Practice Essentials
Acute cholecystitis (AC) occurs as a result of inflammation of the gallbladder (GB) wall, usually because of obstruction of the cystic duct (see the image below). In 90% of cases, AC is initiated by the impaction of a calculus in the neck of the GB or in the cystic duct. [1] Cholelithiasis affects approximately 20 million people in the United States each year, with 20% of symptomatic patients developing acute calculus cholelithiasis (ACC), accounting for 3-9% of hospital admissions for acute abdominal pain. [2]
Acute acalculous cholecystitis (AAC) represents inflammation of the GB in the absence of GB calculi. AAC occurs more commonly in children and adults who are critically ill or in those who have recently undergone the stress of severe trauma, burns, or major surgery.
Emphysematous cholecystitis (EC) is a rare life-threatening form of acute cholecystitis representing between 1% and 3% of acute cholecystitis, with an associated mortality of 25%. [3] It occurs most frequently in male patients aged 50–70 years, often with comorbid diabetes mellitus, immunosuppression, or peripheral vascular disease. EC is characterized by the pres gas in the gallbladder lumen, the gallbladder wall and adjacent structure, and elsewhere in the biliary tracts in the absence of an abnormal communication with the gastrointestinal tract. The gas may disseminate to subcutaneous tissue, as well as to the peritoneal and retroperitoneal cavity. [4]
Clinically, few signs differentiate uncomplicated AC from complicated AC. Complications of AC may have serious clinical implications. These complications include perforation, pericholecystic abscess, empyema, and bilioenteric fistula. Therefore, radiologic imaging makes a substantial contribution to the differential diagnosis. [5]
Preferred examination
Ultrasonography and nuclear medicine studies are the best imaging studies for the diagnosis of both cholecystitis and cholelithiasis. However, the performance of ultrasonography in the diagnosis of inflammation of the gallbladder is not as good as its performance in the diagnosis of gallstones. [5] Although ultrasonography significantly aids in the diagnosis of AC, most ultrasonographic signs are not typical but suggestive of AC. [2, 6, 7] Nevertheless, ultrasonography is usually favored as the initial test. Hepatobiliary iminodiacetic acid scan (HIDA scan) has the highest sensitivity and specificity for acute cholecystitis, although its scarce availability, long time required to perform the test, and exposure to ionizing radiation limit its use to patients with inconclusive ultrasonography results. [1]
The main features of AC on ultrasonography are all nonspecific findings. Examples include GB thickening, calculi in the GB, a positive ultrasonographic Murphy sign, and pericholecystic fluid. The sonographic Murphy sign is negative in as many as 70% of patients with AC. In cases of perforated GB, the wall of the GB is not well delineated, and a localized interruption of the wall may not be noted at the site of perforation. The diagnosis is difficult to make with ultrasonography in obese patients and in patients with gaseous distention. Ultrasonography remains operator dependent.
Plain radiography, computed tomography (CT) scans, and endoscopic retrograde cholangiopancreatography (ERCP) are diagnostic adjuncts.
For patients with AC, plain radiographic findings may be entirely normal. Radiolucent calculi are visible. Opaque calculi in the right upper quadrant on plain abdominal radiographs may be an incidental finding and is not necessarily related to AC.
Inflammatory pericholecystic reaction in the GB fossa is better depicted with CT scanning than with other modalities. CT scanning is also useful in making the differential diagnosis when obesity or gaseous distention limits the use of ultrasonography. CT scanning exposes the patient to a radiation burden, which may not be necessary, while arteriography is invasive and is seldom indicated. Magnetic resonance imaging (MRI) may demonstrate the same morphologic changes as CT scanning, displaying inflammatory changes in the GB wall, pericholecystic fat, and intrahepatic periportal tissues. [7, 8, 9, 10] MRI has limited availability, and it is expensive. In addition, in patients with certain prosthetics, surgical clips, cardiac pacemakers, or claustrophobia, the diagnosis is difficult to make with MRI.
Diffusion-weighted (DW) MRI shows potential for differentiating between acute and chronic cholecystits. In a study comprising 83 patients with abdominal pain, Wang et al noted that increased signal on high b-value images were highly sensitive and moderately specific for acute cholecystitis. [11]
Although cholescintigraphy is sensitive, it has low specificity and involves the use of ionizing radiation.
 Plain abdominal radiograph of a 68-year-old woman who presented with acute abdominal pain. There are multiple calculi distributed in a pyriform shape in the right upper quadrant; these are suggestive of gallstones. Gallstones were diagnosed during sonography several months earlier. A clinical diagnosis of acute cholecystitis was made. However, the plain radiograph also shows features of a pneumoperitoneum. At laparotomy, a perforated cecal carcinoma was found. There were no findings of acute cholecystitis.
Plain abdominal radiograph of a 68-year-old woman who presented with acute abdominal pain. There are multiple calculi distributed in a pyriform shape in the right upper quadrant; these are suggestive of gallstones. Gallstones were diagnosed during sonography several months earlier. A clinical diagnosis of acute cholecystitis was made. However, the plain radiograph also shows features of a pneumoperitoneum. At laparotomy, a perforated cecal carcinoma was found. There were no findings of acute cholecystitis.
Ultrasonographic anatomy
The GB is a pear-shaped, anechoic structure indenting the inferomedial aspect of the right lobe of the liver. A linear, echogenic line representing fat in the main interlobar fissure is interposed between the GB and the right main portal vein. The GB mucosa is hyperechoic, the submucosa and the muscle layer are hypoechoic, and the serosal surface fatty layer is hyperechoic.
A linear fold known as the junctional fold is present on the posterior GB wall at the junction of the body and neck. This structure is of no pathologic significance.
Sound waves from the spiral valve of the neck may cast an acoustic shadow and may mimic a gallstone. The normal thickness of the GB wall is usually less than 3 mm. Provided that the patient has been fasting for 8-12 hours, visualization of the normal GB should be nearly complete. Nonvisualization of the GB is a pathologic finding in 96% of cases involving truly fasting patients.
Guidelines
The American College of Radiology (ACR) makes the following imaging recommendations [12] :
-
Ultrasonography is the preferred initial imaging test for the diagnosis of acute cholecystitis; scintigraphy is the preferred alternative.
-
CT is a secondary imaging test that can identify extrabiliary disorders and complications of acute cholecystitis.
-
CT with intravenous (IV) contrast is useful in diagnosing acute cholecystitis in patients with nonspecific abdominal pain.
-
MRI, often with IV gadolinium-based contrast medium, is also a possible secondary choice for confirming a diagnosis of acute cholecystitis.
-
MRI without contrast is useful for eliminating radiation exposure in pregnant women when ultrasonography has not yielded a clear diagnosis.
-
Contrast agents should not be used in patients on dialysis unless absolutely necessary.
The 2016 World Society of Emergency Surgery (WSES) guidelines are in agreement that ultrasonography is the preferred initial imaging test for diagnosis of ACC. However, the WSES guidelines find the evidence of diagnostic accuracy for CT and MRI to be insufficient and concluded that a combination of clinical, laboratory, and imaging findings are needed to diagnose ACC, although the best combination is not known. [1]
Despite concerns about diagnostic accuracy of ultrasonography, the Tokyo Guidelines 2018 (TG18) continue to recommend it as the preferred imaging for the diagnosis of AC based on its low invasiveness, widespread availability, ease of use, and cost‐effectiveness. The guidelines noted that no recent studies were found to support the use of color or power Doppler sonography for diagnosing acute cholecystitis. Other key imaging recommendations included the following [13] :
-
MRI/MRCP is useful for diagnosing acute cholecystitis if abdominal US does not provide a definitive diagnosis.
-
Contrast‐enhanced CT or contrast‐enhanced MRI for diagnosing gangrenous cholecystitis.
-
CT for diagnosing emphysematous cholecystitis.
Diagnostic Criteria
The Tokyo Guidelines 2013 (TG13) diagnostic criteria for acute cholecystitis became widely adopted and were reaffirmed in TG18 and are summarized in Table 1, below. [13]
TG18/TG13 Diagnostic Criteria for Acute Cholecystitis (Open Table in a new window)
| Local Inflammation Signs | Systemic Inflammation Signs | Imaging Findings |
|---|---|---|
| Murphy's sign | Fever | Imaging characteristic of acute cholecystitis |
| Right upper quadrant mass | Elevated C-reactive protein | |
| Right upper quadrant pain or tenderness | Elevated white blood count | |
| Suspected Diagnosis: 1 local inflammation sign and 1 systemic inflammation sign | ||
| Definite Diagnosis: 1 local inflammation sign, 1 systemic inflammation sign, and characteristic imaging findings | ||
Patient education
For patient information resources, see the Gallbladder, and Pancreas Center, as well as Gallstones.
Radiography
For patients with acute cholecystitis (AC), an acute plain abdominal radiograph is obtained primarily to exclude other diagnoses. Disorders such as empyema of the gallbladder (GB) and gallstone ileus may be suggested by findings on plain radiographs. Likewise, porcelain GB and milk-of-calcium bile have fairly characteristic appearances (see the images below). [14]
Plain abdominal radiograph of a 68-year-old woman who presented with acute abdominal pain. There are multiple calculi distributed in a pyriform shape in the right upper quadrant; these are suggestive of gallstones. Gallstones were diagnosed during sonography several months earlier. A clinical diagnosis of acute cholecystitis was made. However, the plain radiograph also shows features of a pneumoperitoneum. At laparotomy, a perforated cecal carcinoma was found. There were no findings of acute cholecystitis.
 (Left) Plain radiograph of a 57-year-old woman presenting with right iliac fossa pain and mild fever shows large laminated opacities in the right iliac fossa (RIF); these findings suggest gallstones (arrow). Two smaller nonlaminated oval opacities are present more medially; these were interpreted as calculi in the cystic duct. Ultrasonography revealed a Reidel lobe of the liver. The gallbladder was located in the RIF and contained several calculi; however, no ultrasonographic features of acute cholecystitis were observed. The right kidney was also placed in the RIF, in a more medial location. Two calculi were present—one each in the upper and lower pole calices. (Right) Intravenous urogram shows a low-lying right kidney with calculi in the upper and lower pole calices. Urine culture revealed Escherichia coli. The patient's condition responded to a course of antibiotics. This example shows that an acute pyelonephritis can clinically mimic acute cholecystitis. With a Reidel lobe, the gallbladder may be located in the RIF, and an acute cholecystitis may mimic appendicitis or other RIF pathology.
(Left) Plain radiograph of a 57-year-old woman presenting with right iliac fossa pain and mild fever shows large laminated opacities in the right iliac fossa (RIF); these findings suggest gallstones (arrow). Two smaller nonlaminated oval opacities are present more medially; these were interpreted as calculi in the cystic duct. Ultrasonography revealed a Reidel lobe of the liver. The gallbladder was located in the RIF and contained several calculi; however, no ultrasonographic features of acute cholecystitis were observed. The right kidney was also placed in the RIF, in a more medial location. Two calculi were present—one each in the upper and lower pole calices. (Right) Intravenous urogram shows a low-lying right kidney with calculi in the upper and lower pole calices. Urine culture revealed Escherichia coli. The patient's condition responded to a course of antibiotics. This example shows that an acute pyelonephritis can clinically mimic acute cholecystitis. With a Reidel lobe, the gallbladder may be located in the RIF, and an acute cholecystitis may mimic appendicitis or other RIF pathology.
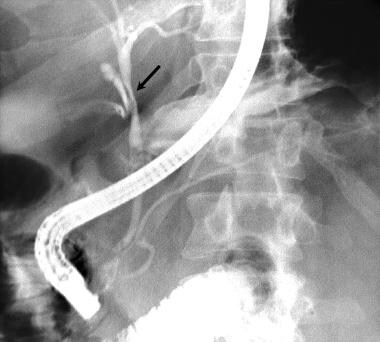 This patient presented with acute cholecystitis, as confirmed at imaging. His pain resolved over a few days, but mildly elevated bilirubin levels persisted. Endoscopic retrograde cholangiopancreatographic (ERCP) study shows smooth narrowing of the bile duct (arrow) at the site of insertion of the cystic duct (Mirizzi syndrome). Note the small calculus in the cystic duct.
This patient presented with acute cholecystitis, as confirmed at imaging. His pain resolved over a few days, but mildly elevated bilirubin levels persisted. Endoscopic retrograde cholangiopancreatographic (ERCP) study shows smooth narrowing of the bile duct (arrow) at the site of insertion of the cystic duct (Mirizzi syndrome). Note the small calculus in the cystic duct.
The plain radiograph may reveal dilated loops of the small bowel in the right upper quadrant (see the image below); these findings may mimic those of small-bowel obstruction. Rarely, the GB is identified as a soft-tissue mass.
 Plain abdominal radiograph in a patient with a clinical diagnosis of acute cholecystitis. The diagnosis was confirmed by means of abdominal ultrasonography. The radiograph shows faint opacities in the region of the gallbladder fossa and dilated loops of small bowel in the epigastrium and mid abdomen secondary to localized ileus.
Plain abdominal radiograph in a patient with a clinical diagnosis of acute cholecystitis. The diagnosis was confirmed by means of abdominal ultrasonography. The radiograph shows faint opacities in the region of the gallbladder fossa and dilated loops of small bowel in the epigastrium and mid abdomen secondary to localized ileus.
On abdominal plain radiographs, the following signs should be assessed:
-
Opacities projected over the GB
-
Linear calcifications in GB walls
-
GB enlargement
-
Focal gas collections within the GB
-
Air-fluid levels in the GB lumen
Plain radiographs may reveal gallstones, which appear as single or multiple pyramidal, faceted, or cuboidal calcifications located in the right upper quadrant. Calcification may be central, homogeneous, or rimlike. When multiple gallstones are seen, the stones are clustered and are usually faceted. On erect images, stones may be layered in the dependent portion of the GB.
Occasionally, stellate radiolucencies are seen in the area of GB. These reflect gas-containing fissures within the GB calculi. This finding is referred to as the Mercedes-Benz sign. Gas in the GB wall or lumen is a feature of emphysematous cholecystitis. Calcification of the GB wall, or porcelain GB, is an indicator of chronic cholecystitis.
Biliary sludge of high calcium content, or limy bile, is also a feature of chronic cholecystitis. Gas may be seen in the bile ducts in cystocutaneous or cystoenteric forms with fistulous complications. The gallstone may pass through such a fistula into the gut and cause gallstone ileus. The stone usually has to be 25 mm in diameter to cause ileus. The ileum near the ileocecal junction is the most common site.
Emphysematous cholecystitis (see the image below) occurs as a complication of acute acalculous cholecystitis (AAC) in more than 50% of cases. Air is readily seen on plain abdominal radiographs. On upright radiographs, an air-fluid level in the right upper quadrant may be seen. This finding represents gas within the GB lumen admixed with inflammatory fluid, sludge, or both. Air within the wall of the GB appears more curvilinear. Gas visualized in the GB in the setting of AAC is highly associated with complications such as gangrene and perforation.
 Plain abdominal radiograph in a 49-year-old diabetic woman shows air within the gallbladder lumen due to emphysematous cholecystitis (arrow).
Plain abdominal radiograph in a 49-year-old diabetic woman shows air within the gallbladder lumen due to emphysematous cholecystitis (arrow).
Advantages and disadvantages of radiography
For patients with gallbladder disease, plain abdominal radiographic findings are nonspecific and are not useful in differentiating between biliary colic and acute cholecystitis. Plain radiography has been superseded by ultrasonography for such patients.
Nevertheless, plain radiography still has value in cases in which the GB is not definitively identified by ultrasonography. Emphysematous cholecystitis may be recognized easily on plain films. (Ultrasonography may be used in cases in which calcifications in the right upper quadrant are not of typical appearance or location.)
On plain abdominal radiographs, however, small bowel dilatation in the right upper quadrant caused by acute cholecystitis may be confused with small bowel obstruction.
The differential diagnosis for gallstones includes renal calculi, which are related to renal outline and which may be separated on oblique images if necessary. Only 50% of pigment stones and 20% of cholesterol stones contain sufficient calcium to be visible on plain radiographs. Gas in the biliary system must be differentiated from abscess or gas-forming collections in the GB fossa. Ultrasonography may prove useful in such cases.
Porcelain GB has the characteristic appearance of eggshell calcification in the right upper quadrant. Other right–upper-quadrant calcifications, such as hepatic granulomas, tumor calcification, costal cartilage calcification, calcified mesenteric lymph nodes, and hepatic or renal artery aneurysms, are rarely confused with GB calculi.
Computed Tomography
For cases of acute cholecystitis (AC), CT scan findings include the following: gallstones within the gallbladder (GB), the cystic duct, or both; more than 3 mm of focal or diffuse thickening of the GB wall in a noncontracted GB; indistinct liver-GB interface; fluid in the GB fossa in the absence of ascites; enlargement of the GB, with the transverse diameter measuring more than 5 cm; infiltration of the surrounding fat; increased bile attenuation, caused by biliary sludge; and GB mucosal sloughing. [7, 8]
A low-attenuating ring surrounding the GB may be indicative of edema of the outer layer of the GB wall, or it may suggest the accumulation of fluid in the GB fossa. In hemorrhagic cholecystitis, the attenuation values of the GB contents may be abnormally elevated.
Contrast-enhanced CT scanning shows enhancement of the GB wall and the adjacent liver.
Inflammatory reaction in the pericholecystic fat is well seen on contrast-enhanced CT scans. This is a specific CT scan sign for AC. The inflammatory reaction is seen as streaky or bandlike areas of attenuation of soft tissue extending from the GB wall into the surrounding fat.
CT scanning may be useful in the diagnosis of acalculous cholecystitis by showing the various signs described. However, CT scanning may be difficult to perform because of the patients' poor condition.
In cases of emphysematous cholecystitis, CT scanning may demonstrate intramural and intraluminal air within the GB better than plain abdominal radiography can. However, CT scanning is not strictly needed for the diagnosis.
Mucosal sloughing and intramural gas are specific signs of acute cholecystitis, but these are seen infrequently. The reported sensitivity and specificity of CT scan findings are 90-95%. CT scanning is more sensitive than ultrasonography in the depiction of a pericholecystic inflammatory response and in localizing pericholecystic abscesses, pericholecystic gas, and calculi outside the GB lumen.
In cases of complicated AC, some CT scan features may mimic those of GB carcinoma. The features that may be confused with a carcinoma include diffuse or focal thickening of the GB wall and inflammatory infiltrate of the surrounding fat.
Magnetic Resonance Imaging
In cases of acute cholecystitis (AC), MRI may depict the same pathologic features as CT scanning does. Increased blood flow and capillary leakage resulting from inflammatory change are best exhibited by the use of gadolinium enhancement, particularly with fat-suppression techniques. Various morphologic changes may be observed (see the images below). [8, 10]
 Nonenhanced CT scans through the gallbladder (GB) shows an indistinct GB wall. Contrast-enhanced CT scan (bottom) shows an inflammatory reaction in the pericholecystic fat, which is seen as streaky or bandlike soft-tissue areas of attenuation extending from the GB wall into the surrounding fat. Note the loss of the interface between the GB and surrounding soft tissue on both the nonenhanced (top) and enhanced (bottom) scans. Note also the striking enhancement of GB and pericholecystic tissues following the use of intravenous contrast material.
Nonenhanced CT scans through the gallbladder (GB) shows an indistinct GB wall. Contrast-enhanced CT scan (bottom) shows an inflammatory reaction in the pericholecystic fat, which is seen as streaky or bandlike soft-tissue areas of attenuation extending from the GB wall into the surrounding fat. Note the loss of the interface between the GB and surrounding soft tissue on both the nonenhanced (top) and enhanced (bottom) scans. Note also the striking enhancement of GB and pericholecystic tissues following the use of intravenous contrast material.

With T1-weighted gadolinium-enhanced images, prominent enhancement is seen along the mucosal layer of the gallbladder (GB) wall; on delayed images, this enhancement progresses to involve the whole thickness of the GB wall. A greater-than-normal degree of enhancement of the GB wall correlates well with the presence of AC. GB wall thickening is well depicted on T1- and T2-weighted images. Transient liver enhancement is shown on immediate postgadolinium images, particularly T1-weighted and fat-suppressed images of the gallbladder fossa.
GB calculi are well seen on T2-weighted images, as is pericholecystic fluid. Intramural abscesses appear as areas of high signal foci on T2-weighted and fat-suppressed images.
Periportal high signal intensity is a nonspecific finding that is occasionally seen.
In hemorrhagic cholecystitis, which is more common in cases of acalculous cholecystitis (AAC), blood breakdown products may be identified on nonenhanced MRI scans. Because of the specific signal-intensity characteristics of blood products on T1- and T2-weighted images, the age of the hemorrhage may be determined.
A magnetic resonance cholangiopancreatography (MRCP) protocol may show calculi in the GB, cystic duct, and common bile duct (CBD). [9]
Evaluation of postcontrast images may reveal nonenhancing regions along the gallbladder wall, representing gangrenous cholecystitis. Susceptibility artifact within the gallbladder wall on gradient echo imaging can indicate foci of air. Complications of gangrenous cholecystitis include perforation and abscess formation. [15]
Gadolinium-based contrast agents have been linked to the development of nephrogenic systemic fibrosis (NSF) or nephrogenic fibrosing dermopathy (NFD). The disease has occurred in patients with moderate to end-stage renal disease after being given a gadolinium-based contrast agent to enhance MRI or MRA scans. NSF/NFD is a debilitating and sometimes fatal disease. Characteristics include red or dark patches on the skin; burning, itching, swelling, hardening, and tightening of the skin; yellow spots on the whites of the eyes; joint stiffness with trouble moving or straightening the arms, hands, legs, or feet; pain deep in the hip bones or ribs; and muscle weakness.
Degree of confidence
For the diagnosis of acute cholecystitis, the sensitivity and accuracy of gadolinium-enhanced MRI techniques are higher than they are with ultrasonographic techniques. The MRI techniques may detect pericholecystic fluid with greater accuracy than is possible with ultrasonography. MRI has much greater sensitivity for the detection of CBD calculi than does ultrasonography.
There are a multitude of causes of increased thickness of the GB wall. Both GB polyps and gallstones may float and appear as signal voids. However, unlike gallstones, polyps may demonstrate enhancement with the use of a gadolinium-based contrast agent. Contrast enhancement may also occur in cases of chronic cholecystitis, but mural enhancement is more pronounced on delayed images than on other images, and pericholecystic enhancement is minimal. (See the images below.)
The ultrasonograms below were taken in a woman with severe, right hypochondriacal pain that mimicked gallstones.
 Acute cholecystitis mimic. CT scan in a 36-year-old woman with severe right hypochondriacal pain. The gallbladder wall is thickened, with a suggestion of the triple wall sign. There is a streak of pericholecystic fluid at the inferior aspect of the gallbladder. An ultrasound for the Murphy sign was negative. No gallstones were seen. There were no predisposing causes of an acalculous acute cholecystitis. A supine CT scan showed signs of inflammation in the region of the duodenum, but the duodenal wall was not well seen. However, further CT scan sections in the right decubitus position showed spasm and thickening of the wall of the first part of the duodenum. Endoscopy revealed an acute penetrating duodenal ulcer.
Acute cholecystitis mimic. CT scan in a 36-year-old woman with severe right hypochondriacal pain. The gallbladder wall is thickened, with a suggestion of the triple wall sign. There is a streak of pericholecystic fluid at the inferior aspect of the gallbladder. An ultrasound for the Murphy sign was negative. No gallstones were seen. There were no predisposing causes of an acalculous acute cholecystitis. A supine CT scan showed signs of inflammation in the region of the duodenum, but the duodenal wall was not well seen. However, further CT scan sections in the right decubitus position showed spasm and thickening of the wall of the first part of the duodenum. Endoscopy revealed an acute penetrating duodenal ulcer.
 Acute cholecystitis mimic. A 36-year-old woman with severe right hypochondriacal pain. The gallbladder wall is thickened, with a suggestion of the triple wall sign. There is a streak of pericholecystic fluid at the inferior aspect of the gallbladder. An ultrasound of the Murphy sign was negative. No gallstones were seen. There were no predisposing causes of an acalculous acute cholecystitis. A supine CT scan showed signs of inflammation in the region of the duodenum, but the duodenal wall was not well seen. However further CT scan sections in the right decubitus position showed spasm and thickening of the wall of the first part of the duodenum. Endoscopy revealed an acute penetrating duodenal ulcer.
Acute cholecystitis mimic. A 36-year-old woman with severe right hypochondriacal pain. The gallbladder wall is thickened, with a suggestion of the triple wall sign. There is a streak of pericholecystic fluid at the inferior aspect of the gallbladder. An ultrasound of the Murphy sign was negative. No gallstones were seen. There were no predisposing causes of an acalculous acute cholecystitis. A supine CT scan showed signs of inflammation in the region of the duodenum, but the duodenal wall was not well seen. However further CT scan sections in the right decubitus position showed spasm and thickening of the wall of the first part of the duodenum. Endoscopy revealed an acute penetrating duodenal ulcer.
Ultrasonography
Ultrasonographic features of acute cholecystitis (AC) include the following [6, 2] :
-
Calculi in the gallbladder (GB), present in more than 90% of patients (calculi may be difficult to detect in the Hartmann pouch or cystic duct)
-
Anterior GB-wall thickness of more than 3 mm
-
Positive Murphy sign (pain on compression of the GB with the ultrasonographic probe)
-
Pericholecystic fluid in severe cases (indicative of actual or impending perforation)
-
Echo-poor halo in or around the GB wall or striated GB wall (indicative of edema)
-
Nonvisualization of the GB in a truly fasting patient (strong evidence of GB disease)
-
Acalculous cholecystitis (5% of cases not associated with gallstones)
-
GB distention (about 93% of patients with GB volume >70 mL have AC)
-
Increased periportal echogenicity (presumably the result of a local inflammatory infiltrate)
-
Loss of definition of GB margins
-
Intraluminal-wall desquamation, resulting in a lacelike lumen
-
Hypervascularization of the GB wall on color flow and power Doppler images, associated with GB-wall thickening on gray-scale imaging
-
Hypervascularization without GB-wall thickening possible in cases of AC
Features of cholecystitis are also found in the images below.
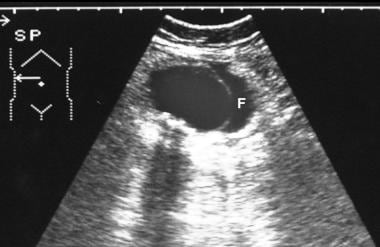
 Longitudinal oblique sonogram through the gallbladder shows a calculus at the neck of the gallbladder with acoustic shadowing and thickening of the gallbladder wall (arrow).
Longitudinal oblique sonogram through the gallbladder shows a calculus at the neck of the gallbladder with acoustic shadowing and thickening of the gallbladder wall (arrow).
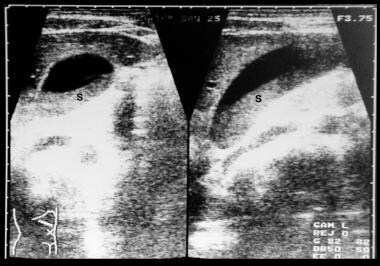 Longitudinal and axial scans through the gallbladder show layering of sludge (S) in the gallbladder lumen.
Longitudinal and axial scans through the gallbladder show layering of sludge (S) in the gallbladder lumen.
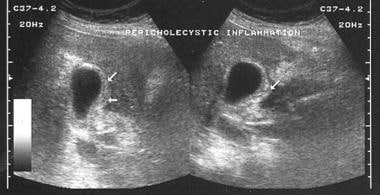
 Oblique and longitudinal sonograms through gallbladder shows marked laminated sonolucent thickening of the gallbladder wall, sludge, and edema (arrow).
Oblique and longitudinal sonograms through gallbladder shows marked laminated sonolucent thickening of the gallbladder wall, sludge, and edema (arrow).
 Axial scan through the gallbladder shows marked thickening of the gallbladder wall, with the lumen of the gallbladder full of sludge.
Axial scan through the gallbladder shows marked thickening of the gallbladder wall, with the lumen of the gallbladder full of sludge.
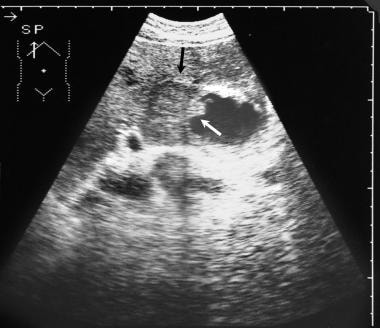
 This 26-year-old man known to be HIV positive presented with pain in the right upper quadrant and mild jaundice. Axial sonogram through the gallbladder and pancreas shows sludge within the gallbladder and the lower common bile duct (CBD). A diagnosis of acalculous cholecystitis was confirmed. Arrow indicates the CBD; A, aorta; GB, gallbladder; IVC, inferior vena cava; P, pancreas; and S, splenic vein.
This 26-year-old man known to be HIV positive presented with pain in the right upper quadrant and mild jaundice. Axial sonogram through the gallbladder and pancreas shows sludge within the gallbladder and the lower common bile duct (CBD). A diagnosis of acalculous cholecystitis was confirmed. Arrow indicates the CBD; A, aorta; GB, gallbladder; IVC, inferior vena cava; P, pancreas; and S, splenic vein.
 Ultrasonogram of the gallbladder shows focal thickening of the gallbladder wall (arrow) that mimics a carcinoma.
Ultrasonogram of the gallbladder shows focal thickening of the gallbladder wall (arrow) that mimics a carcinoma.
 Longitudinal oblique ultrasonogram through the gallbladder shows pseudomembrane formation due to sloughed mucosa. Note the small calculus.
Longitudinal oblique ultrasonogram through the gallbladder shows pseudomembrane formation due to sloughed mucosa. Note the small calculus.
 Axial ultrasonogram through the gallbladder shows tiny calculi in the gallbladder and pericholecystic fluid.
Axial ultrasonogram through the gallbladder shows tiny calculi in the gallbladder and pericholecystic fluid.
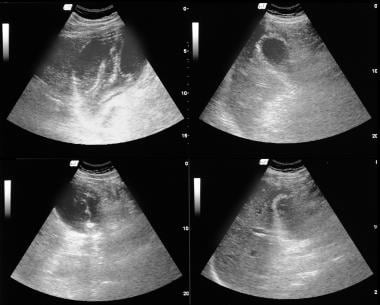 Four scans of different orientations through the gallbladder shows gallbladder wall thickening, pseudomembrane formation, sludge, and pericholecystic fluid.
Four scans of different orientations through the gallbladder shows gallbladder wall thickening, pseudomembrane formation, sludge, and pericholecystic fluid.
 Ultrasonogram shows complete disorganization of the gallbladder and its fossa that mimics a gallbladder carcinoma.
Ultrasonogram shows complete disorganization of the gallbladder and its fossa that mimics a gallbladder carcinoma.
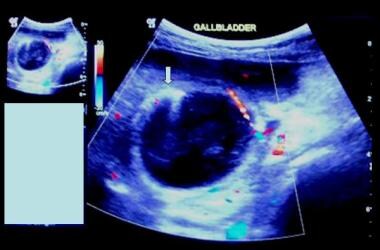 Acute emphysematous cholecystitis. Color Doppler images of the gallbladder of an 82-year-old male with diabetes mellitus who presented with abdominal distention and vomiting. Ultrasound shows a markedly thickened gallbladder wall, which is hypervascularized. There are no gallstones, but note the presence of air in the anterior wall of the gallbladder (arrow).
Acute emphysematous cholecystitis. Color Doppler images of the gallbladder of an 82-year-old male with diabetes mellitus who presented with abdominal distention and vomiting. Ultrasound shows a markedly thickened gallbladder wall, which is hypervascularized. There are no gallstones, but note the presence of air in the anterior wall of the gallbladder (arrow).
In children, AC may be acalculous, with increased GB-wall thickening, signs of hydrops, a positive ultrasonographic Murphy sign, and an increase in the diameter of the CBD as a result of sludge.
In empyema of the GB, ultrasonography may reveal calculi within the lumen of the GB. Occasionally, the impacted calculus may be identified. The GB may be distended and tender to pressure from the ultrasonographic probe. Within the GB lumen, gravity-dependent layering of pus, debris, or bile may be observed. Particulate matter may appear as bright medium to coarse echoes without shadowing.
With acute emphysematous cholecystitis, gas in the lumen of the GB is hyperreflective, with a distal reverberation artifact in the GB lumen. Intramural gas is characterized by hyperreflective foci in the GB wall, with or without a reverberation artifact. An effervescent GB may be seen; in such cases, a large number of bubbles rise from the dependent part of the GB like gas bubbles in a glass of champagne. The differential diagnosis includes various causes of pneumobilia.
The "effervescent gallbladder" sign refers to the finding of tiny echogenic foci rising from the dependent portion of the gallbladder, reminiscent of bubbles rising in a glass of champagne (see the video below). The sign has been described as pathognomonic for emphysematous cholecystitis; however, Niederhauser et al reported 2 cases with this finding in a patient with acute, gangrenous cholecystitis, confirmed in both cases by CT, secondary to the release of gas from gallstones. These 2 cases may cast doubt on the ultrasonographic sign as a pathognomonic finding of emphysematous cholecystitis. [16]
Diagnostic criteria
There are major and minor ultrasonographic diagnostic criteria for the diagnosis of AC. Two major or 1 major and 2 minor criteria need to be present to achieve a diagnosis. This classification is particularly useful with acute acalculous cholecystitis (AAC). The major criteria include the following:
-
GB-wall thickening of more than 3 mm
-
A striated GB wall
-
A positive sonographic Murphy sign
-
Mucosal sloughing
-
Pericholecystic fluid
-
Intramural gas
Minor criteria include sludge within the GB and GB dilatation of greater than 5 cm in transverse diameter. [17]
Degree of confidence
For the diagnosis of acute cholecystitis (AC), ultrasonography is rapid, noninvasive, affordable, and sensitive. Because ultrasonography may be performed at the bedside, it is particularly useful in making the diagnosis of AC in hospitalized patients, who may be very ill, dependent on a respirator, or recovering from surgery or various medical problems. The sensitivity and specificity of ultrasonography in the diagnosis of AC are 81-100% and 60-100%, respectively. [18]
Ultrasonography may be inaccurate in the diagnosis of AC in hospitalized patients, especially in patients who have acalculous cholecystitis. None of the ultrasonographic criteria for diagnosing AC (eg, cholelithiasis, thickened GB wall, nonshadowing echoes, sonolucent stripes, pericholecystic fluid) are specific. Differentiating acute cholecystitis from chronic cholecystitis is possible in only 26% of patients. In 74% of patients, therefore, it is not possible to differentiate between acute and chronic cholecystitis on the basis of ultrasonographic findings. AC is presumed to be present if ultrasonography reveals no other apparent cause of abdominal pain.
The ultrasonographic Murphy sign is present in only 33% of patients with acute gangrenous cholecystitis. When gas is prominent in cases of emphysematous cholecystitis, the GB may be mistaken for a bowel loop because of increased echogenicity and shadowing.
Differentials: GB-wall thickness
The following are causes of increased GB-wall thickness [19] :
-
Fasting (transient GB-wall thickening present in about 3.5% of fasting patients)
-
Poor distention (postprandial)
-
Artifact on oblique sections
-
Acute cholecystitis
-
Chronic cholecystitis
-
Carcinoma GB
-
Xanthogranulomatous cholecystitis
-
Acquired immunodeficiency syndrome
-
Hyperplastic cholesterolosis
-
GB varices
-
Adenomyomatosis
-
Leukemia-GB infiltration
-
GB perforation
-
GB torsion
-
Oriental cholangiohepatitis
-
Hepatic clonorchiasis
-
Cholecystenteric fistula
-
Focal obstruction to GB lymphatic drainage (eg, nodes at the porta)
-
Hepatitis (80%)
-
Cirrhosis
-
Acute alcoholic abuse (severe GB-wall thickening is often present after an alcoholic binge; may make the GB difficult to define)
-
Portal hypertension
-
Veno-occlusive disease
-
Congestive cholecystopathy in chronic liver disease
-
Hepatoportal sclerosis
-
Infectious mononucleosis
-
Extrinsic causes, systemic causes
-
Hypoproteinemia
-
Ascites
-
Acute pancreatitis
-
Acute myelogenous leukemia
-
Sepsis
-
Graft-versus-host reaction, bone marrow transplantation
-
Brucellosis
-
Systemic venous hypertension
-
Right-sided heart failure
-
Acute pyelonephritis (GB-wall thickening secondary to adjacent inflammatory process; similar to that seen in pancreatitis and peptic ulcer disease)
-
Renal failure
-
Myeloma
-
Appendicitis
-
Peptic ulcer disease
-
Infusion with interleukin-2 (IL-2) in HIV infection (symptomatic GB-wall thickening during IL-2 infusion may exactly mimic other forms of acalculous cholecystitis, except when IL-2–associated GB-wall thickness resolves after the cessation of therapy; surgical treatment not required)
Differentials: gallstones
Mimics of gallstones include the following [19] :
-
Partial volume effects, usually caused by impression by the duodenum
-
Misidentification of the GB
-
Fluid-filled bowel associated with gas, a hepatic or renal cyst, debris, hemorrhage, or a combination of these factors
-
Reverberation echoes from folds in the GB neck
-
Respiratory motion artifact (not usually a problem with real-time scanners)
-
Shadows arising directly anterior or posterior to the GB (eg, rib)
-
Junctional mucosal fold
-
Clips in the cholecystectomy bed (patients may be unable to remember having undergone previous cholecystectomy or may be unaware that GB has been removed)
-
Inspissated bile sludge, commonly seen in ill patients
-
Any cause of an intraluminal filling defect
-
Pseudosludge (the artifactual appearance of layering sludge caused by the section thickness and side-lobe artifact; these artifacts may be reduced by appropriate focusing, by centering the GB in the field of view, and by optimizing the gain settings)
-
Adenomyomatosis and cholesterolosis (forms of hyperplastic cholecystosis; usually asymptomatic, but symptoms may occur because of associated gallstones)
-
Emphysematous cholecystitis and porcelain GB (may cause patchy shadowing, which occasionally is present without associated gallstones; air and calcification echogenic and cause shadowing)
-
Echogenic bile (often associated with biliary stasis or bile duct obstruction; echogenicity varies, but usually no shadowing present)
-
Polyps within the GB (vary in size and echogenicity but do not show shadow; differentiation from adherent gallstones may be difficult)
-
Nonvisualization of the GB in a fasting patient
In the last item above, the presence of shadowing foci in the GB bed is strong presumptive evidence of GB disease. A wall-echo-shadow [WES] triad is useful in this setting; the complex consists of 2 parallel arcs of echogenic lines, with an interspaced anechoic space. The echogenic lines represent the GB wall and the leading edge of the gallstone separated by anechoic bile. The WES sign is useful in differentiating a contracted, diseased GB from other conditions with a similar appearance (eg, porcelain GB, emphysematous cholecystitis, air-filled bowel).
The ultrasonograms below were taken in a woman with severe, right hypochondriacal pain that mimicked gallstones.
Acute cholecystitis mimic. CT scan in a 36-year-old woman with severe right hypochondriacal pain. The gallbladder wall is thickened, with a suggestion of the triple wall sign. There is a streak of pericholecystic fluid at the inferior aspect of the gallbladder. An ultrasound for the Murphy sign was negative. No gallstones were seen. There were no predisposing causes of an acalculous acute cholecystitis. A supine CT scan showed signs of inflammation in the region of the duodenum, but the duodenal wall was not well seen. However, further CT scan sections in the right decubitus position showed spasm and thickening of the wall of the first part of the duodenum. Endoscopy revealed an acute penetrating duodenal ulcer.
Acute cholecystitis mimic. A 36-year-old woman with severe right hypochondriacal pain. The gallbladder wall is thickened, with a suggestion of the triple wall sign. There is a streak of pericholecystic fluid at the inferior aspect of the gallbladder. An ultrasound of the Murphy sign was negative. No gallstones were seen. There were no predisposing causes of an acalculous acute cholecystitis. A supine CT scan showed signs of inflammation in the region of the duodenum, but the duodenal wall was not well seen. However further CT scan sections in the right decubitus position showed spasm and thickening of the wall of the first part of the duodenum. Endoscopy revealed an acute penetrating duodenal ulcer.
The following nonshadowing, mobile, intraluminal GB masses may be present [19] :
-
Calculi
-
Tumefactive sludge
-
Cholesterol crystals
-
Pseudosludge, artifact
-
Food and/or feces
-
Blood
-
Pus
-
Fibrinous debris and/or desquamated mucosa
-
Ascaris lumbricoides
-
Clonorchis sinensis
-
Fasciola hepatica
-
Low-level echoes within the GB
-
Cholesterol crystals (small, but echogenic)
-
Multiple small calculi
-
Pus
-
Abnormal mucous
-
Parasites
-
Milk calcium bile or limy bile (echogenicity intermediate between that of sludge and calculi)
-
Concentration of bile
Other differentials
The concentration of bile in the fasting patient may give rise to sludge formation. This is slightly echogenic and does not cause shadowing, but it may form a bile/sludge level. The biochemical nature of sludge has been recognized to consist predominantly of aggregates of cholesterol crystals and liquid crystalline droplets. In some cases of obstructive jaundice and symptomatic liver disease, it is composed of bilirubin granules embedded in a gel matrix of mucous glycoproteins.
Biliary sludge is often associated with biliary stasis, as occurs in association with parenteral nutrition, fasting, pregnancy, and mucous hypersecretion (eg, mucin-secreting bile duct tumors). In most patients, the presence of sludge is a transient phenomenon; as the patient's condition improves, the sludge resolves. If the lumen of the GB is completely filled with sludge that has an echogenicity similar to that of the liver, the GB may not be seen; this process is called hepatization.
Causes of pericholecystic fluid include the following [19] :
-
Acute cholecystitis
-
Pericholecystic abscess
-
Subacute GB perforation
-
Gangrenous infarction of GB
-
Ascites
-
Pancreatitis
-
Peptic ulcer, with or without perforation
-
Liver abscess
-
Peritonitis
-
Ligamentum teres abscess
-
Ruptured hepatic adenoma
-
Ruptured ectopic gestation
-
Acquired immunodeficiency syndrome (AIDS)
-
Low-level echoes in the adjacent liver (eg, secondary to inflammation of the hepatic flexure of colon)
The lack of findings associated with AC and a clinical picture not suggestive of acalculous cholecystitis should suggest the possibility of other causes of pericholecystic fluid.
Nuclear Imaging
Technetium-99m iminodiacetic acid (99mTc-IDA) agents (disofenin and mebrofenin) are routinely used in the performance of cholescintigraphy (see the images below).
 Normal cholescintigrams. Normal technetium-99m hepatic iminodiacetic acid (99mTc-HIDA) scans of the liver shows normal gallbladder filling within 45 minutes.
Normal cholescintigrams. Normal technetium-99m hepatic iminodiacetic acid (99mTc-HIDA) scans of the liver shows normal gallbladder filling within 45 minutes.
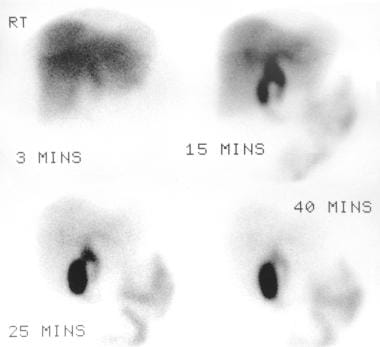
 Technetium-99m hepatic iminodiacetic acid (99mTc-HIDA) scan followed for 1 hour 30 minutes shows no filling of the gallbladder due to cystic duct obstruction.
Technetium-99m hepatic iminodiacetic acid (99mTc-HIDA) scan followed for 1 hour 30 minutes shows no filling of the gallbladder due to cystic duct obstruction.
After the intravenous injection, these compounds are rapidly bound to plasma proteins and are transported to the liver. There, the IDA compounds dissociate from their protein binding. After dissociation, the compounds are taken up by the hepatocytes through a carrier-mediated, non–sodium-dependent membrane transport mechanism. This is the same pathway as that of bilirubin. Therefore, when the serum bilirubin level increases, competition for the carrier molecules occurs, and biliary excretion of IDA compounds is diminished. [20]
Unlike bilirubin, IDA compounds do not undergo conjugation in the hepatocytes, and they are rapidly excreted into the bile. The compounds enable excellent visualization of the bile ducts and gallbladder (GB) within 30-60 minutes. Because AC is initiated by cystic duct obstruction, nonvisualization of the GB after the intravenous injection of 99mTc-IDA is better correlated with acute cholecystitis (AC) than is the detection of gallstones. Normally, the GB is visualized within 60 minutes after tracer injection. Visualization of the GB establishes cystic duct patency and excludes AC with only rare exceptions. Nonvisualization of the GB 3-4 hours after the injection because of cystic duct obstruction is characteristic of an AC.
Alternatively, morphine infusion may be used to shorten the examination time. Morphine increases tone in the sphincter of Oddi, increases CBD pressure, and results in a pressure differential between the CBD and the GB; this promotes tracer entry into the GB.
Nonvisualization of the GB 30 minutes after the morphine infusion suggests AC cholecystitis in the appropriate clinical setting. The rim sign indicates inflammatory spread into the adjacent liver parenchyma; in cases of AC, this is usually a sign that GB gangrene has set in, with or without perforation.
The efficacy of radionuclide angiography and cholescintigraphy in the diagnosis of cholecystitis has been investigated. In one study, radionuclide angiography and cholescintigraphy were performed with a bolus injection of 99mTc-disofenin in 65 patients with clinically suspected AC. AC was surgically confirmed in 23 of 25 patients who had positive radionuclide angiographic findings (a positive result was indicated by increased blood flow to the GB fossa).
Also in the study, severe AC and abscesses were present in 3 patients with a scintigraphically visible GB but with positive angiographic findings. All 20 patients for whom there were positive findings on radionuclide angiography and cholescintigraphy had transmural cholecystitis. Of the 9 patients with AC and false-negative angiographic findings, none had abscess or gangrene of the GB.
Radionuclide angiography may therefore allow the determination of AC severity. In one study, 9 of 25 patients with positive findings had gangrenous cholecystitis or a pericholecystic abscess. Positive findings on radionuclide angiograms may shorten the patient examination, and delayed images (>1 hr) may not be necessary.
Gallium-67 (67Ga) has been shown to accumulate in inflammatory and infective processes. In one study of 10 patients with cholecystitis who were examined with 67Ga scanning, images in 5 patients with AC showed significant accumulation in the GB.
Degree of confidence
Cholescintigraphy is highly sensitive in the diagnosis of AC, and it is especially valuable when ultrasonographic results are equivocal. The negative predictive value of a normal cholescintigram is greater than 98%. [21] The rim sign is not sensitive (35% sensitivity), but it is reasonably specific in cases of complicated cholecystitis; however, the specificity is not high enough to obviate delayed or postmorphine images. [21]
In a meta-analysis, cholescintigraphy displayed a sensitivity of 97% and a specificity of 90% for AC; by way of comparison, ultrasonography displayed a sensitivity of 91% and a specificity of 79%. Although cholescintigraphy is more accurate than ultrasonography, the latter has the advantages of allowing evaluation of all the abdominal structures (possibly enabling an alternative diagnosis for patients with right-upper-quadrant pain who do not have AC). In patients who do have AC, ultrasonography may provide anatomic information regarding gallbladder size, stone size, gallbladder wall thickness, and bile duct size.
Cholescintigraphy is less accurate in diagnosing acalculous AC than it is in diagnosing calculous AC. Sensitivities are 68-100%; specificities are 38-100%. Morphine administration may be particularly helpful in preventing false-positive results in patients with suspected acalculous AC. Use of cholecystokinin before the study causes the emptying of viscous bile from the gallbladder and helps to prevent false-positive results.
Although 67Ga scanning is noninvasive, it has not found acceptance in the diagnosis of AC.
Differentials and false positives
Spontaneous resolution of an acute cholecystitis (AC) may occur 5-7 days after onset of symptoms because of reestablishment of cystic duct patency. In such circumstances, the gallbladder (GB) may appear normal on cholescintigraphy. In a small number of patients with acalculous cholecystitis, GB visualization may be normal.
Most patients with acute acalculous cholecystitis (AAC), however, have a functional cystic duct obstruction as a result of vasculitis or edema; in these cases, GB visualization is unusual. The presence of tracer in the duodenal cap, dilation of the cystic duct, or a duodenal diverticulum may be misinterpreted as GB filling. In appearance, chronic cholecystitis and AC may be indistinguishable. In only 4-8% of cases is the GB not visualized. Especially in patients with symptomatic, chronic cholecystitis is the GB not visualized.
False-positive results with hepatic iminodiacetic acid (HIDA) scanning (eg, lack of GB visualization) are possible in association with the following:
-
Prolonged fasting (gallbladder full)
-
Total parenteral nutrition
-
Ingestion of food less than 1 hour before scanning
-
Acute pancreatitis
-
Hepatitis
-
Alcoholism
-
Cirrhosis
-
Gallbladder hydrops
-
Chronic cholecystitis
-
Postpartum state (speculative)
-
Hydatid cyst rupture into the biliary tree
Serial 67Ga scanning is needed to rule out gallium accumulation in the hepatic flexure of the colon, which is a potential cause of a false-positive result. The accumulation of 67Ga has also been reported in cases of chronic cholecystitis.
Angiography
Patients with acute cholecystitis (AC) are rarely examined with angiography. Historically, angiographic findings of AC have been described. Marked hypervascularity with dilatation of the cystic artery may be observed, but the inflammatory process also results in the acquisition of blood from the right hepatic arterial supply.
Arterial blush is present in association with an increase in the accumulation of contrast material in the gallbladder (GB), the GB fossa, and the associated inflammatory mass. In the subacute phase of disease, hypervascularity persists, but parenchymal accumulation of contrast material may occur early and may be prominent; in such cases, a thickened GB wall is apparent. GB veins are seldom seen when the GB is normal, but in the subacute stage of AC, the GB veins may be particularly prominent.
Degree of confidence
Angiography has no role in the diagnosis of acute cholecystitis. Angiography is an invasive procedure, and there are risks associated with the use of contrast material, with radiation exposure, and with other factors.
In addition, empyema of the GB may arise de novo or as a complication of acute cholecystitis; the angiographic findings may be similar to those seen in cases of subacute AC.
-
Plain abdominal radiograph of a 68-year-old woman who presented with acute abdominal pain. There are multiple calculi distributed in a pyriform shape in the right upper quadrant; these are suggestive of gallstones. Gallstones were diagnosed during sonography several months earlier. A clinical diagnosis of acute cholecystitis was made. However, the plain radiograph also shows features of a pneumoperitoneum. At laparotomy, a perforated cecal carcinoma was found. There were no findings of acute cholecystitis.
-
(Left) Plain radiograph of a 57-year-old woman presenting with right iliac fossa pain and mild fever shows large laminated opacities in the right iliac fossa (RIF); these findings suggest gallstones (arrow). Two smaller nonlaminated oval opacities are present more medially; these were interpreted as calculi in the cystic duct. Ultrasonography revealed a Reidel lobe of the liver. The gallbladder was located in the RIF and contained several calculi; however, no ultrasonographic features of acute cholecystitis were observed. The right kidney was also placed in the RIF, in a more medial location. Two calculi were present—one each in the upper and lower pole calices. (Right) Intravenous urogram shows a low-lying right kidney with calculi in the upper and lower pole calices. Urine culture revealed Escherichia coli. The patient's condition responded to a course of antibiotics. This example shows that an acute pyelonephritis can clinically mimic acute cholecystitis. With a Reidel lobe, the gallbladder may be located in the RIF, and an acute cholecystitis may mimic appendicitis or other RIF pathology.
-
Plain abdominal radiograph in a 49-year-old diabetic woman shows air within the gallbladder lumen due to emphysematous cholecystitis (arrow).
-
Plain abdominal radiograph in a patient with a clinical diagnosis of acute cholecystitis. The diagnosis was confirmed by means of abdominal ultrasonography. The radiograph shows faint opacities in the region of the gallbladder fossa and dilated loops of small bowel in the epigastrium and mid abdomen secondary to localized ileus.
-
This patient presented with acute cholecystitis, as confirmed at imaging. His pain resolved over a few days, but mildly elevated bilirubin levels persisted. Endoscopic retrograde cholangiopancreatographic (ERCP) study shows smooth narrowing of the bile duct (arrow) at the site of insertion of the cystic duct (Mirizzi syndrome). Note the small calculus in the cystic duct.
-
Longitudinal oblique sonogram through the gallbladder shows a calculus at the neck of the gallbladder with acoustic shadowing and thickening of the gallbladder wall (arrow).
-
Longitudinal and axial scans through the gallbladder show layering of sludge (S) in the gallbladder lumen.
-
Oblique and longitudinal sonograms through gallbladder shows marked laminated sonolucent thickening of the gallbladder wall, sludge, and edema (arrow).
-
Axial scan through the gallbladder shows marked thickening of the gallbladder wall, with the lumen of the gallbladder full of sludge.
-
This 26-year-old man known to be HIV positive presented with pain in the right upper quadrant and mild jaundice. Axial sonogram through the gallbladder and pancreas shows sludge within the gallbladder and the lower common bile duct (CBD). A diagnosis of acalculous cholecystitis was confirmed. Arrow indicates the CBD; A, aorta; GB, gallbladder; IVC, inferior vena cava; P, pancreas; and S, splenic vein.
-
Ultrasonogram of the gallbladder shows focal thickening of the gallbladder wall (arrow) that mimics a carcinoma.
-
Longitudinal oblique ultrasonogram through the gallbladder shows pseudomembrane formation due to sloughed mucosa. Note the small calculus.
-
Axial ultrasonogram through the gallbladder shows tiny calculi in the gallbladder and pericholecystic fluid.
-
Four scans of different orientations through the gallbladder shows gallbladder wall thickening, pseudomembrane formation, sludge, and pericholecystic fluid.
-
Ultrasonogram shows complete disorganization of the gallbladder and its fossa that mimics a gallbladder carcinoma.
-
Normal cholescintigrams. Normal technetium-99m hepatic iminodiacetic acid (99mTc-HIDA) scans of the liver shows normal gallbladder filling within 45 minutes.
-
Technetium-99m hepatic iminodiacetic acid (99mTc-HIDA) scan followed for 1 hour 30 minutes shows no filling of the gallbladder due to cystic duct obstruction.
-
Nonenhanced CT scans through the gallbladder (GB) shows an indistinct GB wall. Contrast-enhanced CT scan (bottom) shows an inflammatory reaction in the pericholecystic fat, which is seen as streaky or bandlike soft-tissue areas of attenuation extending from the GB wall into the surrounding fat. Note the loss of the interface between the GB and surrounding soft tissue on both the nonenhanced (top) and enhanced (bottom) scans. Note also the striking enhancement of GB and pericholecystic tissues following the use of intravenous contrast material.
-
Acute emphysematous cholecystitis. Color Doppler images of the gallbladder of an 82-year-old male with diabetes mellitus who presented with abdominal distention and vomiting. Ultrasound shows a markedly thickened gallbladder wall, which is hypervascularized. There are no gallstones, but note the presence of air in the anterior wall of the gallbladder (arrow).
-
Acute cholecystitis mimic. CT scan in a 36-year-old woman with severe right hypochondriacal pain. The gallbladder wall is thickened, with a suggestion of the triple wall sign. There is a streak of pericholecystic fluid at the inferior aspect of the gallbladder. An ultrasound for the Murphy sign was negative. No gallstones were seen. There were no predisposing causes of an acalculous acute cholecystitis. A supine CT scan showed signs of inflammation in the region of the duodenum, but the duodenal wall was not well seen. However, further CT scan sections in the right decubitus position showed spasm and thickening of the wall of the first part of the duodenum. Endoscopy revealed an acute penetrating duodenal ulcer.
-
Acute cholecystitis mimic. A 36-year-old woman with severe right hypochondriacal pain. The gallbladder wall is thickened, with a suggestion of the triple wall sign. There is a streak of pericholecystic fluid at the inferior aspect of the gallbladder. An ultrasound of the Murphy sign was negative. No gallstones were seen. There were no predisposing causes of an acalculous acute cholecystitis. A supine CT scan showed signs of inflammation in the region of the duodenum, but the duodenal wall was not well seen. However further CT scan sections in the right decubitus position showed spasm and thickening of the wall of the first part of the duodenum. Endoscopy revealed an acute penetrating duodenal ulcer.
-
Acute cholecystitis mimic. CT scan in a 36-year-old woman with severe right hypochondriacal pain. The gallbladder wall is thickened, with a suggestion of the triple wall sign. There is streak of pericholecystic fluid at the inferior aspect of the gallbladder. An ultrasound of the Murphy sign was negative. No gallstones were seen. There were no predisposing causes of an acalculous acute cholecystitis. A supine CT scan showed signs of inflammation in the region of the duodenum, but the duodenal wall was not well seen. However, further CT scan sections in the right decubitus position showed spasm and thickening of the wall of the first part of the duodenum. Endoscopy revealed an acute penetrating duodenal ulcer.
-
Acute cholecystitis mimic. CT scans in a 36-year-old woman with severe right hypochondriacal pain. The gallbladder wall is thickened with a suggestion of the triple wall sign. There is a streak of pericholecystic fluid at the inferior aspect of the gallbladder. An ultrasound of the Murphy sign was negative. No gallstones were seen. There were no predisposing causes of an acalculous acute cholecystitis. A supine CT scan showed signs of inflammation in the region of the duodenum, but the duodenal wall was not well seen. However, further CT scan sections in the right decubitus position showed spasm and thickening of the wall of the first part of the duodenum. Endoscopy revealed an acute penetrating duodenal ulcer.
-
Acute cholecystitis mimic. CT scans in a 36-year-old woman with severe right hypochondriacal pain. The gallbladder wall is thickened, with a suggestion of the triple wall sign. There is a streak of pericholecystic fluid at the inferior aspect of the gallbladder. An ultrasound of the Murphy sign was negative. No gallstones were seen. There were no predisposing causes of an acalculous acute cholecystitis. A supine CT scan showed signs of inflammation in the region of the duodenum, but the duodenal wall was not well seen. However, further CT scan sections in the right decubitus position showed spasm and thickening of the wall of the first part of the duodenum. Endoscopy revealed an acute penetrating duodenal ulcer.
-
Acute cholecystitis mimic. Ultrasound image of the gallbladder of a patient with acute lymphatic leukemia, showing marked gallbladder wall thickening with no clinical features of acute or chronic cholecystitis.
-
CT scan shows pearl gallstones and thickening of the gallbladder wall.
-
Line diagrams show a trocar method of cholecystostomy and placement of a pigtail catheter in the gallbladder lumen.
-
This video shows a rare but more specific finding: small, nonshadowing echogenic foci rising up from the dependent portions of the gallbladder lumen ("champagne sign," similar to effervescing bubbles in a glass of champagne).
Tables
| Local Inflammation Signs | Systemic Inflammation Signs | Imaging Findings |
|---|---|---|
| Murphy's sign | Fever | Imaging characteristic of acute cholecystitis |
| Right upper quadrant mass | Elevated C-reactive protein | |
| Right upper quadrant pain or tenderness | Elevated white blood count | |
| Suspected Diagnosis: 1 local inflammation sign and 1 systemic inflammation sign | ||
| Definite Diagnosis: 1 local inflammation sign, 1 systemic inflammation sign, and characteristic imaging findings | ||








