, trivial fractures in 9 cases, and insufficient breath holding in 1 case. [38]
Magnetic Resonance Imaging
Although magnetic resonance imaging (MRI) is not used as a primary means of detecting rib fractures, displaced or angulated lateral rib fractures as well as posterior rib fractures can be detected by MRI. Anterior chest wall movement with breathing may limit the visualization of nondisplaced fractures. Gradient-echo MRI, T2 fast-spin echo (FSE), and T2 short tau inversion recovery (STIR) sequences demonstrate the edema that is related to rib fractures. Spinal fractures may be associated with secondary effects of posterior rib fractures such as hemorrhage and edema. Lower cervical spine injury may be associated with fractures of the first or second ribs.
Breathing motion can cause artifacts, resulting in nondiagnostic MRIs of anterior rib fractures. Partial-volume effects may result in a false suggestion of a nondisplaced rib fracture.
Ultrasonography
Direct visualization of rib fractures is generally not possible with ultrasonography. However, the presence of a hemothorax can be confirmed with ultrasonography of the pleural space, and edema in the chest-wall muscles may be seen as thickening of the pleural space, as well as the alteration of the echogenic pattern within the chest-wall muscles. [39, 40, 41, 42, 43]
Hemothorax cannot be consistently differentiated from a pleural effusion. The visualization of a splenic or hepatic hematoma may indirectly suggest a search for a rib fracture. Ultrasonography is not effective in the visualization of a pneumothorax, small pleural effusions, and nondisplaced rib fractures.
In a study by Celik et al comparing the diagnostic accuracy of US with that of CT for detecting rib fractures in 145 patients who presented to the ED with blunt chest trauma, diagnostic accuracy of US was 80%, with a sensitivity of 91.2% and a specificity of 72.7%. However, a positive US performed poorly in determining the exact location and number of the fractured ribs. [40]
In a study by Hwang and Lee of 201 patients with blunt chest trauma who underwent radiographic and US examinations, of the 132 patients who showed no rib fractures on radiography, 92 showed fractures on US. In addition, of the 69 patients with rib fractures detected on radiography, 33 had additional rib fractures detected on US. [42]
Nuclear Imaging
Nuclear medicine techniques are useful in the detection of subacute rib fractures, as well as costochondral separations. The bone-seeking 99mTc-labeled phosphonates are selectively distributed into the areas that surround healing rib fractures. The dose of 99mTc-medronate is usually 800 megabecquerels (MBq). Imaging is generally performed after a 4-5 hour delay to allow the clearing of the diagnostic agent from the blood pool.
If a localized lesion is under investigation, regional blood flow can be evaluated with a 3-phase study in which a flow phase, a blood-pool image, and delayed static images are obtained. The flow phase is obtained immediately. The static images are generally obtained 4 hours after the administration of the diagnostic agent.
Increased regional nuclear activity within a chest-wall contusion may be detected on immediate imaging. A positive result for a rib fracture is represented by a focal area of increased nuclear activity. In the case of a linear fracture, the increased activity is localized to the site of the injury. If a large area of the chest wall is injured, several ribs in multiple locations may demonstrate an increased uptake of the radionuclide. [44]
Degree of confidence
Increased radionuclide uptake in the area of chest-wall trauma indicates a rib fracture in most cases. The application of lateral, oblique, and single-photon emission computed tomography (SPECT) imaging techniques improve diagnostic accuracy. Standard radiographs and the results of CT scans of the chest should be compared with bone scans whenever possible.
Positive results with radionuclide imaging require a moderate degree of cooperation from the injured patient. Movement, including rapid breathing, results in poor image quality and decreased sensitivity. A rib fracture is generally seen as a site of increased nuclear activity after a short (12- to 24-hr) delay in a young patient. In older patients and in patients with metabolic bone disease, fractures may not be visible until 72 hours after an injury. Except for pathologic fractures, a bone scan that is directed toward the detection of rib fractures should be delayed 48-72 hours after the traumatic event.
Normal costochondral uptake in a child may be intense enough to suggest rib stippling when viewed from a posterior projection. Any disease or lesion of a rib that results in increased bone turnover may result in positive findings in the ribs. False-negative results may occur in patients who have received iron dextran injections. High levels of iron in the bone marrow interfere with the normal uptake of bone. Fractures or other lesions of the ribs may not be detected until the iron storages return to normal.
Angiography
Selective angiography has a limited role in the evaluation of rib fractures. Thoracic angiograms may show a traumatic pseudoaneurysm or the extravasation of contrast material into the pleural space. Complications in cases of multiple trauma may include central vascular injury (aortic tear) and laceration of the subcostal artery. Direct visualization of active hemorrhage that is associated with a rib fracture is useful in the direction of surgical or angiographic intervention. Diagnostic angiography may be helpful in demonstrating a remote vascular injury and the delayed development of a pseudoaneurysm or arteriovenous fistula (AVF).
Degree of confidence
Thoracic angiography is both sensitive and specific for traumatic aortic injury. Injury to the subclavian artery may require selective injection of a contrast agent into the proximal subclavian artery to make the diagnosis of a traumatic pseudoaneurysm. The use of digital subtraction angiography (DSA) permits full evaluation of the injured artery without the artifacts that are caused by any superimposed bone.
The failure to identify an arterial laceration or pseudoaneurysm is most commonly associated with motion artifacts, rotation, or poor angiographic technique. Ulcerated plaques within the aortic arch of older patients have been mistaken for aortic trauma. The origin of branch vessels that is otherwise poorly filled has been mistaken for small aneurysms.
-
Image of the common middle rib. The common middle rib consists of the neck that is closest to the thoracic spine with an articular tubercle, the angle of which is a curved portion of the rib, and the distal body.
-
Image of central rib, viewed from the back, in which the subcostal groove is best seen. The costal artery and nerve follow the subcostal groove.
-
Image of the first rib, which is one of the upper, specialized ribs. Important features of the first rib include the attachments of the scalenus medius and serratus anterior muscles. Grooves for the subclavian artery and vein represent important potential areas of serious injury in fractures of the first rib.
-
Image of the 10th rib. Note that the 10th rib has a single articular facet. No direct anterior connection to the sternum is present. The forms of the 10th, 11th, and 12th ribs are similar.
-
Image of a typical upper thoracic rib. Each of the 9 upper thoracic ribs has 2 posterior articulations with a thoracic vertebral body above and below (costovertebral junction [CVJ]) and an anterior articulation with the sternum (costochondral junction [CCJ]). VB = vertebral body.
-
Image of the 12th rib. Note the single articular facet and the absence of an angle.
-
Frontal image of the rib cage. Ribs 1-12 demonstrate the variable shape of the upper 9 ribs. The 12th rib does not articulate anteriorly. The sternum consists of the manubrium (M), the body (S), and the xiphoid (X). The ribs articulate with the sternum via the costochondral (CC) junction. C = clavicle.
-
Posterior image of the thorax. The ribs are numbered 1-12. The clavicle (C) and scapula (S) are often involved in injuries that include rib fractures.
-
Anteroposterior (AP) chest radiograph in a patient who presented with severe left chest wall pain after a minor fall. No rib injury is apparent.
-
Anteroposterior (AP) radiograph of an elderly female patient with severe left chest wall pain after a minor fall. This image demonstrates a left lateral rib fracture (arrow) that is not seen on the standard AP chest radiograph.
-
This detailed oblique radiograph shows 2 rib fractures (arrows) that are not depicted on anteroposterior (AP) chest radiographs.
-
This anteroposterior (AP) chest radiograph demonstrates a left lateral lower rib fracture (white arrow). In addition, there is an associated left subcutaneous gas pattern that dissects along the left chest wall (black arrow).
-
Semi-erect anteroposterior (AP) chest radiograph in a patient with a nondisplaced posterior fracture of the left 10th rib. A small, apical pneumothorax (black arrow) is present on the left, and there is volume loss in the left lower lobe (white arrow).
-
Image depicting multiple fractures of the left upper chest wall. The first rib is often fractured posteriorly (black arrows). If multiple rib fractures occur along the midlateral (red arrows) or anterior chest wall (blue arrows), a flail chest (dotted black lines) may result.
-
Anteroposterior (AP) supine chest radiograph that was obtained upon a patient's arrival in the emergency department after a serious automobile accident. Although rib fractures are identified along the left lateral chest wall (black arrows), the transportation bed created superimposed metal artifacts (blue arrows) that obscure visualization of possible other rib fractures along the chest wall.
-
Supine anteroposterior (AP) chest radiograph that was obtained after the removal of metal artifacts along the left chest wall. Multiple posterolateral rib fractures are noted on the left (arrows; Note: White and black arrows were used for easy visualization due to the dark and light areas of the lungs).
-
Supine anteroposterior (AP) chest radiograph shows the presence of a right tension pneumothorax, which has displaced the trachea to the right (blue arrow). A displaced right lower rib fracture is present in the right posterolateral aspect of the chest (black arrow).
-
Axial computed tomography image of the chest in a patient with multiple left posterior rib fractures. A large left pneumothorax is present (arrows).
-
Axial computed tomography image of the chest in a patient with left posterior rib fractures. The left pneumothorax (white arrows) is associated with a displaced posterior left rib fracture (black arrow). Secondary effects on the left lung include a pulmonary contusion and volume loss.
-
Axial computed tomography image of the chest in a patient with trauma to the left chest wall, where air (yellow arrow) is noted. A small left pneumothorax (blue arrow) is present, and the posterior left lung and the pleural space are opacified due to the combination of a left hemothorax and a left pulmonary contusion.
-
Supine anteroposterior (AP) chest radiograph. This image demonstrates increased opacity of the left lateral upper lobe (arrow), a finding that is consistent with a pulmonary contusion after left chest wall trauma and rib fractures.
-
Axial computed tomography image of the chest in a patient with a complex, unstable, thoracic spinal fracture. Multiple rib fractures (white arrows) are shown. In addition, the midthoracic spine is fractured (yellow arrow), and a large right hemothorax (HT) is present. CT = chest tube.
-
Axial computed tomography image of the lower cervical spine in a patient with multiple rib fractures and an unstable fracture of the thoracic spine. Air has dissected into the epidural space posterior to the cervical dura (arrows).
-
Sagittal reformatted computed tomography image of the cervical spine in a patient with multiple rib fractures and an unstable thoracic spinal injury. Epidural gas is noted dorsally in the spinal canal (arrows).
-
Abdominal radiograph. This image demonstrates moderate gaseous distention. The distended stomach was associated with a hemoperitoneum.
-
Axial computed tomography image of the chest in a patient with both anterior and posterior thoracic injuries. A fracture of the sternum (white arrow) and a posterior left rib fracture (yellow arrow) are present.
-
Axial computed tomography image of the lower thorax in a patient with multiple trauma. A left lower posterior rib fracture has resulted in a splenic contusion (arrow).
-
Axial computed tomography image in a patient with a severe thoracic injury. Rib fractures and a complex left scapular fracture (arrows) are present.
-
Axial computed tomography image of the chest. This image demonstrates a comminuted fracture of the body of the sternum (white arrows). The aorta was intact in this case. Note the bilateral posterior pulmonary contusions (yellow arrows).
-
Axial computed tomography image of multiple left upper rib fractures and a traumatic aortic rupture. The contour of the aorta (A) is distorted (arrow) at the site of the aortic rupture. The rib fractures are also associated with a left hemothorax (H).
-
Axial computed tomography image of the chest in a patient with multiple anterior and posterior rib fractures. A liver laceration is present. Air is noted in the subcutaneous space surrounding the left ribs (white arrows), blood is in the perisplenic space (black arrow), and a subcutaneous emphysema is present along the left chest wall. The patient was also treated for a large left pneumothorax.
-
Axial computed tomography image of the brain in a patient with multiple rib fractures and a tension pneumothorax. Multiple bilateral cerebral infarcts are present (arrows). The direct injury to the brain was less complicated by hypoxia.
-
Chest radiograph in a patient who presented with a gunshot wound to the anterior chest wall. Note the pulmonary contusion (arrow). The bullet struck an anterior right rib, resulting in a rib fracture. Other injuries involved the pleura and lung on the right.
-
Axial computed tomography image of the chest in a patient with a gunshot wound. Note the comminuted rib fracture (black arrow). A lung contusion is present along the path of the bullet (yellow arrow). A chest tube was placed to treat the right pneumothorax.
-
Computed tomography image of the chest. This image demonstrates bilateral lower lobe volume loss in a patient with multiple rib fractures.
-
Right rib radiograph in a 48-year-old male who presented with severe right posterior chest wall pain following a fall. This image demonstrates 2 fractures of the right chest wall (white arrows).
-
Computed tomography image of the chest in a patient who sustained multiple rib fractures. This image demonstrates an irregular area of low density in the medial posterior right lobe of the liver, a pattern that is consistent with a liver contusion.
-
Computed tomography image of the chest. Posterior lateral rib fractures are noted (white arrow), as well as multiple liver contusions.
-
Chest radiography in a patient who had sustained a fall 2 weeks previous to presentation. The patient complained of right-sided chest pain.
-
Computed tomography image of the chest. This image demonstrates a posterior right chest wall rib fracture, which is related to a contusion within the right lobe of the liver.
-
Axial computed tomography image of the chest. This image demonstrates a posterior fibro thorax (ie, fibrosis of the pleural space) (white arrows).
-
If the management of multiple rib fractures is complicated by reducing lung function, the chest wall can be stabilized by the use of plates held in position by multiple screws (black arrows).
-
The treatment of multiple rib fractures includes the option of alignment and fixation of the fractures if respiration is compromised. After alignment, a plate was applied to each of four displaced rib fractures, held in position by multiple screws (white arrows).
-
Lung tissue has herniated through a defect in the right chest wall. The defect was the result of multiple right rib fractures.
-
A portion of the right lung has herniated through the right chest wall (white arrow) due to multiple contiguous right rib fractures.









