Practice Essentials
Olecranon bursitis, a relatively common condition, is inflammation of the subcutaneous synovial-lined sac of the bursa overlying the olecranon process at the proximal aspect of the ulna (see the images below). [1, 2] The bursa supports the olecranon and reduces friction between it and the skin, especially during movement. The superficial location of the bursa, between the ulna and the skin at the posterior tip of the elbow, makes it susceptible to inflammation from acute or repetitive (cumulative) trauma. Many cases are idiopathic in nature, but, less commonly, inflammation results secondary to an infectious etiology (septic bursitis). (See Etiology, Workup, Treatment, and Medication.) [1, 3, 4, 5, 6, 7]
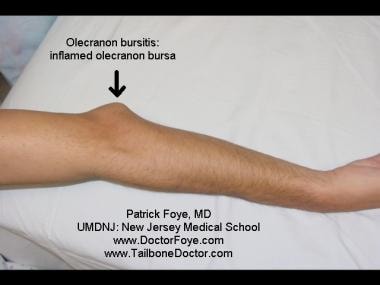
 Olecranon bursitis, shown here with the elbow flexed. Image courtesy of UMDNJ-New Jersey Medical School, www.DoctorFoye.com, and www.TailboneDoctor.com.
Olecranon bursitis, shown here with the elbow flexed. Image courtesy of UMDNJ-New Jersey Medical School, www.DoctorFoye.com, and www.TailboneDoctor.com.
 Olecranon bursitis seen with the elbow extended. Focal swelling at the olecranon is more visible with the elbow extended than in the flexed position. Image courtesy of UMDNJ-New Jersey Medical School, www.DoctorFoye.com, and www.TailboneDoctor.com.
Olecranon bursitis seen with the elbow extended. Focal swelling at the olecranon is more visible with the elbow extended than in the flexed position. Image courtesy of UMDNJ-New Jersey Medical School, www.DoctorFoye.com, and www.TailboneDoctor.com.
 Olecranon bursitis seen with the elbow extended. Image courtesy of UMDNJ-New Jersey Medical School, www.DoctorFoye.com, and www.TailboneDoctor.com.
Olecranon bursitis seen with the elbow extended. Image courtesy of UMDNJ-New Jersey Medical School, www.DoctorFoye.com, and www.TailboneDoctor.com.
Signs and symptoms of olecranon bursitis
Classically, olecranon bursitis presents as a clearly demarcated, often fluctuant posterior elbow swelling, appearing as a "goose egg" over the olecranon process.
Patient history may include the following findings:
-
The patient may report pain at the affected site, although sometimes the swelling is painless, especially in noninflammatory, aseptic bursitis
-
Pain often is exacerbated by pressure; however, chronic, recurrent swelling is often nontender
-
Swelling may have a gradual (mostly due to a chronic cause) or acute/sudden (due to trauma or infection/inflammation) onset
Workup in olecranon bursitis
If the clinician suspects an underlying condition is present, laboratory studies are necessary. If an infectious etiology is suspected (due to the presence of fever, erythema, previous puncture wounds, or cellulitis), the olecranon bursa should be aspirated and the fluid sent for culture, for a cell count (white blood cells [WBCs], red blood cells [RBCs]), and for Gram staining for bacteria. Additionally, lab work should be obtained, including a blood count with differential, glucose, C-reactive protein, and the erythrocyte sedimentation rate. If there is concern for rheumatoid arthritis or gout, a rheumatoid factor and uric acid level, respectively, should be obtained.
Plain film radiographs of the elbow should be performed to assess for a possible olecranon fracture if significant trauma occurred or if an avulsed osteophyte is present at the triceps insertion into the olecranon, which is fairly common.
The use of ultrasonography has been shown to be extremely effective in the diagnosis of olecranon bursitis and other soft-tissue lesions in the olecranon area by rapidly demonstrating the presence of effusions, synovial proliferation, loose bodies, increased blood flow consistent with inflammation, tendonitis with calcifications, and other indications of bursitis. [8]
In atypical cases, a magnetic resonance imaging (MRI) study may be indicated to help exclude concomitant pathology, such as a stress fracture, triceps tendinopathy versus tear, or the rare case of osteomyelitis/abscess or tumor. [9]
Management of olecranon bursitis
Generally, physical and occupational therapy are not needed for the treatment of olecranon bursitis. In some cases of aseptic bursitis, however, the physician may recommend a course of physical or occupational therapy to speed recovery time.
Oral nonsteroidal anti-inflammatory drugs (NSAIDs) can help to reduce the pain and inflammation of olecranon bursitis, but these products probably should be avoided if joint aspiration reveals a hemorrhagic bursitis. Injectable corticosteroid can be beneficial in cases in which the history, physical examination, and joint aspiration do not raise a significant suspicion of infection. [10] Most cases of olecranon bursitis respond very well to a series of 1-2 joint aspirations (with or without corticosteroid injection) combined with additional treatment.
Usually, no surgical intervention is required in cases of olecranon bursitis. [11] In severe cases resistant to conservative treatment, a bursectomy may be indicated.
If surgical intervention is required, endoscopic olecranon bursectomy is an effective alternative to open bursectomy in either aseptic or septic cases. Endoscopic outcomes are excellent and can minimize wound-healing problems. [12]
Etiology
The olecranon bursa allows the skin to glide freely over the olecranon process. Given its superficial location, however, it is susceptible to inflammation from acute or repetitive trauma.
Acute injuries can be secondary to any repetitive trauma (eg, the constant rubbing of an elbow against the table as a person writes) or secondary to a sports-related activity that includes direct or repetitive trauma to the posterior elbow (eg, landing on the olecranon process during a fall onto a hard floor or an artificial-turf playing field).
Septic bursitis, a less common cause of olecranon bursa inflammation, can result from an abrasion or laceration of the affected site or by way of seeding from hematogenous spread via bacteremia. Inflammation can also be caused by a systemic inflammatory process (eg, rheumatoid arthritis) or a crystal-deposition disease (eg, gout or pseudogout). Additionally, septic bursitis may develop as a secondary complication of aseptic olecranon bursitis. [1] Risks factors for the development of non-traumatic olecranon bursitis include diabetes mellitus, uremia, a history of intravenous drug abuse, alcohol abuse, or long-term use of steroids. [13, 14, 15, 16, 17, 18] Larsen et al reported a case of bacillus Calmette-Guérin (BCG) olecranon bursitis that developed from disseminated BCG infection, the result of BCG treatment for superficial bladder cancer. [19]
In patients on long-term hemodialysis treatment, uremia or a mechanical insult (such as resting the posterior elbow during hemodialysis treatment) is thought possibly to cause bursitis. [20] Inflammation of the bursa can also be an adverse effect of the drug sunitinib, which is used to treat patients with renal cell carcinoma. [21]
A retrospective study by Schermann et al of olecranon bursitis in the Israel Defense Forces found the condition to be more prevalent in combat units than in noncombat units, with most of the diagnoses being made during summer and autumn, when training is particularly intensive. The investigators stated that the relatively high number of olecranon bursitis cases diagnosed during those times of the year is probably related to outdoor training that requires crawling and suggested that the use of protective gear could alleviate the problem. [22]
Prognosis
Most cases of aseptic olecranon bursitis respond very well to a series of 1-2 joint aspirations (with or without corticosteroid injection) combined with additional treatment. Some patients may experience recurrence, in which even relatively minor trauma causes a significant effusion to reappear.
Complications
Complications of olecranon bursitis include progressive or persistent pain potentially associated with functional impairment of the affected upper extremity. Potential complications of aspiration/injection include the following:
-
Bleeding
-
Bruising
-
Allergic reaction to corticosteroids (if utilized)
-
Swelling - This may recur, particularly if the patient does not maintain adequate pressure or icing at the site or if an infection was present at the time of the initial aspiration
-
Infection - The clinician should use appropriate aseptic techniques to minimize the chance of iatrogenic infection
-
Persistent drainage through the injection tract
-
Ulnar nerve injury - This theoretically may occur if a medial approach is used for the aspiration/injection
-
Transient elevation of blood glucose levels (if corticosteroids are utilized)
-
Cardiac arrhythmia - This potentially can result from intravascular injection, due to the local anesthetic component
-
Peripheral nerve dysfunction - This is possible if the injection is administered near or within a major nerve
-
Compromised wound healing
-
Gastric, hepatic, and renal adverse effects from NSAIDs and narcotic analgesics
Patient Education
The patient should be educated regarding olecranon bursitis’s diagnosis, causative factors, and treatment plan. The most important aspect of patient education is ensuring that the patient understands the importance of and knows to immediately report any signs or symptoms of persistent drainage or infection, particularly if a corticosteroid injection has been given. Diabetic patients should be told that they may experience a transient elevation of their blood glucose levels.
Patients should be informed that a corticosteroid usually does not begin to provide symptomatic improvement until a few days after the injection. Patients should also understand that they may experience a mild, transient increase in symptoms during the window of time when the local anesthetic has worn off but the steroids have not begun to take therapeutic effect. For patient education information, see the Arthritis Center, as well as Bursitis.
-
Olecranon bursitis, shown here with the elbow flexed. Image courtesy of UMDNJ-New Jersey Medical School, www.DoctorFoye.com, and www.TailboneDoctor.com.
-
Olecranon bursitis seen with the elbow extended. Focal swelling at the olecranon is more visible with the elbow extended than in the flexed position. Image courtesy of UMDNJ-New Jersey Medical School, www.DoctorFoye.com, and www.TailboneDoctor.com.
-
Olecranon bursitis seen with the elbow extended. Image courtesy of UMDNJ-New Jersey Medical School, www.DoctorFoye.com, and www.TailboneDoctor.com.
-
Olecranon bursogram. This image shows a needle injecting contrast material into the olecranon bursa, under fluoroscopic guidance. Although olecranon bursa aspiration/injection usually does not require fluoroscopy or contrast, employing fluoroscopy here has demonstrated the outline of the involved bursa. Image ©2005, by Patrick M. Foye, MD, UMDNJ: New Jersey Medical School.
-
Needle aspiration in olecranon bursitis. Image courtesy of UMDNJ-New Jersey Medical School, www.DoctorFoye.com, and www.TailboneDoctor.com.
-
Aspiration of a hemorrhagic effusion in a patient with olecranon bursitis. Image courtesy of UMDNJ-New Jersey Medical School, www.DoctorFoye.com, and www.TailboneDoctor.com.
-
After fluid is removed from the olecranon bursa, an elastic, tubular compressive sleeve can be used to minimize reaccumulation of the fluid. Image courtesy of UMDNJ-New Jersey Medical School, www.DoctorFoye.com, and www.TailboneDoctor.com.
-
Gout. Radiograph of erosions with overhanging edges.
-
Gout. Polarizing microscopy revealing needles of urate.
-
Rheumatoid arthritis. Rheumatoid nodules at the elbow. Photograph by David Effron MD, FACEP
-
Olecranon fracture.







