Practice Essentials
Cerebral venous thrombosis (venous sinus thrombosis; CVT) is caused by clots in the dural venous sinuses and accounts for 0.5% to 1% of all strokes. [1, 2] CVT results in an increased venous pressure that can lower cerebral perfusion pressure and induce parenchymal change due to vasogenic edema, cytotoxic edema, or notably intracranial hemorrhage. [3] The mainstay of treatment is long-term anticoagulation. [4]
Because cerebral venous thrombosis hormonal factors are implicated (primarily oral contraceptives) and pregnancy, over 70% of cases are in women. [2] The annual prevalence of CVT in women of childbearing age is estimated to be 3 in 100,000. [5] The greatest risk periods for CVT include the third trimester and the first month postpartum, with 73% of CVT cases in women occurring in the puerperium. The incidence of cerebral venous thrombosis during pregnancy and post partum ranges from 1 in 2500 deliveries to 1 in 10,000 deliveries in developed countries. [6]
CVT has been found to be a rare but life-threatening complication of COVID-19 infection. [7] Additionally, cases of CVT in combination with thrombocytopenia following COVID-19 vaccination have been reported. [8] Cerebral venous sinus thrombosis after adenovirus-vectored COVID-19 ChAdOx1 nCov-19 and Ad26.COV2.S is a rare complication that occurs mainly in individuals younger than 60 years and more frequently in women, manifesting 4-24 days after vaccination. The leading symptom is headache, but seizures, visual disturbances, focal neurologic symptoms, and increased intracranial pressure are also possible. On T2* (susceptibility-weighted) MR sequences, the thrombus causes regions of dark signal with associated susceptibility-induced signal loss (blooming). [9, 10, 11]
Imaging modalities
Cerebral venous thrombosis is an elusive diagnosis because of its nonspecific presentation and its numerous predisposing causes (see the images below). CVT cases have a more varied clinical presentation than other stroke types, and they rarely present as a stroke syndrome. Presentations include isolated headache, intracranial hypertension syndrome, seizures, a focal lobar syndrome, and encephalopathy. Because of the increased use of magnetic resonance imaging (MR) for investigating patients with acute and subacute headaches and new-onset seizures, CVT is being diagnosed with increasing frequency. The confirmation of the diagnosis of CVT relies on the demonstration of thrombi in the cerebral veins and/or sinuses by MRI/MR venography or CT venography. [12]
The current gold standard to detect CVT is the use of CT abd CT venography, or conventional MRI along with MR venography, particularly with dynamic time-resolved angiographic techniques. [2, 13, 14, 15]
Imaging can detect direct or indirect signs. Direct signs correspond to visualization of a thrombus or venous thrombosis, while indirect signs include cerebral ischemia or hemorrhage. If an aneurysm is suspected, CT angiography or arterial 3D time-of-flight (TOF) imaging should be performed, covering the posterior inferior cerebellar arteries to the callosal marginal arteries. If the patient has an unusual headache with neurologic or visual signs or confusion, MR venography should be performed, with 2D or 3D phase contrast and 2D TOF or 3D T1 elliptical post-gadolinium enhancement. [16, 2]
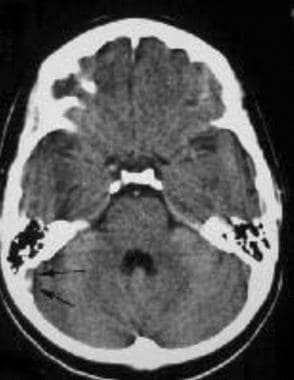 A 23-year-old woman with headache. CT scan demonstrates a subtle right transverse sinus thrombosis with high attenuation (arrows). No hemorrhagic infarction is seen.
A 23-year-old woman with headache. CT scan demonstrates a subtle right transverse sinus thrombosis with high attenuation (arrows). No hemorrhagic infarction is seen.
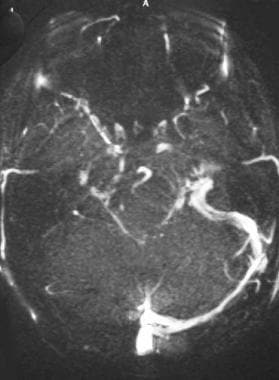 MR venography demonstrates absent flow in the right transverse sinus, sigmoid sinus, and internal jugular vein.
MR venography demonstrates absent flow in the right transverse sinus, sigmoid sinus, and internal jugular vein.
 Sagittal T1-weighted image demonstrates T1-hyperintense thrombus (arrows) within the superior sagittal sinus consistent with thrombus. Courtesy of James G. Smirniotopoulos and MedPix.
Sagittal T1-weighted image demonstrates T1-hyperintense thrombus (arrows) within the superior sagittal sinus consistent with thrombus. Courtesy of James G. Smirniotopoulos and MedPix.
Cerebral venous thrombosis often presents with hemorrhagic infarction in areas atypical for arterial vascular distribution. Magnetic resonance venography (MRV) in conjunction with conventional MRI can accurately diagnose cerebral venous thrombosis. With careful interpretation and a high degree of clinical suspicion, CT can also lead to a definitive diagnosis. [17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27] We have recently encountered an isolated case of cerebral venous sinus thrombosis wihtout assoicated venous infarction.
According to the European Stroke Organization (ESO), computed tomographic venography (CTV), magnetic resonance venography (MRV), and digital subtraction angiography (DSA) have similar accuracies in the diagnosis of CVT. The ESO guidelines noted that the advantages of CTV include rapid image acquisition and the fact that it is not necessarily contraindicated in patients with a pacemaker and ferromagnetic device. The benefits of MRI/MRV include the ability to show the thrombus itself and greater sensitivity in detecting parenchymal lesions. [16]
Clinical manifestations and physical findings may be nonspecific. The diagnosis may be made or suggested by CT brain scan before and after intravenous contrast medium injection. [12, 28, 29]
Two-dimensional time-of-flight (2D TOF) MRV is performed in the coronal plane; however, in-plane signal loss that mimics thrombosis may occur with this technique. Thus, a review of source data and conventional MRI brain scan is necessary. Phase-contrast MRV techniques may help, since small cortical venous infarcts may not be observed on 2D TOF MRV. [30]
For severe cases of cerebral venous sinus thrombosis, intravascular thrombolytic therapy can be performed within the affected sinus if conventional heparin therapy fails. [31] Localized thrombolysis during the postpartum period has also been successful. [32, 33]
Computed Tomography
The diagnosis of cerebral venous thrombosis (venous sinus thrombosis) occasionally can be made by CT scan with careful attention to the findings, which may be subtle (see the images below).
A 23-year-old woman with headache. CT scan demonstrates a subtle right transverse sinus thrombosis with high attenuation (arrows). No hemorrhagic infarction is seen.
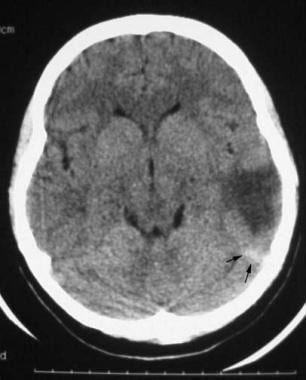
 A noncontrast CT image located demonstrates thrombus (arrows) extending along the course of the right transverse sinus.
A noncontrast CT image located demonstrates thrombus (arrows) extending along the course of the right transverse sinus.
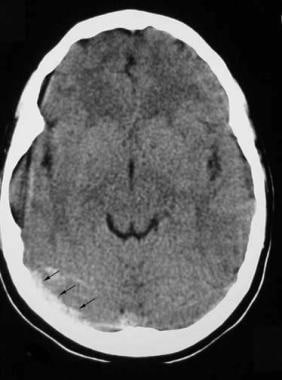
 A 32-year-old postpartum patient with headaches. Axial CT image shows a hypodense left temporal lobe venous infarct. A triangular high-attenuation focus (arrows) posterolateral to the area of infarction represents thrombus within the left transverse sinus.
A 32-year-old postpartum patient with headaches. Axial CT image shows a hypodense left temporal lobe venous infarct. A triangular high-attenuation focus (arrows) posterolateral to the area of infarction represents thrombus within the left transverse sinus.
Diagnostic findings include the following:
-
On noncontrast CT scan, the classic finding is the delta sign, which is observed as a dense triangle (from hyperdense thrombus) within the superior sagittal sinus. However, this is not specific, since high attenuation in the healthy nonthrombosed sinus can be observed occasionally and is common in neonates because of an elevated hematocrit. [34]
-
On contrast-enhanced CT scan, the reverse delta sign (ie, empty triangle sign) can be observed in the superior sagittal sinus from enhancement of the dural leaves surrounding the comparatively less dense thrombosed sinus.
-
The presence of both the delta and reverse delta signs increases the likelihood of the diagnosis.
-
On CT brain scan, infarctions in a nonarterial distribution in the white matter and/or cortical white matter junction, often associated with hemorrhage, should suggest the possible diagnosis of venous thrombosis. Bilateral cerebral involvement can occur, including the superior cerebral white matter of the convexities from superior sagittal sinus thrombosis, or the basal ganglia and thalami from internal cerebral vein thrombosis in which the internal cerebral veins appear hyperdense in the noncontrast scan.
-
Indirect CT signs include focal cerebral cortical ischemia with gyral enhancement, small ventricles compressed by cerebral edema, and intense tentorial enhancement. Occasionally, the transcerebral medullary cortical veins can be observed.
A 320-detector-row CT perfusion imaging scanner is capable of visualizing changes in the blood flow of the entire brain, including posterior circulation structures as well as cortical areas close to the vertex. In a retrospective review of 10 patients diagnosed with acute CVT who underwent CT perfusion as a part of the imaging evaluation, perfusion maps were analyzed including cerebral blood volume (CBV), cerebral blood flow (CBF), mean transit time, and time to peak. In this study, 9 had perfusion abnormalities. All perfusion abnormalities were localized in areas adjacent to the occluded sinus and did not match typical anterior or posterior circulation arterial territories. Bilateral perfusion deficits were seen in 4 cases. In 2 cases, parenchymal hemorrhage was diagnosed on noncontrast CT imaging; in those cases, focal CBV and CBF were reduced. The researchers concluded that whole-brain CT perfusion imaging can assist in establishing the diagnosis of CVT by detecting perfusion abnormalities corresponding to venous and not arterial territories. CT perfusion could assist in the differentiation between focal reversible changes, such as those caused by vasogenic edema, and irreversible changes due to infarction. [35]
In a study of non-contrast CT to diagnose CVT, Bonatti et al found that this modality had 81% sensitivity, 77% specificity, 78% positive predictive value, and 80% negative predictive value. [36]
Limitations
The characteristic CT scan appearances and signs strongly suggest cerebral venous thrombosis, but CT scans are seldom conclusively diagnostic. Because of the subtlety of the findings, the prospective diagnosis of venous thrombosis may not be made unless a high index of suspicion is maintained during interpretation of the CT study. CT venography also can confirm the diagnosis [37] and does not suffer from the in-plane flow artifact that causes signal loss on 2-dimensional time-of-flight (2D TOF) magnetic resonance venography (MRV).
A false-positive delta sign may occur in a trauma setting because of an adjacent subdural hematoma. The dural sinus normally may appear hyperdense relative to adjacent tissues. Both the delta and reverse delta signs may need to be present to establish the diagnosis of cerebral venous thrombosis (venous sinus thrombosis). Occasionally, the superior sagittal sinus may bifurcate proximal to the torcular herophili, resulting in a confluens sinuum and an empty delta sign without the presence of a venous thrombosis.
In most patients, MRI brain scan with MRV or CT with CT venography is recommended to establish the diagnosis. Cerebral arteriography and venography may be necessary when MRI scan and MRV are not available.
Magnetic Resonance Imaging
MRI in conjunction with magnetic resonance venography (MRV) is both sensitive and specific enough to provide the best noninvasive method of diagnosing cerebral venous thrombosis (see the images below).
MR venography demonstrates absent flow in the right transverse sinus, sigmoid sinus, and internal jugular vein.
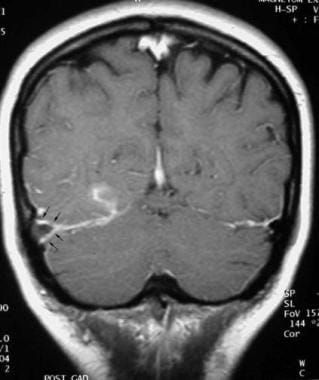 Postgadolinium T1-weighted image demonstrates enhancement of the dura surrounding the right transverse sinus thrombosis and right occipital lobe enhancement in the area of ischemic brain. Following heparin therapy, the right transverse sinus recanalized. One year later, the MR venogram was normal with no residual T2 hyperintensity in the right occipital lobe.
Postgadolinium T1-weighted image demonstrates enhancement of the dura surrounding the right transverse sinus thrombosis and right occipital lobe enhancement in the area of ischemic brain. Following heparin therapy, the right transverse sinus recanalized. One year later, the MR venogram was normal with no residual T2 hyperintensity in the right occipital lobe.
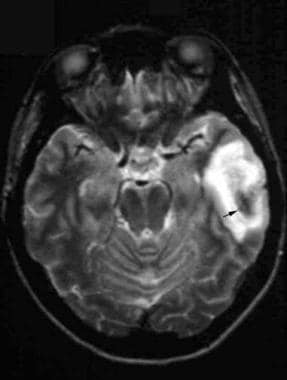 Axial T2-weighted image reveals left temporal lobe T2 hyperintensity consistent with infarction and a central focus of T2 hypointensity (arrow) due to the susceptibility effect of blood in a deoxyhemoglobin phase. Venous infarction is possible and is frequently hemorrhagic. Gradient-echo axial images are more sensitive to hemorrhagic products.
Axial T2-weighted image reveals left temporal lobe T2 hyperintensity consistent with infarction and a central focus of T2 hypointensity (arrow) due to the susceptibility effect of blood in a deoxyhemoglobin phase. Venous infarction is possible and is frequently hemorrhagic. Gradient-echo axial images are more sensitive to hemorrhagic products.
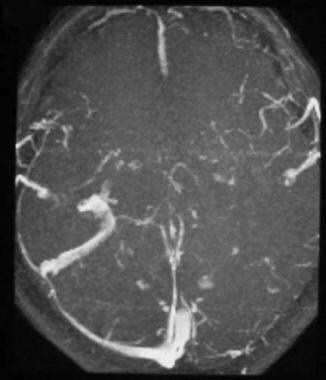 Axial MR venogram demonstrates occlusion of the left transverse sinus, sigmoid sinus, and internal jugular vein.
Sagittal T1-weighted image demonstrates T1-hyperintense thrombus (arrows) within the superior sagittal sinus consistent with thrombus. Courtesy of James G. Smirniotopoulos and MedPix.
Axial MR venogram demonstrates occlusion of the left transverse sinus, sigmoid sinus, and internal jugular vein.
Sagittal T1-weighted image demonstrates T1-hyperintense thrombus (arrows) within the superior sagittal sinus consistent with thrombus. Courtesy of James G. Smirniotopoulos and MedPix.
The diagnosis usually can be made without intravenous contrast, although contrast enhancement can aid in confirming the diagnosis. [21, 38, 39, 40, 41] A thrombus can be directly visualized within a vessel. Secondary venous infarctions and foci of hemorrhage can be seen with gradient-echo images. Susceptibility-induced signal loss from deoxyhemoglobin provides a basis for detection of even small foci of hemorrhage, which tend to occur in the subcortical white matter, thalami, and basal ganglia.
Parenchymal regions of T2-hyperintense signal abnormality in the distribution of the draining sinus is often observed and may be reversible, even when large. This may occur independent of recanalization of the thrombosed vessels. Dilated venous collaterals, such as transcortical medullary veins, provide indirect evidence of venous thrombosis. The appearance of intravenous thrombus on conventional MRI depends on the age of the blood clot within the vessel.
In acute venous thrombosis, loss of flow void on T1-weighted images occurs along with hypointensity on T2-weighted images, making the determination of sinus occlusion difficult. In the subacute phase, blood clot can result in loss of normal flow void on T1-weighted images and T1 hyperintensity; conversely, on T2-weighted images, blood clot can be of low signal intensity, thus mimicking flowing blood. In this instance, blood is in the intracellular methemoglobin stage.
Flow-related enhancement phenomena created by slow flow can occur in veins and cause T1 hyperintensity. To circumvent this problem, flow-sensitive imaging techniques can be used (ie, 2-dimensional time-of-flight [2D TOF] or phase-contrast MRV) to accurately assess the venous sinuses; 2D TOF MRV pulse sequence is sensitive to slow flow. Maximum signal is produced when blood flows orthogonal to the imaging plane, and since many cerebral veins course in an anteroposterior direction, coronal acquisition is often used with an inferior saturation pulse to eliminate arterial signal.
Restricted diffusion may or may not be seen in cerebral venous thrombosis and, when present, may occasionally be reversible. [42] Partially recanalized chronic venous sinus thrombosis has been described to demonstrate intense enhancement of the thrombosed segments following intravenous gadolinium-based contrast agents. A case report of restricted diffusion in the optic nerves bilaterally has been described in the setting of cavernous sinus thrombosis.
The role of the fibrin-specific MR contrast agent EP-2104R, which is based on gadolinium, has been postulated to bind only to fibrin and not to circulating fibrinogen and has been demonstrated in animal models to be highly selective for cerebral sinus vein thrombosis. This agent may indicate a developing role for molecular imaging. [22]
Pffefferkorn et al studied 32 patients with cerebral venous thrombosis, and they found that the most frequent parenchymal MRI finding was thalamic edema (69% of patients; bilateral in 47%). [43]
Kang and colleagues examined the arterial spin-labeling perfusion-weighted image (ASL-PWI) of 13 patients with confirmed CVT and found bright signal in dural sinus termed “bright sinus appearance” in all (100%) and hypoperfusion in brain parenchyma drained by thrombosed sinus in 10 (70%). This study demonstrated that bright sinus appearance on ASL-PWI had higher sensitivity for identifying cerebral venous thrombosis than the findings on conventional MRI of susceptibility vessel sign, empty delta sign, and atypical distribution against arterial territory (with differences of 15%; P = .500, 46%; P = .031, and 50%; P = .031, respectively). [3]
Hakim et al measured the diagnostic accuracy of high-resolution 3D T2 sampling perfection with application-optimized contrasts by using different flip angle evolution in patients with cerebral venous sinus thrombosis and found that accuracy, sensitivity, and specificity were 100% each in 35 patients (63 MRI exams). [44]
Limitations
Variants of venous anatomy are common, and a hypoplastic sinus or prominent arachnoid granulations may simulate venous sinus thrombosis. With 2D TOF MRV techniques, thrombus in the intracellular or extracellular methemoglobin stage can present with increased signal and falsely simulate blood flow. Phase-contrast MRV may avoid this error.
Hypoplasia or severe attenuation of a transverse sinus, which are normal anatomic variants, may simulate venous sinus thrombosis. In-plane flow-induced signal loss in 2D TOF MRV also can mimic intravenous thrombus. Prominent arachnoid granulations may simulate thrombus. A careful review of the MRV images and conventional MRI may lead to the correct diagnosis.
Ultrasonography
In general, ultrasonography is not useful for cerebral venous thrombosis (venous sinus thrombosis). Better noninvasive modalities include MRI with MRV and CT venography. As with other imaging modalities, differentiation of the normal anatomic variant of hypoplastic sinus from a thrombosed sinus can be difficult with ultrasonography. In neonates, however, the diagnosis of venous sinus thrombosis may be made by color Doppler ultrasound. An isolated case diagnosed with power Doppler was reported in the literature. [45, 46]
A published series from Germany reported 14 patients with transverse sinus thrombosis studied by transcranial color duplex ultrasonography and concluded that without contrast media administration, ultrasonography is "almost useless." [47]
The use of Levovist imaging agent (ie, transpulmonary stable microbubbles formed in galactose suspension) results in a signal increase of 25 dB and offers improved diagnostic capability.
Angiography
Prior to the advent of MRI, the diagnosis of cerebral venous thrombosis (venous sinus thrombosis) was confirmed by contrast arteriography.
Classic findings include the following:
-
Filling defects from thrombus within the venous sinus
-
Occlusion of a draining sinus
Secondary indirect angiographic findings are as follows:
-
Decreased focal venous circulation around a thrombosed venous sinus
-
Visualization of collateral circulation
-
Narrowing of arteries in the involved region
-
Prolonged contrast blush in the brain parenchyma
-
Tortuous vessels in the capillary and venous phases
-
Collateral flow in dilated anastomotic vessels
-
A 23-year-old woman with headache. CT scan demonstrates a subtle right transverse sinus thrombosis with high attenuation (arrows). No hemorrhagic infarction is seen.
-
A noncontrast CT image located demonstrates thrombus (arrows) extending along the course of the right transverse sinus.
-
MR venography demonstrates absent flow in the right transverse sinus, sigmoid sinus, and internal jugular vein.
-
Postgadolinium T1-weighted image demonstrates enhancement of the dura surrounding the right transverse sinus thrombosis and right occipital lobe enhancement in the area of ischemic brain. Following heparin therapy, the right transverse sinus recanalized. One year later, the MR venogram was normal with no residual T2 hyperintensity in the right occipital lobe.
-
A 32-year-old postpartum patient with headaches. Axial CT image shows a hypodense left temporal lobe venous infarct. A triangular high-attenuation focus (arrows) posterolateral to the area of infarction represents thrombus within the left transverse sinus.
-
Axial T2-weighted image reveals left temporal lobe T2 hyperintensity consistent with infarction and a central focus of T2 hypointensity (arrow) due to the susceptibility effect of blood in a deoxyhemoglobin phase. Venous infarction is possible and is frequently hemorrhagic. Gradient-echo axial images are more sensitive to hemorrhagic products.
-
Axial MR venogram demonstrates occlusion of the left transverse sinus, sigmoid sinus, and internal jugular vein.
-
Sagittal T1-weighted image demonstrates T1-hyperintense thrombus (arrows) within the superior sagittal sinus consistent with thrombus. Courtesy of James G. Smirniotopoulos and MedPix.







