Practice Essentials
Cardiopulmonary resuscitation (CPR) consists of the use of chest compressions and artificial ventilation to maintain circulatory flow and oxygenation during cardiac arrest (see the images below). Although survival rates and neurologic outcomes are poor for patients with cardiac arrest, early appropriate resuscitation—including early defibrillation when needed—and appropriate implementation of post–cardiac arrest care lead to improved survival and neurologic outcomes.
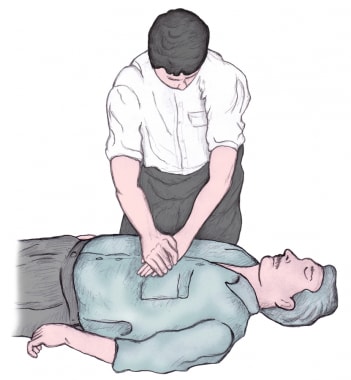 Delivery of chest compressions. Note the overlapping hands placed on the center of the sternum, with the rescuer's arms extended. Although it may be difficult to tell from the illustration, the rescuer's elbows should be locked out. Chest compressions are to be delivered at a rate of 100 to 120 per minute. The rescuer should push as hard as needed to attain a depth of each compression of 2 inches, and should allow complete chest recoil between each compression ('2 inches down, all the way up'). The rescuer should minimize any interruptions in compressions.
Delivery of chest compressions. Note the overlapping hands placed on the center of the sternum, with the rescuer's arms extended. Although it may be difficult to tell from the illustration, the rescuer's elbows should be locked out. Chest compressions are to be delivered at a rate of 100 to 120 per minute. The rescuer should push as hard as needed to attain a depth of each compression of 2 inches, and should allow complete chest recoil between each compression ('2 inches down, all the way up'). The rescuer should minimize any interruptions in compressions.
 Delivery of mouth-to-mouth ventilations. Avoid excessive ventilation. If no advanced airway, 30:2 compression-ventilation ratio. That is, perform 30 compressions and then 2 breaths.
Delivery of mouth-to-mouth ventilations. Avoid excessive ventilation. If no advanced airway, 30:2 compression-ventilation ratio. That is, perform 30 compressions and then 2 breaths.
Indications and contraindications
CPR should be performed immediately on any person who has become unconscious and is found to be pulseless.
Assessment of cardiac electrical activity via rapid rhythm strip recording can provide a more detailed analysis of the type of cardiac arrest, as well as indicate additional treatment options.
Loss of effective cardiac activity is generally due to the spontaneous initiation of a nonperfusing arrhythmia, sometimes referred to as a malignant arrhythmia. The most common nonperfusing arrhythmias include the following:
-
Pulseless bradycardia
Although prompt defibrillation has been shown to improve survival for VF and pulseless VT rhythms, [1] CPR should be started before the rhythm is identified and should be continued while the defibrillator is being applied and charged. Additionally, CPR should be resumed immediately after a defibrillatory shock until a pulsatile state is established. This is supported by studies showing that preshock pauses in CPR result in lower rates of defibrillation success and patient recovery. [2]
In a study involving out-of-hospital cardiac arrests in Seattle, 84% of patients regained a pulse when defibrillated during VF. [3] Defibrillation is generally most effective the faster it is deployed.
The American College of Surgeons, the American College of Emergency Physicians, the National Association of EMS Physicians, and the American Academy of Pediatrics have issued guidelines on the withholding or termination of resuscitation in pediatric out-of-hospital traumatic cardiopulmonary arrest. [4] Recommendations include the following:
-
Withholding resuscitation should be considered in cases of penetrating or blunt trauma victims who will obviously not survive.
-
Standard resuscitation should be initiated in arrested patients who have not experienced a traumatic injury.
-
Victims of lightning strikes or drowning with significant hypothermia should be resuscitated.
-
Children who showed signs of life before traumatic CPR should be taken immediately to the emergency department; CPR should be performed, the airway should be managed, and intravenous or intraosseous lines should be placed en route.
-
In cases in which the trauma was not witnessed, it may be assumed that a longer period of hypoxia might have occurred and limiting CPR to 30 minutes or less may be considered.
-
When the circumstances or timing of the traumatic event are in doubt, resuscitation can be initiated and continued until arrival at the hospital.
-
Terminating resuscitation in children should be included in state protocols.
Contraindications
The only absolute contraindication to CPR is a do-not-resuscitate (DNR) order or other advanced directive indicating a person’s desire to not be resuscitated in the event of cardiac arrest. A relative contraindication to performing CPR is if a physician justifiably believes that the intervention would be medically futile. This is an area of active research. [5, 6]
Equipment
CPR, in its most basic form, can be performed anywhere without the need for specialized equipment. Universal precautions (ie, gloves, mask, gown) should be taken. However, CPR is delivered without such protections in the vast majority of patients who are resuscitated in the out-of-hospital setting. Some hospitals and EMS systems employ devices to provide mechanical chest compressions. A cardiac defibrillator provides an electrical shock to the heart via 2 electrodes placed on the patient’s torso and may restore the heart into a normal perfusing rhythm.
Technique
In its full, standard form, CPR comprises the following 3 steps, performed in order:
-
Chest compressions
-
Airway
-
Breathing
For lay rescuers, compression-only CPR (COCPR) is recommended.
Positioning for CPR is as follows:
-
CPR is most easily and effectively performed by laying the patient supine on a relatively hard surface, which allows effective compression of the sternum
-
Delivery of CPR on a mattress or other soft material is generally less effective
-
The person giving compressions should be positioned high enough above the patient to achieve sufficient leverage, so that he or she can use body weight to adequately compress the chest
For an unconscious adult, CPR is initiated as follows:
-
Give 30 chest compressions
-
Perform the head-tilt chin-lift maneuver to open the airway and determine if the patient is breathing
-
Before beginning ventilations, look in the patient’s mouth for a foreign body blocking the airway
Chest compression
The provider should do the following:
-
Place the heel of one hand on the patient’s sternum and the other hand on top of the first, fingers interlaced
-
Extend the elbows and the provider leans directly over the patient (see the image below)
-
Press down, compressing the chest at least 2 in
-
Release the chest and allow it to recoil completely
-
The compression depth for adults should be at least 2 inches (instead of up to 2 inches, as in the past)
-
The compression rate should be at least 100-120/min
-
The key phrase for chest compression is, “Push hard and fast”
-
Untrained bystanders should perform chest compression–only CPR (COCPR)
-
After 30 compressions, 2 breaths are given; however, an intubated patient should receive continuous compressions while ventilations are given (8-10 ventilations per minute for an intubated adult patient)
-
This process is repeated until a pulse returns or the patient is transferred to definitive care
-
To prevent provider fatigue or injury, new providers should rotate onto the chest every 2-3 minutes (ie, providers should swap out, giving the previous chest compressor a rest while another rescuer continues CPR
Ventilation
If the patient is not breathing, 2 ventilations are given via the provider’s mouth or a bag-valve-mask (BVM). If available, a barrier device (pocket mask or face shield) should be used.
To perform the BVM or invasive airway technique, the provider does the following:
-
Ensure a tight seal between the mask and the patient’s face
-
Squeeze the bag with one hand for approximately 1 second, forcing at least 500 mL of air into the patient’s lungs
To perform the mouth-to-mouth technique, the provider does the following:
-
Pinch the patient’s nostrils closed to assist with an airtight seal
-
Put the mouth completely over the patient’s mouth
-
After 30 chest compression, give 2 breaths (the 30:2 cycle of CPR)
-
Give each breath for approximately 1 second with enough force to make the patient’s chest rise
-
Failure of the chest to rise with ventilation indicates an inadequate mouth seal or airway occlusion
-
After giving the 2 breaths, resume the CPR cycle
Complications
Complications of CPR include the following:
-
Fractures of ribs or the sternum from chest compression
-
Gastric insufflation from artificial respiration using noninvasive ventilation methods (eg, mouth-to-mouth, BVM); this can lead to regurgitation, with further airway compromise or aspiration; insertion of an invasive airway (eg, endotracheal tube) prevents this problem
ACLS
In the in-hospital setting or when a paramedic or other advanced provider is present, ACLS guidelines call for a more robust approach to treatment of cardiac arrest, including the following:
-
Drug interventions
-
ECG monitoring
-
Defibrillation
-
Invasive airway procedures
Emergency cardiac treatments no longer recommended include the following:
-
Routine atropine for pulseless electrical activity (PEA)/asystole
-
Cricoid pressure (with CPR)
-
Airway suctioning for all newborns (except those with obvious obstruction)
Background
For patients with cardiac arrest, survival rates and neurologic outcomes are poor, though early appropriate resuscitation, involving cardiopulmonary resuscitation (CPR), early defibrillation, and appropriate implementation of post–cardiac arrest care, leads to improved survival and neurologic outcomes. Targeted education and training regarding treatment of cardiac arrest directed at emergency medical services (EMS) professionals as well as the public has significantly increased cardiac arrest survival rates. [7]
CPR consists of the use of chest compressions and artificial ventilation to maintain circulatory flow and oxygenation during cardiac arrest. A variation of CPR known as “hands-only” or “compression-only” CPR (COCPR) consists solely of chest compressions. This variant therapy is receiving growing attention as an option for lay providers (that is, nonmedical witnesses to cardiac arrest events).
The relative merits of standard CPR and COCPR continue to be widely debated. An observational study involving more than 40,000 patients concluded that standard CPR was associated with increased survival and more favorable neurologic outcomes than COCPR was. [8] However, other studies have shown opposite results, and it is currently accepted that COCPR is superior to standard CPR in out-of-hospital cardiac arrest.
Several large randomized controlled and prospective cohort trials, as well as one meta-analysis, demonstrated that bystander-performed COCPR leads to improved survival in adults with out-of-hospital cardiac arrest, in comparison with standard CPR. [9, 10, 11] Differences between these results may be attributable to a subgroup of younger patients arresting from noncardiac causes, who clearly demonstrate better outcomes with conventional CPR. [8]
The 2010 revisions to the American Heart Association (AHA) CPR guidelines state that untrained bystanders should perform COCPR in place of standard CPR or no CPR (see American Heart Association CPR Guidelines). [12]
Of the more than 300,000 cardiac arrests that occur annually in the United States, survival rates are typically lower than 10% for out-of-hospital events and lower than 20% for in-hospital events. [13, 14, 15, 16, 17] A study by Akahane et al suggested that survival rates may be higher in men but that neurologic outcomes may be better in women of younger age, though the reasons for such sex differences are unclear. [18]
Additionally, studies have shown that survival falls by 10-15% for each minute of cardiac arrest without CPR delivery. [19, 20] Bystander CPR initiated within minutes of the onset of arrest has been shown to improve survival rates 2- to 3-fold, as well as improve neurologic outcomes at 1 month. [21, 22]
It has also been demonstrated that out-of hospital cardiac arrests occurring in public areas are more likely to be associated with initial ventricular fibrillation (VF) or pulseless ventricular tachycardia (VT) and have better survival rates than arrests occurring at home. [23]
This article focuses on CPR, which is just one aspect of resuscitation care. Other interventions, such as the administration of pharmacologic agents, cardiac defibrillation, invasive airway procedures, post–cardiac arrest therapeutic hypothermia, [24, 25, 26, 27, 28] the use of echocardiography in resuscitation, [29] and various diagnostic maneuvers, [30, 31] are beyond the scope of this article. For more information, see the Resuscitation Resource Center; for specific information on the resuscitation of neonates, see Neonatal Resuscitation.
See the guidelines sections detailed later in the article.
Indications & Contraindications
Indications
CPR should be performed immediately on any person who has become unconscious and is found to be pulseless.
Assessment of cardiac electrical activity via rapid rhythm strip recording can provide a more detailed analysis of the type of cardiac arrest, as well as indicate additional treatment options.
Loss of effective cardiac activity is generally due to the spontaneous initiation of a nonperfusing arrhythmia, sometimes referred to as a malignant arrhythmia. The most common nonperfusing arrhythmias include the following:
-
Pulseless bradycardia
Although prompt defibrillation has been shown to improve survival for VF and pulseless VT rhythms, [1] CPR should be started before the rhythm is identified and should be continued while the defibrillator is being applied and charged. Additionally, CPR should be resumed immediately after a defibrillatory shock until a pulsatile state is established. This is supported by studies showing that preshock pauses in CPR result in lower rates of defibrillation success and patient recovery. [2]
In a study involving out-of-hospital cardiac arrests in Seattle, 84% of patients regained a pulse when defibrillated during VF. [3] Defibrillation is generally most effective the faster it is deployed.
The American College of Surgeons, the American College of Emergency Physicians, the National Association of EMS Physicians, and the American Academy of Pediatrics have issued guidelines on the withholding or termination of resuscitation in pediatric out-of-hospital traumatic cardiopulmonary arrest. [4] Recommendations include the following:
-
Withholding resuscitation should be considered in cases of penetrating or blunt trauma victims who will obviously not survive.
-
Standard resuscitation should be initiated in arrested patients who have not experienced a traumatic injury.
-
Victims of lightning strikes or drowning with significant hypothermia should be resuscitated.
-
Children who showed signs of life before traumatic CPR should be taken immediately to the emergency department; CPR should be performed, the airway should be managed, and intravenous or intraosseous lines should be placed en route.
-
In cases in which the trauma was not witnessed, it may be assumed that a longer period of hypoxia might have occurred and limiting CPR to 30 minutes or less may be considered.
-
When the circumstances or timing of the traumatic event are in doubt, resuscitation can be initiated and continued until arrival at the hospital.
-
Terminating resuscitation in children should be included in state protocols.
Contraindications
The only absolute contraindication to CPR is a do-not-resuscitate (DNR) order or other advanced directive indicating a person’s desire to not be resuscitated in the event of cardiac arrest. A relative contraindication to performing CPR is if a physician justifiably believes that the intervention would be medically futile. This is an area of active research. [5, 6]
Preparation
Anesthesia
Because a person in cardiac arrest is almost invariably unconscious, anesthetic agents are not typically required for cardiopulmonary resuscitation (CPR).
Equipment
CPR, in its most basic form, can be performed anywhere without the need for specialized equipment. Regardless of the equipment available, proper technique (see Technique) is essential.
Universal precautions (ie, gloves, mask, gown) should be taken. However, in the vast majority of patients who are resuscitated in the out-of-hospital setting, CPR is delivered without such protections.
Some hospitals and emergency medical services (EMS) systems employ devices to provide mechanical chest compressions, although until relatively recently, such devices had not been shown to be more effective than high-quality manual compressions. [32] One study has shown increased survival with better neurologic outcome in patients receiving active compression-decompression CPR with augmentation of negative intrathoracic pressure (achieved with an impedance threshold device), compared with patients receiving standard CPR. [33]
In a meta-analysis of 12 studies, mechanical chest compression devices proved superior to manual chest compressions in the ability to achieve return of spontaneous circulation. In the meta-analysis, Westfall and colleagues found that devices that use a distributing band to deliver chest compression (load-distributing band CPR) was significantly superior to manual CPR (odds ratio, 1.62), while the difference between piston-driven CPR devices and manual resuscitation did not reach significance (odds ratio, 1.25) [34] This finding was supported by a study conducted by Pinto et al. [35]
Additionally, other health systems have begun to implement devices to monitor CPR electronically and provide audiovisual CPR feedback to providers, thereby helping them improve the quality of compressions during CPR. [2, 36, 37, 38]
An Advanced Cardiac Life Support (ACLS) provider (ie, physician, nurse, paramedic) may also elect to insert an endotracheal tube directly into the trachea of the patient (intubation), which provides the most efficient and effective ventilations. However, 2 retrospective cohort studies have called into question the value of prehospital endotracheal intubation. [39, 40] Further study in this area is warranted.
An additional device employed in the treatment of cardiac arrest is a cardiac defibrillator. This device provides an electrical shock to the heart via 2 electrodes placed on the patient’s chest and can restore the heart into a normal perfusing rhythm.
Positioning
CPR is most easily and effectively performed by laying the patient supine on a relatively hard surface, which allows effective compression of the sternum. Delivery of CPR on a mattress or other soft material is generally less effective.
The health care provider giving compressions should be positioned high enough above the patient to achieve sufficient leverage, so that he or she can use body weight to adequately compress the chest (see the video below).
In the hospital setting, where patients are in gurneys or beds, appropriate positioning is often achieved by lowering the bed, having the CPR provider stand on a step-stool, or both. In the out-of-hospital setting, the patient is often positioned on the floor, with the CPR provider kneeling over him or her.
Technique
Overview
In its full, standard form, cardiopulmonary resuscitation (CPR) comprises 3 steps: chest compressions, airway, and breathing (CAB), to be performed in that order in accordance with American Heart Association (AHA) guidelines.
Note that artificial respirations are no longer recommended for bystander rescuers; thus, lay rescuers should perform compression-only CPR (COCPR). Healthcare providers, however, should perform all 3 components of CPR (chest compressions, airway, and breathing).
For an unconscious adult, CPR is initiated using 30 chest compressions. Perform the head-tilt chin-lift maneuver to open the airway and determine if the patient is breathing. Before beginning ventilations, rule out airway obstruction by looking in the patient’s mouth for a foreign body blocking the patient’s airway. CPR in the presence of an airway obstruction results in ineffective ventilation/oxygenation and may lead to worsening hypoxemia.
The techniques described here refer specifically to CPR as prescribed by the Basic Cardiac Life Support (BCLS) guidelines. In the in-hospital setting, or when a paramedic or other advanced provider is present in the out-of-hospital setting, Advanced Cardiac Life Support (ACLS) guidelines call for a more robust approach to treatment of cardiac arrest, including drug interventions, electrocardiographic (ECG) monitoring, defibrillation, and invasive airway procedures.
Attempting to perform CPR is better than doing nothing at all, even if the provider is unsure if he or she is doing it correctly. This especially applies to many people’s aversion to providing mouth-to-mouth ventilations. If one does not feel comfortable giving ventilations, chest compressions alone are still better than doing nothing.
Chest compression
The heel of one hand is placed on the patient’s sternum, and the other hand is placed on top of the first, fingers interlaced. The elbows are extended and the provider leans directly over the patient (see the image below). The provider presses down, compressing the chest at least 2 in. The chest is released and allowed to recoil completely (see the video below).
Delivery of chest compressions. Note the overlapping hands placed on the center of the sternum, with the rescuer's arms extended. Although it may be difficult to tell from the illustration, the rescuer's elbows should be locked out. Chest compressions are to be delivered at a rate of 100 to 120 per minute. The rescuer should push as hard as needed to attain a depth of each compression of 2 inches, and should allow complete chest recoil between each compression ('2 inches down, all the way up'). The rescuer should minimize any interruptions in compressions.
With the hands kept in place, the compressions are repeated 30 times at a rate of 100/min. The key thing to keep in mind when doing chest compressions during CPR is to push fast and hard. Care should be taken to not lean on the patient between compressions, as this prevents chest recoil and worsens blood flow.
After 30 compressions, 2 breaths are given (see Ventilation). Of note, an intubated patient should receive continuous compressions while ventilations are given 8-10 times per minute. This entire process is repeated until a pulse returns or the patient is transferred to definitive care.
When done properly, CPR can be quite fatiguing for the provider. If possible, in order to give consistent, high-quality CPR and prevent provider fatigue or injury, new providers should intervene every 2-3 minutes (ie, providers should swap out, giving the chest compressor a rest while another rescuer continues CPR).
For COCPR (ie, CPR without rescue breaths), the provider delivers only the chest compression portion of care at a rate of 100/min to a depth of 38-51 mm (1-1.5 in.) without pause. This delivery of compressions continues until the arrival of medical professionals or until another rescuer is available to continue compressions. [9]
The use of mechanical CPR devices was reviewed in three large trials. Outcomes were similar between mechanical devices and manual compressions. The studies did not recommend routinely replacing manual compressions with mechanical CPR devices, but they did not rule out a role for the mechanical devices if high-quality manual chest compression is not available. [41]
Ventilation
If the patient is not breathing, 2 ventilations are given via the provider’s mouth (see the image below) or a bag-valve-mask (BVM).
Delivery of mouth-to-mouth ventilations. Avoid excessive ventilation. If no advanced airway, 30:2 compression-ventilation ratio. That is, perform 30 compressions and then 2 breaths.
The mouth-to-mouth technique is performed as follows (see the video below):
-
The nostrils of the patient are pinched closed to assist with an airtight seal
-
The provider puts his mouth completely over the patient’s mouth
-
The provider gives a breath for approximately 1 second with enough force to make the patient’s chest rise
Effective mouth-to-mouth ventilation is determined by observation of chest rise during each exhalation. Failure to observe chest rise indicates an inadequate mouth seal or airway occlusion. As noted (see above), 2 such exhalations should be given in sequence after 30 compressions (the 30:2 cycle of CPR). When breaths are completed, compressions are restarted. If available, a barrier device (pocket mask or face shield) should be used.
More commonly, health care providers use a BVM, which forces air into the lungs when the bag is squeezed. Several adjunct devices may be used with a BVM, including oropharyngeal and nasopharyngeal airways.
The BVM or invasive airway technique is performed as follows:
-
The provider ensures a tight seal between the mask and the patient’s face.
-
The bag is squeezed with one hand for approximately 1 second, forcing at least 500 mL of air into the patient’s lungs.
Next, the provider checks for a carotid or femoral pulse. If the patient has no pulse, chest compressions are begun.
Post Procedure
Complications
Performing chest compressions may result in the fracturing of ribs or the sternum, although the incidence of increased mortality from such fractures is widely considered to be low. [42]
Artificial respiration using noninvasive ventilation methods (eg, mouth-to-mouth, bag-valve-mask [BVM]) can often result in gastric insufflation. This can lead to vomiting, which can further lead to airway compromise or aspiration. The problem is eliminated by inserting an invasive airway, which prevents air from entering the esophagus.
CPR and ECC Guidelines Summary
Updated cardiopulmonary resuscitation (CPR) and/or emergency cardiovascular care (ECC) guidelines were issued in 2020 by the American Heart Association (AHA) and International Liaison Committee on Resuscitation (ILCOR), and in 2020-2021 by the European Resuscitation Council (ERC).
American Heart Association
The AHA's CPR guidelines are updated every 5 years and have transitioned to a new online format for continuous evidence evaluation since 2015.
The 2020 guidelines include recommendations in the following areas [43] :
-
Adult basic and advanced life support
-
Pediatric basic and advanced life support
-
Neonatal resuscitation
-
Resuscitation education science
-
Systems of care
European Resuscitation Council
The ERC guidelines provide detailed algorithms and recommendations in 10 areas, which are updated and published approximately every 5 years in separate papers. The 2021 guidelines cover the following areas [44] :
-
Epidemiology of cardiac arrest in Europe
-
Systems saving lives
-
Adult BLS
-
Adult ACLS
-
Cardiac arrest in special circumstances
-
Postresuscitation care
-
First aid
-
Neonatal resuscitation
-
Pediatric life support
-
Education for resuscitation
-
Ethics of resuscitation and end-of-life decisions
The International Liaison Committee on Resuscitation
Initially formed in 1993, the ILCOR includes representatives from the AHA, the ERC, the Heart and Stroke Foundation of Canada, the Australian and New Zealand Committee on Resuscitation, the Resuscitation Council of Southern Africa, the InterAmerican Heart Foundation, and the Resuscitation Council of Asia. The ILCOR defines emergency cardiac care as “all responses necessary to treat sudden life-threatening events affecting the cardiovascular and respiratory systems, with a particular focus on sudden cardiac arrest.” [45]
Like the AHA and ERC guidelines, the ILCOR guidelines are updated on a 5-year cycle and include consensus treatment recommendations in the following areas [46] :
-
Adult BLS
-
Adult ACLS, including post–cardiac arrest care
-
Acute coronary syndromes
-
Pediatric BLS and ALS
-
Neonatal resuscitation
-
Education, implementation, and teams
-
First aid
Chain of Survival Guidelines
The 2020 update added a 'Recovery' link to the chain of survival for both in-hospital cardiac arrests (IHCAs) and out-of-hospital cardiac arrests (OHCAs). [43]
Table 1. Adult Chain of Survival (Open Table in a new window)
Link 1 |
Link 2 |
Link 3 |
Link 4 |
Link 5 |
Link 6 | |
IHCA |
Early recognition and prevention |
Activation of the emergency response system |
Immediate high-quality CPR |
Rapid defibrillation |
Advanced life support and post-arrest care |
Recovery |
Responder(s) |
Primary Provider |
Code Team |
Cath Lab/ICU |
|||
OHCA |
Recognition and activation of the emergency response system |
Immediate high-quality CPR |
Rapid defibrillation |
Basic and advanced emergency medical services |
Advanced life support and post-arrest care |
Recovery |
Responder(s) |
Lay Rescuers |
Emergency Medical Services (EMS) | ED/Cath Lab/ICU | |||
ILCOR and ERC do not separate in-hospital from out-of-hospital cardiac arrest in their definition of chain of survival, and, therefore, they do not have the IHCA’s link 1 of surveillance and prevention. Otherwise they have similar chains of survival. [47, 45]
Postresuscitation care recommendations were added back in the 2015 update as a new section in collaboration with the European Society of Intensive Care Medicine. These postresuscitation care guidelines acknowledge the importance of high-quality postresuscitation care as a vital link in the chain of survival. [48]
Adult BLS and AED Guidelines
The AHA adult basic life support (BLS) algorithm reflects the widespread use of mobile telephones that can be used for assistance without leaving the patient. The algorithm is detailed in Table 2, below. [49]
Table 2. Adult BLS Algorithm (Open Table in a new window)
Untrained Lay Responders |
Trained Lay Responders |
Healthcare Professionals |
|
Step 1 |
Ensure scene safety |
||
Step 2 |
Check for response |
||
Step 3 |
Responder should shout for nearby help and phone or have another bystander phone 9-1-1; the phone should remain on speaker for receiving further instructions from the dispatcher. |
Responder should shout for nearby help and activate the emergency response system (9-1-1, emergency response). Ensure that the phone remains on speaker, if at all possible. |
Responder should shout for nearby help. The resuscitation team can be activated now or after checking breathing and pulse. |
Step 4 |
Follow dispatcher’s instructions. |
Check for no breathing or only gasping; if there is none, begin CPR with chest compressions. |
Check for no breathing or only gasping and check for a pulse (ideally should be done simultaneously). Activation and retrieval of the AED/emergency equipment by either the lone healthcare provider or by a second person must occur immediately after a check of breathing and pulse identifies cardiac arrest. |
Step 5 |
As instructed by dispatcher to check for no breathing or only gasping. |
Answer dispatcher’s questions and follow subsequent instructions. |
Begin CPR immediately, and use AED/defibrillator if available. |
Step 6 |
Follow dispatcher’s instructions. |
Send another person for an AED, if one is available. |
With arrival of a second responder, two-person CPR is provided and AED/defibrillator is used. |
The AHA 2010 guidelines revised the initial CPR sequence of steps from ABC (airway, breathing, chest compressions) to CAB (chest compressions, airway, breathing) [50] ; this was reaffirmed in subsequent updates, which also offered the following revised recommendations for performance of CPR [49] :
-
Chest compressions should be performed at a rate of 100-120/min (class I)
-
During manual CPR, chest compressions should be at a depth of at least 2 inches for an average adult, while avoiding excessive chest compression depths (>2.4 inches) (class I)
-
Total preshock and postshock pauses in chest compressions should be as short as possible (class I)
-
For adults in cardiac arrest receiving CPR without an advanced airway, it is reasonable to pause compressions for less than 10 seconds to deliver two breaths (class IIa)
-
In adult cardiac arrest with an unprotected airway, it may be reasonable to perform CPR, in which case, the chest compression target fraction should still be as high as possible (at least 60%) (class IIb)
Class I recommendations specifically for lay responders include the following [51] :
-
Untrained responders should provide compression-only CPR, with or without dispatcher assistance
-
Compression-only CPR should continue until the arrival of an AED or responders with additional training
-
All responders should, at a minimum, provide chest compressions for victims of cardiac arrest; in addition, if a trained lay responder is able to perform rescue breaths, they should be added in a ratio of 30 compressions to two breaths
Recommendations specifically for dispatchers include the following [51] :
-
Emergency dispatchers should be educated to identify unresponsiveness with abnormal breathing and agonal gasps across a range of clinical presentations and descriptions (class I)
-
After acquiring the requisite information to determine the location of the event, dispatchers should determine whether a patient is unresponsive with abnormal breathing (class I); if the caller reports that the patient is unresponsive with abnormal or no breathing, it is reasonable to assume the patient is in cardiac arrest (class IIa)
-
To increase bystander performance of CPR, telephone instructions on compression-only CPR should be provided to callers reporting an unresponsive adult who is not breathing or not breathing normally (ie, only gasping) (class I)
-
Dispatchers should instruct responders to provide CPR if the victim is unresponsive with no normal breathing, even when the victim demonstrates occasional gasps (class I)
-
Review of the quality of dispatcher CPR instructions provided to specific callers is an important component of a high-quality lifesaving program (class IIb)
Although the guideline recommends that dispatchers ask only about responsiveness and breathing, cardiac arrest is defined physiologically by the lack of a detectable pulse. For example, a person who is post-ictal may be unresponsive and have abnormal breathing, yet have a completely normal heart and normal pulse. Therefore, one should consider simultaneous detection of pulse if possible.
The guidelines recommend a simultaneous, choreographed approach to the performance of chest compressions, airway management, rescue breathing, rhythm detection, and shocks (if indicated) by an integrated team of highly trained rescuers in applicable settings. [51] Additional recommendations specifically for EMS and other healthcare providers include the following [51] :
-
If the patient is unresponsive with no breathing or only gasping, the patient should be assumed to be in cardiac arrest and the emergency response system should be immediately activated (class I)
-
If a pulse is not definitely felt within 10 seconds, chest compressions should be initiated (class IIa)
-
It is reasonable for healthcare providers to provide chest compressions and ventilation for all adult patients in cardiac arrest, from either a cardiac or noncardiac cause (class IIa) (However, note that chest compression must pause during rhythm analysis by an AED.)
-
Rapid defibrillation is the treatment of choice for ventricular fibrillation of short duration for victims of witnessed OHCA or for IHCA in a patient whose heart rhythm is monitored (class I)
-
For a witnessed OHCA with a shockable rhythm, it may be reasonable for EMS systems with priority-based, multitiered response to delay positive-pressure ventilation for up to three cycles of 200 continuous compressions with passive oxygen insufflation and airway adjuncts (class IIb)
-
Routine use of passive ventilation techniques during conventional CPR for adults is not recommended (class III); in EMS systems that use bundles of care involving continuous chest compressions, the use of passive ventilation techniques may be considered as part of that bundle (class IIb)
-
When the victim has an advanced airway in place during CPR, rescuers need no longer deliver cycles of 30 compressions and two breaths (ie, interrupt compressions to deliver breaths); instead, it may be reasonable for one rescuer to deliver one breath every 6 seconds (10 breaths per minute) while another rescuer performs continuous chest compressions (class IIb)
To open the airway in victims with suspected spinal injury, lay rescuers should initially use manual spinal motion restriction (eg, placing their hands on the sides of the patient’s head to hold it still) rather than immobilization devices, because use of immobilization devices by lay rescuers may be harmful (class III). For healthcare providers and others trained in two-person CPR, if there is evidence of trauma that suggests spinal injury, a jaw thrust without head tilt should be used to open the airway (class IIb)
There are no significant differences in the recommendations from ERC or ILCOR. [47, 52]
Adult ACLS Guidelines
Although management of cardiac arrest begins with BLS and progresses sequentially through the links of the chain of survival, there is some overlap as each stage of care progresses to the next. Generally, in the three guidelines, advanced cardiovascular life support (ACLS) comprises the level of care between basic life support (BLS) and post–cardiac arrest care. Recommendations for adult BLS and ACLS are combined in the 2020 guidelines. [43]
The following summarizes the 2020 AHA adult cardiac arrest algorithm [43] :
-
0. Activate emergency response system
-
1a. Initiate CPR and give oxygen when available
-
1b. Attach monitor/defibrillator/AED as soon as possible
-
2. If shockable rhythm (VF, pVT), defibrillate (shock) once. Use the manufacturer's device-specific recommendation (eg, 120-200 J for biphasic waveform and 360 J for monophasic waveform); if unknown, use the maximum available energy setting.
-
3a. Resume CPR immediately without pulse check and continue for five cycles. One cycle of CPR equals 30 compressions and two breaths; five cycles of CPR should take roughly 2 minutes (compression rate 100-120 per minute); do not check for rhythm/pulse until five cycles of CPR are completed.
-
3b. Secure IV (preferred) or IO access. During CPR, minimize interruptions while securing IV access.
-
3c. After 5 cycles (2 min) of CPR, recheck for a pulse and the rhythm.
-
4. If shockable rhythm (VF, pVT), defibrillate (shock) once. Use an equal or greater energy setting than the previous defibrillation.
-
5a. Resume CPR immediately without pulse check and continue for five cycles.
-
5b. Give epinephrine every 3-5 minutes.
-
5c. Consider advanced airway. Consider capnography. If intubation is elected, minimize interruptions while performing endotracheal intubation. Once the patient is intubated, continue CPR at 100-120 compressions per minute without pauses for respirations, and ventilate at 10 breaths per minute.
-
5d. After 5 cycles (2 min) of CPR, recheck for a pulse and the rhythm.
-
6. If shockable rhythm (VF, pVT), defibrillate (shock) once. Use an equal or greater energy setting than the previous defibrillation.
-
7a. Continue CPR.
-
7b. Give amiodarone (first dose 300 mg, second dose half that) or lidocaine (first dose 1-1.5 mg/kg, second dose half that).
-
7c. Treat reversible causes, if present.
Go to '3c' above.
If no shockable rhythm (and no pulse):
-
7d. Continue CPR.
-
7e. Treat reversible causes, if present.
Go to '9b' below.
If no shockable rhythm (PEA, asystole):
-
9a. Give epinephrine as soon as possible. Then give epinephrine every 3-5 minutes.
-
9b. Resume CPR immediately without pulse check and continue for five cycles. One cycle of CPR equals 30 compressions and two breaths; five cycles of CPR should take roughly 2 minutes (compression rate 100-120 per minute); do not check for rhythm/pulse until five cycles of CPR are completed.
-
9c. Secure IV (preferred) or IO access. During CPR, minimize interruptions while securing IV access. Consider advanced airway. Consider capnography. If intubation is elected, minimize interruptions while performing endotracheal intubation. Once the patient is intubated, continue CPR at 100-120 compressions per minute without pauses for respirations, and ventilate at 10 breaths per minute.
-
9d. After 5 cycles (2 min) of CPR, recheck for a pulse and the rhythm.
If shockable rhythm (VF, pVT), Go to '4' above.
If no shockable rhythm (and no pulse):
-
10a. Continue CPR.
-
10b. Treat reversible causes, if present.
Go to '9b' above.
If signs of return of spontaneous circulation (ROSC), Go to Post–Cardiac Arrest Care.
Note that for defibrillation, it is important to make sure the pads are correctly placed.
Reversible causes of adult cardiac arrest include the following:
-
Hypovolemia
-
Hypoxia
-
Hydrogen ion (acidosis): Consider bicarbonate therapy
-
Hyperkalemia/hypokalemia and metabolic disorders
-
Hypoglycemia: Check fingerstick or administer glucose
-
Hypothermia: Check core rectal temperature
-
Tension pneumothorax: Consider thoracostomy
-
Tamponade, cardiac: Check with ultrasonography
-
Toxins
-
Thrombosis, coronary or pulmonary: Consider thrombolytic therapy
AHA recommendations regarding termination of resuscitation in OHCA
According to the AHA, if termination of resuscitation (TOR) is being considered, BLS providers should use the BLS TOR rule where ALS is not available or will be delayed, and it is reasonable for ALS providers to use the adult ALS TOR rule in the field.
The BLS TOR rule recommends TOR when all of the following three criteria apply before moving to the ambulance for transport:
-
Arrest was not witnessed by EMS providers or first responder
-
No ROSC obtained
-
No shocks were delivered
The 2020 AHA guidelines note that in a recent meta-analysis of seven published studies (33,795 patients), only 0.13% (95% confidence interval [CI], 0.03-0.58%) of patients who fulfilled the BLS termination criteria survived to hospital discharge. [43]
The ALS TOR rule recommends TOR when all of the following criteria apply before moving to the ambulance for transport:
-
Arrest was not witnessed
-
No bystander CPR was provided
-
No ROSC after full ALS care in the field
-
No AED shocks were delivered
The 2020 AHA guidelines note that in a recent meta-analysis of two published studies (10,178 patients), only 0.01% (95% CI, 0.00-0.07%) of patients who fulfilled the ALS termination criteria survived to hospital discharge. [43]
Defibrillation
AHA recommendations for defibrillation include the following [49] :
-
Use defibrillators (using , or monophasic waveforms) to treat atrial and ventricular arrhythmias (class I)
-
Defibrillators using biphasic waveforms (BTE or RLB) are preferred (class IIa)
-
Use a single-shock strategy (as opposed to stacked shocks) for defibrillation (class IIa)
Adjuncts for airway control and ventilation
The AHA guidelines provide the following recommendations for airway control and ventilation [49] :
-
Advanced airway placement in cardiac arrest should not delay initial CPR and defibrillation for cardiac arrest
-
If advanced airway placement will interrupt chest compressions, consider deferring insertion of the airway until the patient fails to respond to initial CPR and defibrillation attempts or demonstrates return of spontaneous circulation
-
The routine use of cricoid pressure in cardiac arrest is not recommended (class III)
-
Either a bag-mask device or an advanced airway may be used for oxygenation and ventilation during CPR in both the in-hospital and out-of-hospital setting (class IIb); t
-
For healthcare providers trained in their use, either a supraglottic airway (SGA) device or an may be used as the initial advanced airway during CPR (class IIb)
-
Providers who perform endotracheal intubation should undergo frequent retraining (class I)
-
To facilitate delivery of ventilations with a bag-mask device, oropharyngeal airways can be used in unconscious (unresponsive) patients with no cough or gag reflex and should be inserted only by trained personnel (class IIa)
-
In the presence of known or suspected basal skull fracture or severe coagulopathy, an oral airway is preferred
-
Continuous waveform capnography in addition to clinical assessment is the most reliable method of confirming and monitoring correct placement of an ETT (class I)
-
If continuous waveform capnometry is not available, a nonwaveform carbon dioxide detector, esophageal detector device, and ultrasound used by an experienced operator are reasonable alternatives (class IIa)
-
Automatic transport ventilators (ATVs) can be useful for ventilation of adult patients in noncardiac arrest who have an advanced airway in place in both out-of-hospital and in-hospital settings (class IIb)
The recommendations from ERC or ILCOR do not differ significantly from those of the AHA. [53, 54]
Medication management
AHA guidelines offer the following recommendations for the administration of drugs during cardiac arrest [49] :
-
Amiodarone may be considered for or pVT that is unresponsive to CPR, defibrillation, and a vasopressor; lidocaine may be considered as an alternative (class IIb)
-
Routine use of magnesium for VF/pVT is not recommended in adult patients, other than in torsades de pointes/polymorphic VT with a long QT interval (class III)
-
Inadequate evidence exists to support routine use of lidocaine; however, the initiation or continuation of lidocaine may be considered immediately after ROSC from cardiac arrest due to VF/pVT (class IIb)
-
Inadequate evidence exists to support the routine use of a beta-blocker after cardiac arrest; however, the initiation or continuation of a beta-blocker may be considered after hospitalization from cardiac arrest due to VF/pVT (class IIb)
-
Atropine during pulseless electrical activity (PEA) or asystole is unlikely to have a therapeutic benefit (class IIb)
-
There is insufficient evidence for or against the routine initiation or continuation of other antiarrhythmic medications after ROSC from cardiac arrest
-
Standard-dose epinephrine (1 mg every 3-5 min) may be reasonable for patients in cardiac arrest (class IIb); high-dose epinephrine is not recommended for routine use in cardiac arrest (class III)
-
Vasopressin has been removed from the Adult Cardiac Arrest Algorithm and offers no advantage in combination with epinephrine or as a substitute for standard-dose epinephrine (class IIb)
-
It may be reasonable to administer epinephrine as soon as feasible after the onset of cardiac arrest due to an initial nonshockable rhythm (class IIb)
Post–Cardiac Arrest Care Guidelines
The 2020 AHA guidelines reaffirmed recommendations from the 2015 AHA Guidelines Update for CPR and ECC about treatment of hypotension, titrating oxygen to avoid both hypoxia and hyperoxia, detection and treatment of seizures, and targeted temperature management.
According to the AHA guidelines, although the best hospital care for patients with ROSC after cardiac arrest is not completely known, a comprehensive, structured, multidisciplinary system of care should be implemented in a consistent manner for the treatment of post–cardiac arrest patients (class I). Components of structured interventions include the following [49] :
-
Therapeutic hypothermia
-
Optimization of hemodynamics and gas exchange
-
Immediate coronary reperfusion, when indicated for restoration of coronary blood flow, with percutaneous coronary intervention (PCI)
-
Glycemic control
-
Neurological diagnosis, management, and prognostication
The key issues and major changes in the 2015 AHA guidelines update for post–cardiac-arrest care include the following [49] :
-
Emergency coronary angiography is recommended for all patients with ST elevation and for hemodynamically or electrically unstable patients without ST elevation in whom a cardiovascular lesion is suspected; the decision to perform revascularization should not be affected by the patient’s neurological status, which can change
-
Targeted temperature management (TTM) with a range of acceptable temperatures from 32-36˚C is recommended (at least for the first 24 h).
-
Identification and correction of hypotension is recommended in the immediate post–cardiac-arrest period
-
Prognostication no sooner than 72 hours after the completion of TTM
The following summarizes the AHA algorithm for adult immediate post‒cardiac arrest care after ROSC [49] :
-
Optimize ventilation and oxygenation
-
Treat hypotension
-
Perform a 12-lead ECG to determine whether acute ST elevation or ischemia is present
-
For ST-elevation myocardial infarction (STEMI), perform coronary reperfusion with PCI
-
TTM
Targeted temperature management
The 2010 AHA guidelines strongly advised induced hypothermia (32-34˚C) for patients with out-of-hospital VF/pVT cardiac arrest and post-ROSC coma (the absence of purposeful movements) and encouraged consideration of induced hypothermia for most other comatose patients after cardiac arrest. However, the precise duration and optimal temperature targets were unknown.
Because a range of temperatures is used, the term “targeted temperature management” (TTM) has been adopted. This term encompasses both induced hypothermia and active control of temperature at any target. [49]
The reaffirmed (from 2015) 2020 recommendations for TTM included the following [49] :
-
TTM for comatose adult patients with ROSC (class I)
-
A constant temperature of 32-36°C during TTM (class I)
-
TTM for at least 24 hours after achieving target temperature (class IIa)
-
Routine prehospital cooling of patients after ROSC with rapid infusion of cold IV fluids is not recommended (class III)
-
Prevention of fever in comatose patients after TTM may be reasonable (class IIb)
Management of seizures
The detection and treatment of nonconvulsive status epilepticus remains a priority.
Neuroprognostication
The 2020 AHA guidelines note that the timing for prognostication is typically greater than 72 hours after ROSC for patients treated with TTM. However, the guidelines acknowledge that withdrawal of life support may occur before 72 hours because of underlying terminal disease, brain herniation, or other clearly nonsurvivable situations. [49]
Additional recommendations for the timing of prognostication include the following [49] :
-
Clinical examination results may be used for prognostication in patients treated with TTM, where sedation or paralysis could be a confounder, in a minimum of 72 hours after completion of TTM (class IIb)
-
In patients not treated with TTM, 72 hours after cardiac arrest is the earliest time to prognosticate a poor neurologic outcome using clinical examination (class I)
-
Time until prognostication can be longer than 72 hours after cardiac arrest if the residual effect of sedation or paralysis confounds the clinical examination (class IIa)
The ERC guidelines indicate that poor outcome is very likely in patients who are unconscious for 72 hours or more after ROSC and have one or both of the following [48] :
-
No pupillary and corneal reflexes
-
Bilaterally absent N20 somatosensory-evoked potential (SSEP) wave
If neither of those are present, the ERC recommends waiting at least 24 hours. At that point, poor outcome is very likely in patients with two or more of the following:
-
Status myoclonus 48 hours or less after ROSC
-
High neuron-specific enolase
-
Status epilepticus on EEG
-
Diffuse anoxic injury on brain CT/MRI
Organ donation
All three guidelines recommend that all patients who are resuscitated from cardiac arrest but subsequently progress to death or brain death be evaluated for organ donation. [49, 48, 54] In addition, the AHA guidelines recommend considering kidney or liver donation in patients who do not have ROSC after resuscitation efforts and would otherwise have termination of efforts. [49]
Pediatric BLS and ACLS Guidelines
AHA guidelines on initiating CPR
As with the adult BLS recommendations, the AHA 2010 guidelines revised the initial CPR sequence of steps from ABC (airway, breathing, chest compressions) to CAB (chest compressions, airway, breathing). [50] This change was reaffirmed in the 2020 update, which states "It may be reasonable to initiate CPR with compressions-airway-breathing over airway breathing-compressions." [43]
The AHA 2020 guidelines also recommend that (1) lay rescuers should begin CPR for any victim who is unresponsive, not breathing normally, and does not have signs of life; do not check for a pulse and (2) in infants and children with no signs of life, it is reasonable for healthcare providers to check for a pulse for up to 10 seconds and begin compressions unless a definite pulse is felt. [43]
AHA guidelines algorithm for pediatric BLS
For lay rescuers
Step 1. Make sure the scene is safe. Check to see if the person is awake and breathing normally.
Step 2. If not, shout for help.
-
If you are alone and have a cell phone, call 911 then perform CPR (30 compressions:2 breaths) for 5 cycles (~2 minutes), then get an AED.
-
If you are alone and do not have a cell phone, perform CPR (30 compressions:2 breaths) for 5 cycles (~2 minutes), then get an AED.
-
If two or more people are available to help, one person calls 911 and then gets an AED, while the other person performs CPR (30 compressions:2 breaths).
Step 3. Repeat cycles of CPR (30 compressions:2 breaths); use AED as soon as it arrives.
For single healthcare providers on scene
Step 1. Make sure the scene is safe. Check to see if the person is awake and breathing normally.
Step 2. If not, shout for help. Activate 911.
Step 3. Look for no breathing or only gasping and (simultaneously) check for a DEFINITE pulse WITHIN 10 SECONDS.
3b. If pulse and normal breathing, monitor until EMS arrives.
3c. If pulse but NO normal breathing:
-
Provide rescue breathing, at 1 breath every 2-3 seconds, or about 20-30 breaths/min.
-
Assess pulse rate for no more than 10 seconds. If the heartrate is less than 60 beats/min with signs of poor perfusion, begin CPR. Otherwise, continue rescue breathing at 1 breath every 2-3 seconds, or about 20-30 breaths/min. Recheck the pulse every 2 minutes.
3d. If no pulse or normal breathing AND a witnessed sudden collapse, call 911, then go get an AED, then use the AED and perform CPR (30 compressions:2 breaths).
3e. If no pulse and NOT witnessed sudden collapse:
-
If you are alone: perform CPR (30 compressions:2 breaths) for 5 cycles (~2 minutes), then call 911 and go get an AED.
-
If two or more people are available to help, one person calls 911 and then gets an AED, while the other person performs CPR (30 compressions:2 breaths).
Step 4. Use AED as soon as it is available. If shock is advised, give 1 shock. Resume CPR immediately for 2 minutes (until prompted by AED to allow rhythm check). Continue until ALS providers take over or the person starts to move.
For two or more healthcare providers on scene
Step 1. Make sure the scene is safe. Check to see if the person is awake and breathing normally.
Step 2. If not, shout for help.
Step 3. One person calls 911 and then gets an AED, while the other person looks for no breathing or only gasping and (simultaneously) checks for a DEFINITE pulse WITHIN 10 SECONDS.
3b. If pulse and normal breathing, monitor until EMS arrives.
3c. If pulse but NO normal breathing:
-
Provide rescue breathing, at 1 breath every 2-3 seconds, or about 20-30 breaths/min.
-
Assess pulse rate for no more than 10 seconds. If the heartrate is less than 60 beats/min with signs of poor perfusion, begin CPR. Otherwise, continue rescue breathing at 1 breath every 2-3 seconds, or about 20-30 breaths/min. Recheck the pulse every 2 minutes.
3d. If no pulse or normal breathing, start CPR. The first rescuer performs cycles of 30 compressions and 2 breaths. When the second rescuer returns, the two perform cycles of 15 compressions and 2 breaths. Use the AED as soon as it is available.
Step 4. Use AED as soon as it is available.
Use AED as soon as it is available. If shock is advised, give 1 shock. Resume CPR immediately for 2 minutes (until prompted by AED to allow rhythm check). Continue until ALS providers take over or the person starts to move.
AHA guidelines algorithm for pediatric ALS
Step 1: Begin CPR. Begin bag-mask ventilation and give oxygen. Attach monitor/defibrillator.
Step 2a: If VF/pVT, deliver shock.
Step 2b: If PEA/asystole, give epinephrine as soon as possible and go to step 8 (below).
Step 3. Continue CPR for 2 min (5 rounds). Establish IV (preferred) or IO access.
Step 4a. If VF/pVT, deliver shock.
Step 4b: If PEA/asystole, give epinephrine as soon as possible and go to step 8 (below).
Step 5. Continue CPR for 2 min (5 rounds). Give epinephrine every 3-5 minutes. Consider advanced airway placement.
Step 6a. If VF/pVT, deliver shock.
Step 6b: If PEA/asystole, give epinephrine as soon as possible and go to step 8 (below).
Step 7. Continue CPR for 2 min (5 rounds). Continue epinephrine every 3-5 minutes. Give amiodarone (or lidocaine). Treat reversible causes. Go to step 4 (above).
Step 8. Continue CPR for 2 min (5 rounds). Establish IV (preferred) or IO access. Continue epinephrine every 3-5 min. Consider advanced airway and capnography.
Step 9a. If VF/pVT, go to step 6a (above) (deliver shock).
Step 9b: If PEA/asystole, continue CPR for 2 min (5 rounds). Treat reversible causes.
Step 10a. If VF/pVT, go to step 6a (above) (deliver shock).
Step 10b: If PEA/asystole, go to step 8 (above).
If signs of ROSC are noted, go to Post–Cardiac Arrest Care
High-quality CPR
The following are considered essential elements of high-quality CPR:
-
Compression rate of 100-120/min
-
Compression depth to at least one third of the anterior-posterior diameter of the chest (approximately 4 cm in infants to 5 inches in children); for adolescents, the adult compression depth of at least 5 cm, but no more than 6 cm should be used.
-
Complete chest recoil after each compression
-
Minimized interruptions in chest compressions
-
Avoidance of excessive ventilation
Additional pediatric ALS guidelines
As with BLS, algorithms are a key component of pediatric advanced life support (PALS) and are designed to simplify and expedite recognition and treatment of life-threatening conditions. Unlike BLS, PALS typically involves a coordinated team of trained responders who are able to initiate several processes simultaneously.
VF or pVT
The following summarizes the AHA PALS algorithm for VF or pVT [49] :
-
Call for help and activate the emergency response
-
Initiate high-quality CPR and give oxygen
-
Attach an ECG monitor and defibrillator pads
-
Establish vascular access; initially, attempting peripheral IV access is acceptable but only for a short, limited time; if a peripheral IV access cannot be quickly established, then an IO line should be placed by a trained provider
Once the child is attached to the monitor or AED, the rhythm should be analyzed and determined to be shockable or nonshockable. Shockable rhythms include pulseless ventricular tachycardia or ventricular fibrillation. Nonshockable rhythms include pulseless electrical activity or asystole.
If the rhythm indicates ventricular tachycardia or ventricular fibrillation, then it is a shockable rhythm and intervention proceeds as follows:
-
The defibrillator should be charged to 2 J/kg, and a shock should be delivered as soon as possible once all team members are clear
-
Promptly restart CPR for an additional 2 minutes
-
Establish IV/IO access if not already done
-
After 2 minutes, recheck the rhythm
If the rechecked rhythm is determined to be shockable, intervention proceeds as follows:
-
The defibrillator should be charged to 4 J/kg and a shock should be delivered
-
Promptly restart CPR for an additional 2 minutes
-
Give epinephrine 0.01 mg/kg IV or IO; this may be repeated every 3-5 minutes
-
Consider endotracheal intubation or other advanced airway placement
-
Consider amiodarone 5 mg/kg IV/IO for refractory VF/pVT (may repeat up to 2 times)
If the rhythm is nonshockable, intervention proceeds as follows:
-
Continue CPR for an additional 2 minutes
-
Establish IV/IO access
-
Give epinephrine 0.01 mg/kg IV/IO; this may be repeated every 3-5 minutes
-
Consider endotracheal intubation or other advanced airway placement
Once the patient is intubated, chest compressions and ventilations should work independently, with the compressions at a continuous rate of 100/min and the ventilations 10/min.
In addition, identify and correct the following if necessary:
-
Hypovolemia
-
Hypoxia
-
Hydrogen ion (acidosis)
-
Hyperkalemia/hypokalemia and metabolic disorders
-
Hypoglycemia
-
Hypothermia
-
Toxins
-
Tamponade, cardiac
-
Tension pneumothorax
-
Thrombosis, coronary or pulmonary
Bradyarrhythmias
Emergency treatment of bradycardia is indicated when the rhythm results in hemodynamic compromise. The AHA algorithm for the recognition and management of bradyarrhythmias is summarized below. [49]
When a pediatric patient is found to be bradycardiac, quickly check for a pulse. If no pulse is found, proceed to the pulseless arrest algorithm. If a pulse is found, assess for signs of cardiopulmonary compromise. These signs include the following:
-
Hypotension
-
Acutely altered mental status
-
Other signs of shock
If cardiopulmonary compromise is evident, the following immediate steps should be taken:
-
Put the patient on supplemental oxygen and assist ventilations as needed
-
Attach cardiac monitoring, blood pressure cuff, pulse oximetry, and pacing pads
-
Establish vascular access (IV, or IO if necessary)
-
Get a 12-lead ECG for rhythm analysis if possible
If the heart rate continues to be below 60 bpm and cardiopulmonary compromise is evident despite oxygenation and ventilation, then chest compressions should be initiated.
While the algorithm is being applied, attempt to identify and treat any underlying causes. If bradycardia persists after 2 minutes of chest compressions, consider the following:
-
Epinephrine: 0.01 mg/kg IV or IO; repeat every 3-5 minutes
-
Atropine: 0.02 mg/kg, not to exceed 0.5 mg/dose (for increased vagal tone or primary heart block) may be repeated once
-
Transcutaneous or transvenous pacing
-
Continue to identify and treat any underlying causes
If the bradycardia resolves, continue to support the ABCs, monitor the child, and consider expert consultation.
If the bradycardia evolves into pulseless arrest, proceed to the pulseless arrest algorithm.
Tachyarrhythmia
The most common types of tachycardia in the pediatric population are sinus tachycardia, supraventricular tachycardia, and ventricular tachycardia. As with other elements of PALS, an algorithmic approach is used for tachyarrhythmia, as outlined below.
If a pediatric patient is found to be unresponsive and not breathing in the context of tachycardia on the monitor, then proceed to the pulseless arrest algorithm. If a pulse is found, assess for signs of cardiopulmonary compromise. These signs include the following:
-
Hypotension
-
Acutely altered mental status
-
Other signs of shock
If cardiopulmonary compromise is evident, the following immediate steps should be taken:
-
Put the patient on supplemental oxygen and assist ventilations as needed
-
Attach cardiac monitoring, blood pressure cuff, pulse oximetry, and defibrillator pads
-
Establish vascular access (IV, or IO if necessary)
-
Get a 12-lead ECG for rhythm analysis
-
Evaluate the ECG and determine if the QRS duration is narrow or wide
If the QRS is wide on the initial ECG, ventricular tachycardia should be assumed. Supraventricular tachycardia with aberrant conduction is a less common possibility.
If the patient shows signs of cardiopulmonary compromise, synchronized cardioversion is delivered at 0.5-1 J/kg, with an increase to 2 J/kg if initially unsuccessful. If the patient shows no signs of cardiopulmonary compromise, adenosine may be empirically given for the possibility of supraventricular tachycardia with aberrancy.
Amiodarone and procainamide should not be routinely administered together, but they may be given in conjunction with expert consultation, as follows:
-
Amiodarone: 5 mg/kg IV infused over 20-60 minutes
-
Procainamide: 15 mg/kg IV infused over 30-60 minutes
If the QRS is narrow, determine whether sinus tachycardia or supraventricular tachycardia is more probable. Evidence supporting sinus tachycardia includes the following:
-
Presence of P waves
-
Variable R-R intervals
-
Heart rate less than 180 bpm
Evidence supporting supraventricular tachycardia includes the following:
-
Absence of P waves
-
No R-R variability
-
Heart rate 180 bpm or greater
Sinus tachycardia
Treat the underlying cause(s). Common causes of sinus tachycardia include hypovolemia, sepsis, fever, pain, hypoxia, and anemia. The history and physical examination can provide important information for narrowing the differential diagnosis.
Supraventricular tachycardia
While preparations are being made for chemical or electrical cardioversion, vagal maneuvers may be attempted to break the dysrhythmia. Vagal maneuvers include the following:
-
Application of an ice bag to the child's face
-
Unilateral carotid massage in older children.
If vagal maneuvers are unsuccessful and the patient has IV or IO access, then chemical cardioversion with adenosine is indicated. The regimen is as follows:
-
Push adenosine 0.1 mg/kg (not to exceed 6 mg)
-
If unsuccessful, second dose of 0.2 mg/kg (not to exceed 12 mg)
If chemical cardioversion is unsuccessful or not available, electrical cardioversion is indicated. The regimen is as follows:
-
If possible, sedate the patient beforehand, but do not delay cardioversion
-
Deliver a synchronized shock at 0.5-1 J/kg
-
If this is not successful, increase the charge to 2 J/kg
If chemical and electrical cardioversion continue to be unsuccessful, consider expert consultation for additional antiarrhythmics and rate-controlling recommendations.
Neonatal Resuscitation Guidelines
The 2015 update of the AHA guidelines for neonatal resuscitation are the foundation for the seventh edition of the American Academy of Pediatrics’ Textbook of Neonatal Resuscitation. The textbook, in turn, forms the basis for the training provided by the Neonatal Resuscitation Program (NPR).
The NRP should be completed by all clinicians—including physicians, nurses, and respiratory therapists—who may be involved in the stabilization and resuscitation of neonates in the delivery room. [29] In the 2015 AHA guidelines, a revised recommendation suggested that neonatal resuscitation training occur more frequently than at 2-year intervals. [49]
The following is a summary of the AHA revised algorithm for neonatal resuscitation. [49] The neonatal resuscitation algorithm was reaffirmed unchanged in the 2020 guidelines. [43]
Resuscitation equipment and anticipation of potential problems
Prior to delivery, risk factors should be identified, neonatal problems anticipated, equipment checked, qualified personal should be available, and a care plan formulated. A known perinatal risk factor, such as preterm birth, requires preparation of supplies specific to thermoregulation and respiratory support, and the delivery room should be equipped with all the tools necessary for successful resuscitation. A standardized checklist may be helpful to ensure that all necessary supplies and equipment are present and functioning.
First minute
Time: 0-30 seconds
The initial evaluation is the following questions:
-
Term gestation?
-
Good muscle tone?
-
Breathing or crying?
If initial findings are normal, the infant stays with the mother and the following routine care is provided:
-
Warm and maintain normal temperature
-
Clear airway if necessary
-
Dry newborn
If initial findings are abnormal, care consists of the following:
-
Warm and maintain normal temperature
-
Clear airway if necessary
-
Dry, stimulate, and reposition
Time: 30-60 seconds
Secondary evaluation is the following:
-
Breathing
-
Heart rate
-
Color
If the heart rate is greater than 100 bpm and the baby is pink with nonlabored breathing, proceed with routine care. If the heart rate is greater than 100 bpm and the baby is cyanotic or has labored breathing, do the following:
-
Clear airway and begin monitoring pulse oximetry oxygen saturation (SpO2)
-
Consider supplementary oxygen
-
Consider continuous positive airway pressure (CPAP)
-
Institute postresuscitation care
If the heart rate is less than 100 bpm and the baby is gasping or has apnea, do the following:
-
Clear airway and begin SpO2 monitoring
-
Provide positive-pressure ventilation (PPV)
-
Consider ECG monitor
-
Reassess heart rate, and, if greater 100 bpm, institute postresuscitation care
After first minute
If heart rate is less than 100 bpm, do the following:
-
Check chest movement
-
Take ventilation correction steps, if needed
-
ETT or laryngeal mask, if needed
-
Reassess heart rate
If the heart rate is less than 60 bpm, do the following:
-
Intubate if not already done
-
Start chest compressions
-
Coordinate with PPV
-
100% oxygen
-
ECG monitor
-
Consider emergency umbilical vein catheterization (UVC)
If the heart rate is greater than 60 bpm, stop compressions and continue ventilation.
If the heart rate remains less than 60 bpm, do the following:
-
Administer IV epinephrine
-
Consider hypovolemia
-
Consider pneumothorax
Oxygen saturation
A comparison of the preductal oxygen saturation (SpO2) targets after birth are listed in Table 3, below. [49, 55]
Table 3. Preductal Oxygen Saturation (SpO2) Targets (Open Table in a new window)
1 Minute |
2 Minutes |
3 Minutes |
4 Minutes |
5 Minutes |
|
AHA |
60-65% |
65-70% |
70-75% |
75-80% |
85-95% |
ERC |
60% |
70% |
80% |
85% |
90% |
Umbilical cord management
The following are the AHA recommendations for umbilical cord management [49] :
-
Delaying cord clamping for longer than 30 seconds is suggested for both term and preterm infants who do not require resuscitation at birth (class IIa)
-
There is insufficient evidence to recommend an approach to cord clamping for infants who require resuscitation at birth (class IIb)
-
In light of the limited information regarding the safety of rapid changes in blood volume for extremely preterm infants, routine use of cord milking for infants born at less than 29 weeks of gestation is recommended against outside of a research setting (class IIb)
Compressions
The AHA guidelines include the following specific recommendation for delivering compressions [49] :
-
Method: The 2 thumb–encircling hands technique is preferred (class IIb); allow complete chest recoil after each compression (class IIa)
-
Depth: At least one-third anteroposterior chest diameter (class IIb)
-
Compression rate: 90 compressions and 30 breaths per minute (class IIa)
-
Compression-to-ventilation ratio: 3:1 (class IIa)
-
Oxygen concentration should be increased to 100% whenever chest compressions are provided (class IIa)
-
To reduce the risks of complications associated with hyperoxia, supplementary oxygen concentration should be weaned as soon as the heart rate recovers (class I)
Meconium-stained amniotic fluid
The 2015 AHA guidelines offer the following revised recommendations for infants born with meconium-stained amniotic fluid [49] :
-
Initial steps of resuscitation should be completed under the radiant warmer and PPV should be initiated if the infant is not breathing or the heart rate is less than 100 bpm after the initial steps are completed (class IIb)
-
Routine intubation for tracheal suction is not recommended (class IIb)
Withholding or discontinuing resuscitation
The guidelines offer the following recommendations for withholding or discontinuance of resuscitation [49] :
-
It is possible to identify conditions associated with high mortality and poor outcome in which withholding resuscitative efforts may be considered reasonable, particularly when there has been the opportunity for parental agreement (class IIb)
-
In infants with an Apgar score of 0 after 10 minutes of resuscitation, if the heart rate remains undetectable, it may be reasonable to stop assisted ventilations; however, the decision to continue or discontinue resuscitative efforts must be individualized (class IIb)
-
Variables to be considered may include whether the resuscitation was considered optimal; availability of advanced neonatal care, such as therapeutic hypothermia; specific circumstances before delivery (eg, known timing of the insult); and wishes expressed by the family (class IIb)
-
When gestation, birth weight, or congenital anomalies are associated with almost certain early death and when unacceptably high morbidity is likely among the rare survivors, resuscitation is not indicated (class IIb)
-
Under circumstances when an outcome remains unclear, the desires of the parents should be supported (class IIb)
Acute Coronary Syndromes Guidelines
Last updated in 2015, AHA, ERC, and ILCOR limited recommendations to prehospital and emergency department (ED) care for acute coronary syndromes (ACSs). For in-hospital care, clinicians are advised to consult either the AHA/American College of Cardiology or European Society of Cardiology guidelines for the management of STEMI and non-STEMI ACS. [49, 56, 57]
The following summarizes the AHA algorithm for emergent treatment of ACS [49] :
-
All patients being transported for chest pain should be managed as if the pain were ischemic in origin, unless clear evidence to the contrary is established
-
Prehospital notification by EMS personnel should alert ED staff to the possibility of a patient with myocardial infarction (MI)
Specific prehospital care is as follows:
-
Monitor ABCs; be prepared to provide CPR and defibrillation
-
12-Lead ECG
-
Supplemental oxygen
-
Immediate administration of aspirin (160-325 mg) en route
-
Nitroglycerin for active chest pain (avoid in hypotensive patients) and morphine, if needed
-
Establish IV access
-
If fibrinolysis is considered, complete fibrinolytic checklist
ED assessment and immediate treatment is as follows:
-
Vital signs and pulse oximetry; if oxygen saturation is less than 90%, start oxygen at 4 L/min, titrate
-
Intravenous access and aspirin, if not administered by EMS
-
Nitroglycerin given sublingually or by spray; IV morphine if needed
-
Brief, targeted history and physical examination
-
Review/complete fibrinolytic checklist
-
Obtain cardiac marker, electrolyte, and coagulation studies
-
Portable chest radiograph in less than 30 minutes
Further therapy is based on ECG diagnosis, as follows:
-
STEMI: ST elevation or new left bundle-branch block (LBBB)
-
High-risk non-STEMI ACS: ST depression or dynamic T-wave inversion
-
Low/intermediate-risk ACS: Normal or nondiagnostic changes in ST segment or T wave
For STEMI and high-risk non-STEMI ACS, adjunctive therapies should begin as indicated. For STEMI with symptom onset 12 or fewer hours ago, reperfusion should not be delayed. Selection of therapy is defined by patient and center criteria, with the following door-to-treatment goals:
-
Percutaneous coronary intervention (PCI): 90 minutes
-
Fibrinolysis: 30 minutes
In patients with suspected STEMI for whom primary PCI reperfusion is planned, unfractionated heparin can be administered either in the prehospital or the hospital setting (class IIb)
For STEMI with onset of symptoms more than 12 hours or high-risk non-STEMI ACS, an early invasive strategy is indicated for patients with any of the following:
-
Refractory ischemic chest discomfort
-
Recurrent or persistent ST deviation
-
Ventricular tachycardia
-
Hemodynamic instability
-
Signs of heart failure
For low/intermediate-risk ACS, admit to the ED chest pain unit or appropriate bed for further monitoring and possible intervention.
Further medical management of ACS should be conducted according to the other related guidelines.
Diagnostic interventions
The 2015 guidelines include the following class I recommendations for prehospital diagnostic intervention [49] :
-
12-Lead ECG should be acquired early for patients with possible ACS
-
Notification of the receiving hospital (if fibrinolysis is the likely reperfusion strategy) and/or prehospital activation of the catheterization laboratory should occur for all patients with a recognized STEMI on ECG
-
If providers are not trained to interpret the 12-lead ECG, field transmission of the ECG or a computer report should be sent to the receiving hospital
-
12-Lead ECG diagnostic programs should be implemented with concurrent medically directed quality assurance
Additional recommendations include the following [49] :
-
Negative high-sensitivity cardiac troponin (hs-cTn) and cardiac-specific troponin I (cTnI) levels during initial patient evaluation should not be used as a standalone measure to exclude an ACS (class III)
There are no significant variances in the ERC and ILCOR recommendations. [56, 57]
Emergent reperfusion decisions in STEMI
The AHA guidelines advocate for a systems-of-care approach involving a reperfusion team that mobilizes hospital resources for an optimized approach. The guidelines argue that when such a system is active either in the ED or based on prehospital data, time-sensitive therapies can be offered more rapidly. [49]
Specific recommendations for emergent reperfusion include the following:
-
For patients presenting in less than 12 hours of symptom onset, reperfusion should be initiated as soon as possible independent of the method chosen (class I)
-
If fibrinolysis is chosen, fibrinolytics should be administered in the ED as early as possible according to a predetermined process developed by the ED and cardiology staff (class I)
-
Fibrinolytic therapy is generally not recommended for patients presenting between 12 and 24 hours after onset of symptoms unless continuing ischemic pain is present with continuing ST-segment elevation (class IIb)
-
Fibrinolytic therapy is contraindicated in patients who present more than 24 hours after the onset of symptoms (class III)
-
Coronary angioplasty with or without stent placement is the treatment of choice when it can be performed effectively with a door-to-balloon time of less than 90 minutes by a skilled provider at a skilled PCI facility (class I)
-
When fibrinolysis is contraindicated, PCI should be performed despite the delay, rather than forgoing reperfusion therapy (class I)
-
Fibrinolytic therapy followed by immediate PCI (as contrasted with immediate PCI alone) is not recommended (class III)
-
Administration of fibrinolytics in the prehospital setting ideally requires protocols using fibrinolytic checklists, 12-lead ECG interpretation, staff experienced in advanced life support, communication with the receiving institution, a medical director experienced in STEMI management, and continuous quality improvement (class I)
-
Where prehospital fibrinolysis and direct transport to a PCI center are both available, prehospital triage and transport directly to a PCI center may be preferred (class IIb)
-
Regardless of whether time of symptom onset is known, the interval between first medical contact and reperfusion should not exceed 2 hours (class I)
-
In patients presenting within 2 hours of symptom onset, immediate fibrinolysis rather than primary PCI may be considered when the expected delay to primary PCI is more than 60 minutes (class IIb)
-
In adult patients presenting with STEMI in the ED of a non–PCI-capable hospital, immediate transfer without fibrinolysis from the initial facility to a PCI center is recommended, instead of immediate fibrinolysis at the initial hospital with transfer only for ischemia-driven PCI (class I)
ERC guidelines include one additional recommendation: When fibrinolysis is the treatment strategy, if transport times exceed 30 minutes, fibrinolysis using trained EMS staff is preferred. [56]
Questions & Answers
Overview
What is cardiopulmonary resuscitation (CPR)?
What are the indications for cardiopulmonary resuscitation (CPR)?
What are the contraindications to cardiopulmonary resuscitation (CPR)?
When is cardiopulmonary resuscitation (CPR) indicated?
What is the only absolute contraindication to cardiopulmonary resuscitation (CPR)?
What are the most common arrhythmias requiring cardiopulmonary resuscitation (CPR)?
When should cardiopulmonary resuscitation (CPR) be performed?
What equipment is used to perform cardiopulmonary resuscitation (CPR)?
What are the steps of cardiopulmonary resuscitation (CPR)?
Which type of cardiopulmonary resuscitation (CPR) is recommended for lay rescuers?
How is the patient positioned for cardiopulmonary resuscitation (CPR)?
How is cardiopulmonary resuscitation (CPR) performed when an adult is unconscious?
How are chest compressions administered during cardiopulmonary resuscitation (CPR)?
How are ventilations administered during cardiopulmonary resuscitation (CPR)?
How is the mouth-to-mouth technique performed during cardiopulmonary resuscitation (CPR)?
What are complications of cardiopulmonary resuscitation (CPR)?
What is the prognosis in patients with cardiac arrest receiving cardiopulmonary resuscitation (CPR)?
What is included in cardiopulmonary resuscitation (CPR)?
What is the prognosis associated with compression-CPR (COCPR)?
What are the AHA guidelines indications for compression-only CPR (COCPR)?
What is the common cause of cardiac arrests occurring in public areas?
Where can information on advanced resuscitation care be found?
What are the most common arrhythmias requiring cardiopulmonary resuscitation (CPR)?
When should cardiopulmonary resuscitation (CPR) be performed?
What is the prognosis of cardiac arrest following defibrillation?
What is a relative contraindication to performing cardiopulmonary resuscitation (CPR)?
What is the role of anesthetic agents in cardiopulmonary resuscitation (CPR)?
When can cardiopulmonary resuscitation (CPR) be performed?
What are the universal precautions for cardiopulmonary resuscitation (CPR)?
What is the role of endotracheal intubation in cardiopulmonary resuscitation (CPR)?
What is the role of a cardiac defibrillator during cardiopulmonary resuscitation (CPR)?
How should a patient be positioned for cardiopulmonary resuscitation (CPR)?
What are the steps of cardiopulmonary resuscitation (CPR)?
How is cardiopulmonary resuscitation (CPR) initiated?
What are the techniques used for cardiopulmonary resuscitation (CPR)?
Is there benefit in untrained providers performing cardiopulmonary resuscitation (CPR)?
What is the chest compression technique for cardiopulmonary resuscitation (CPR)?
What can be done to prevent provider fatigue and injury during CPR chest compressions?
What is the efficacy of mechanical cardiopulmonary resuscitation (CPR) devices?
How many ventilations are required during cardiopulmonary resuscitation (CPR)?
How is the mouth-to-mouth technique performed in cardiopulmonary resuscitation (CPR)?
What is the significance of chest rise during CPR mouth-to-mouth ventilation?
Which equipment may be used for ventilation during cardiopulmonary resuscitation (CPR)?
How is the bag-valve-mask (BVM) technique performed for cardiopulmonary resuscitation (CPR)?
What are complications of cardiopulmonary resuscitation (CPR)?
What is the AHA adult basic life support (BLS) algorithm?
What are the AHA recommendations for cardiopulmonary resuscitation (CPR) for dispatchers?
What is the significance of detection of pulse in cardiopulmonary resuscitation (CPR)?
What are the AHA recommendations for cardiopulmonary resuscitation (CPR) for EMS providers?
How is adult ACLS defined in cardiopulmonary resuscitation (CPR) guidelines?
Which finding in intubated patients is an indication to end cardiopulmonary resuscitation (CPR)?
What are the AHA guidelines for post-cardiac arrest care?
What are the major revisions in in the 2015 AHA guidelines for post-cardiac-arrest care?
What is the AHA algorithm for immediate post-cardiac arrest care in adults after ROSC?
How do the ERC guidelines for postresuscitation care compare with AHA guidelines?
What are the AHA guidelines for targeted temperature management (TTM) in comatose patients?
What is included in postresuscitation targeted temperature management (TTM)?
What are the 2015 AHA recommendations for postresuscitation TTM?
What are AHA recommendations for the timing of prognostication following cardiac arrest?
What factors does the ERC use for prognostication following cardiac arrest?
When should organ donation be considered following cardiac arrest?
What is the basis for training provided by the Neonatal Resuscitation Program (NPR)?
Who should complete the neonatal resuscitation program (NRP)?
In the AHA revised algorithm for neonatal resuscitation, what steps are taken prior to delivery?
Which questions are asked in the initial evaluation of newborn’s cardiac health?
What is included in the routine care of infants if the initial cardiac findings are normal?
What is included in the care of newborns if the initial cardiac findings are abnormal?
What included in the secondary cardiac evaluation of newborns?
What is the initial management of cardiac distress in newborns?
What is the management if the heart rate of a newborn is less than 100 bpm after 1 minute?
What is the management if the heart rate of the newborn is less than 60 bpm after 1 minute?
What is the management if the heart rate of the newborn is greater than 60 bpm after 1 minute?
What is the management if the heart rate of the newborn is less than 60 bpm after initial treatment?
What are the AHA and ERC recommended preductal oxygen saturation (SpO2) targets for neonates?
What are the AHA recommendations for umbilical cord management in neonates?
What are the AHA recommendations for delivering chest compressions to neonates?
What are the limitations of guidelines for acute coronary syndromes (ACS)?
What is the AHA algorithm for emergent treatment of acute coronary syndromes (ACS)?
What are the AHA guidelines for prehospital care of acute coronary syndromes (ACS)?
What are the possible ECG classifications of acute coronary syndromes (ACS)?
What are the door-to-treatment goals for STEMI and high-risk non-STEMI ACS?
When is heparin indicated in the treatment of suspected STEMI?
When is an early invasive strategy indicated for the treatment of STEMI and high-risk non-STEMI ACS?
What are the class I recommendations for prehospital diagnostic intervention in patients with ACS?
Why does the AHA guidelines advocate for a for a systems-of-care approach for ACS?
What are the specific recommendations for emergent reperfusion in ACS?
What are the AHA guidelines for the use of cardiopulmonary resuscitation (CPR) in children?
How do the AHA pediatric BLS guidelines differ for lay providers compared to healthcare providers?
How do the AHA pediatric BLS guidelines differ for one rescuer CPR compared to two rescuer CPR?
What are the AHA pediatric guidelines for CPR with use of an AED?
What are the essential elements of high-quality cardiopulmonary resuscitation (CPR) in children?
How is a rhythm determined to be shockable in pediatric cardiac arrest?
What is the emergent treatment of ventricular tachycardia or ventricular fibrillation in a child?
What steps should be taken to in the treatment of a rechecked shockable rhythm in a child?
What is the emergent treatment for a child in cardiac arrest with a nonshockable rhythm?
Which steps of cardiopulmonary resuscitation (CPR) are performed once a patient is intubated?
What needs to be identified and corrected during cardiopulmonary resuscitation (CPR)?
What is the AHA algorithm for the recognition and management of bradyarrhythmias in children?
What is the significance of pulse in the treatment of bradyarrhythmias in children?
What is the treatment of cardiopulmonary compromise in children with bradyarrhythmias?
If cardiopulmonary compromise is evident in a child with tachycardia, what steps are taken?
When should chest compression be initiated in children with bradyarrhythmias?
What treatment is continued in a child with resolved bradycardia?
What are the most common types of tachycardia in the pediatric population?
What are the signs used to determine treatment approach in children with tachycardia?
How is tachycardia diagnosed with ECG in children?
Which medications are given to treat children with tachycardia?
What findings indicate sinus tachycardia in children?
Which findings suggest supraventricular tachycardia in children?
What are common causes of sinus tachycardia in children?
Which vagal maneuvers are used to treat children with sinus tachycardia?
What is the role of adenosine in the treatment of children with sinus tachycardia?
What is the role of electrical cardioversion in the treatment of sinus tachycardia in children?
When should an expert be consulted in the emergency treatment of sinus tachycardia in children?
-
Delivery of chest compressions. Note the overlapping hands placed on the center of the sternum, with the rescuer's arms extended. Although it may be difficult to tell from the illustration, the rescuer's elbows should be locked out. Chest compressions are to be delivered at a rate of 100 to 120 per minute. The rescuer should push as hard as needed to attain a depth of each compression of 2 inches, and should allow complete chest recoil between each compression ('2 inches down, all the way up'). The rescuer should minimize any interruptions in compressions.
-
Delivery of mouth-to-mouth ventilations. Avoid excessive ventilation. If no advanced airway, 30:2 compression-ventilation ratio. That is, perform 30 compressions and then 2 breaths.
-
CPR positioning. Video courtesy of Daniel Herzberg, 2008.
-
CPR ventilation. Video courtesy of Daniel Herzberg, 2008.
-
CPR compressions. Video courtesy of Daniel Herzberg, 2008.
Tables
Link 1 |
Link 2 |
Link 3 |
Link 4 |
Link 5 |
Link 6 | |
IHCA |
Early recognition and prevention |
Activation of the emergency response system |
Immediate high-quality CPR |
Rapid defibrillation |
Advanced life support and post-arrest care |
Recovery |
Responder(s) |
Primary Provider |
Code Team |
Cath Lab/ICU |
|||
OHCA |
Recognition and activation of the emergency response system |
Immediate high-quality CPR |
Rapid defibrillation |
Basic and advanced emergency medical services |
Advanced life support and post-arrest care |
Recovery |
Responder(s) |
Lay Rescuers |
Emergency Medical Services (EMS) | ED/Cath Lab/ICU | |||
Untrained Lay Responders |
Trained Lay Responders |
Healthcare Professionals |
|
Step 1 |
Ensure scene safety |
||
Step 2 |
Check for response |
||
Step 3 |
Responder should shout for nearby help and phone or have another bystander phone 9-1-1; the phone should remain on speaker for receiving further instructions from the dispatcher. |
Responder should shout for nearby help and activate the emergency response system (9-1-1, emergency response). Ensure that the phone remains on speaker, if at all possible. |
Responder should shout for nearby help. The resuscitation team can be activated now or after checking breathing and pulse. |
Step 4 |
Follow dispatcher’s instructions. |
Check for no breathing or only gasping; if there is none, begin CPR with chest compressions. |
Check for no breathing or only gasping and check for a pulse (ideally should be done simultaneously). Activation and retrieval of the AED/emergency equipment by either the lone healthcare provider or by a second person must occur immediately after a check of breathing and pulse identifies cardiac arrest. |
Step 5 |
As instructed by dispatcher to check for no breathing or only gasping. |
Answer dispatcher’s questions and follow subsequent instructions. |
Begin CPR immediately, and use AED/defibrillator if available. |
Step 6 |
Follow dispatcher’s instructions. |
Send another person for an AED, if one is available. |
With arrival of a second responder, two-person CPR is provided and AED/defibrillator is used. |
1 Minute |
2 Minutes |
3 Minutes |
4 Minutes |
5 Minutes |
|
AHA |
60-65% |
65-70% |
70-75% |
75-80% |
85-95% |
ERC |
60% |
70% |
80% |
85% |
90% |

What would you like to print?
- Practice Essentials
- Background
- Indications & Contraindications
- Preparation
- Technique
- Post Procedure
- CPR and ECC Guidelines Summary
- Chain of Survival Guidelines
- Adult BLS and AED Guidelines
- Adult ACLS Guidelines
- Post–Cardiac Arrest Care Guidelines
- Pediatric BLS and ACLS Guidelines
- Neonatal Resuscitation Guidelines
- Acute Coronary Syndromes Guidelines
- Questions & Answers
- Show All
- Media Gallery
- Tables
- References



