Practice Essentials
Medial collateral ligament (MCL) and lateral collateral ligament (LCL) injuries of the knee are common. In fact, injury to the MCL is the most common ligamentous knee injury.
The MCL and LCL provide restraint to valgus and varus angulation of the knee, respectively. The MCL has superficial and deep components. The superficial MCL fibers attach proximally to the medial femoral epicondyle and distally to the medial aspect of the tibia, approximately 4 cm distal to the joint line. The deep MCL fibers originate from the medial joint capsule and are attached to the medial meniscus.
The LCL is part of a complex of ligaments collectively named the posterolateral corner (PC). The structures in the PC include the LCL, the popliteofibular ligament, the popliteus ligament, the arcuate ligament, the short lateral ligament, and the posterolateral joint capsule. The LCL is separated from the lateral meniscus by a fat pad (see image below). [1, 2, 3, 4]
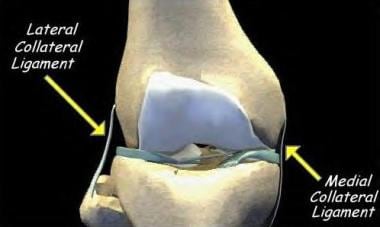 The medial and lateral collateral ligaments of the knee. Courtesy of Randale Sechrest, MD, CEO, Medical Multimedia Group.
The medial and lateral collateral ligaments of the knee. Courtesy of Randale Sechrest, MD, CEO, Medical Multimedia Group.
Signs and symptoms
Medial collateral ligament (MCL) injury
Signs and symptoms include the following:
-
Most patients are able to continue ambulating after an acute injury
-
Pain and stiffness are localized to the medial knee
-
Erythema may appear after several days
-
Instability or mechanical symptoms (eg, a locking or popping sensation) are uncommon
Lateral collateral ligament (LCL) injury
Signs and symptoms include the following:
-
Most patients are able to continue ambulating after an acute injury
-
Pain and stiffness are localized to the lateral knee
-
Erythema may appear after several days
-
Swelling is often present
-
Instability or mechanical symptoms (eg, a locking or popping sensation) are uncommon
Workup
Diagnosis of a medial collateral ligament (MCL) or lateral collateral ligament (LCL) injury is usually clinical. [5, 6, 7]
Plain films in patients with suspected knee ligamentous injuries should include anteroposterior, lateral, intercondylar notch, and sunrise views.
Magnetic resonance imaging (MRI) is helpful for ruling out other soft-tissue injuries (eg, anterior or posterior cruciate ligament tears, meniscus injury).
Management
Medial collateral ligament (MCL) injury
The type of physical therapy (PT) treatment indicated for a medial collateral ligament (MCL) injury depends on the severity of the injury. [5, 8] Recommendations for treatment include the following:
-
Grade I - Compression, elevation, and cryotherapy are recommended; short-term use of crutches may be indicated, with weight-bearing–as–tolerated (WBAT) ambulation; early ambulation is recommended
-
Grade II - A short-hinged brace that blocks 20° of terminal extension but allows full flexion should be used; the patient may ambulate, WBAT; closed-chain exercises allow for strengthening of knee musculature without putting stress on the ligaments
-
Grade III - The patient initially should be non–weight-bearing (NWB) on the affected lower extremity; a hinged braced should be used, with gradual progression to full weight-bearing (FWB) over 4 weeks; grade III injuries may require 8-12 weeks to heal
All MCL injuries should be treated with early range of motion (ROM) and strengthening of musculature that stabilizes the knee joint.
Lateral collateral ligament (LCL) injury
Recommendations for the treatment of LCL injuries include the following:
-
Grades I and II - These injuries are treated according to a regimen similar to that for MCL injuries of the same severity; a hinged brace is used for 4-6 weeks
-
Grade III - Severe LCL injuries typically are treated surgically due to rotational instability, because they usually involve the posterolateral corner of the knee; patients may require bracing and physical therapy for up to 3 months in order to prevent later instability
Related Medscape Drugs & Diseases topics:
Collateral Ligament Injuries MRI
Pathophysiology
Medial collateral ligament (MCL) and lateral collateral ligament (LCL) injuries are caused primarily by valgus and varus stress (respectively) to the knee joint. Injuries also can occur to both ligaments with excessive lateral rotation of the knee.
Epidemiology
Frequency
United States
The annual incidence of acute knee injury in the United States is estimated to be 300 cases per 100,000 population. Collateral ligament injuries account for 25% of patients presenting to emergency rooms with acute knee injury. Peak incidence of collateral ligament injuries occurs in adults aged 20-34 years. The National Collegiate Athletic Association (NCAA) injury surveillance system reported 2.1 medial or lateral collateral injuries per 1000 player exposures in games across all NCAA sports over 1 year. [9] Even noncontact sports, such as gymnastics and swimming, can lead to collateral ligament injuries. [10]
International
In a prospective study of Elite Club players in the Union of European Football Associations (UEFA), Lundblad et al found that medial collateral ligament (MCL) injuries accounted for 130 of 4364 registered injuries (3%) occurring among 51 teams over 1-3 full seasons. Ninety-eight MCL injuries (75%) were contact related, with tackling or being tackled representing the most frequent playing-associated contact mechanisms (12% and 29%, respectively). [11]
Mortality/Morbidity
Medial collateral ligament (MCL) and lateral collateral ligament (LCL) injuries can in most individuals be treated successfully with conservative methods. Severe injuries may require surgical intervention and tend to have good outcomes. [2, 5]
Race
There is no known racial predilection for medial collateral ligament (MCL) and lateral collateral ligament (LCL) injuries.
Sex
Unlike anterior cruciate ligament (ACL) injuries, which occur at a higher rate in women, medial collateral ligament (MCL) and lateral collateral ligament (LCL) injuries occur at equal rates in men and women. [10, 12]
Related Medscape Drugs & Diseases articles:
Anterior Cruciate Ligament Pathology
Rehabilitation for Anterior Cruciate Ligament Injury
Anterior Cruciate Ligament Injury
Anterior Cruciate Ligament (ACL) MRI
Age
Age patterns for medial collateral ligament (MCL) and lateral collateral ligament (LCL) injuries are bimodal, with the highest incidence rates found in individuals aged 20-34 years and in persons aged 55-65 years. Nonetheless, MCL and LCL injuries can occur at any age.
-
The medial and lateral collateral ligaments of the knee. Courtesy of Randale Sechrest, MD, CEO, Medical Multimedia Group.






