Overview
Diagnosis and treatment of painful muscle syndromes can be a difficult and frustrating task for any clinician. Typically, the mainstay of therapy for such conditions is therapeutic exercise, analgesics, and a tincture of time. Unfortunately, not all patients respond to this paradigm, and, despite heroic efforts on the part of the treating clinician, some conditions are refractory to this approach.
Reports have described the purported effectiveness of using a biologic neuromuscular blocking agent, botulinum toxin, in the treatment of painful conditions associated with skeletal muscle. While incompletely understood and at times controversial, use of botulinum toxin in the treatment of conditions associated with involuntary muscle contraction, such as focal dystonia and spasticity, is supported by prospective, randomized clinical research; however, while the volume of comparable studies in pain syndromes is growing, the number of clinical randomized trials is limited. Moreover, not all such reports have demonstrated clear efficacy of the use of botulinum toxin under all circumstances. Therefore, in view of our current understanding of the nature of muscle-induced pain and the paucity of prospective research regarding neuromuscular blockade and/or inhibition of nociception in such conditions, critical and careful analysis of the data and opinions presented in this section is appropriate.
This article provides general direction and practical details for the clinician considering botulinum toxin for treatment of pain. Anatomic drawings for injection localization and dosing information are intended only as general guidelines; therapy with botulinum toxin always must be individualized, accounting for the patient's needs and the clinician's expertise. In addition, information presented should be used as a convenient reference source, not as a substitute for clinical training in the use of botulinum toxin.
Pharmacology of Botulinum Toxin
Pharmacology
Botulinum toxin is produced by the anaerobic bacterium Clostridium botulinum, a rod-shaped, gram-positive organism found in soil and water. Botulinum toxin type A (abbreviated BoNT-A or BTX-A) belongs to a family of neurotoxins (designated as types A, B, C1, C2, D, E, F, and G) with similar properties. BoNT-A causes degrees of flaccid (rather than rigid or tetanic) paralysis by blocking acetylcholine, required for muscle contraction, from release at the nerve terminal. [1, 2, 3] Therapeutic benefit may be derived by exploiting the pharmacologic properties of carefully administered regional application of this purified neurotoxin.
The various botulinum toxins possess individual potencies, and care is required to assure proper use and avoid medication errors. Recent changes to the established drug names by the FDA were intended to reinforce these differences and prevent medication errors. The products and their approved indications include the following:
-
OnabotulinumtoxinA (Botox, Botox Cosmetic)
Botox - Cervical dystonia, severe primary axillary hyperhidrosis, strabismus, blepharospasm
Botox Cosmetic - Moderate-to-severe glabellar lines
-
AbobotulinumtoxinA (Dysport) - Cervical dystonia, moderate-to-severe glabellar lines
-
IncobotulinumtoxinA (Xeomin) - Cervical dystonia, blepharospasm
-
RimabotulinumtoxinB (Myobloc) - Cervical dystonia
-
DaxibotulinumtoxinA (Daxxify) - Cervical dystonia
Botulinum toxin's putative success in pain management was originally attributed to its ability to block acetylcholine from being released at the synapse. One important feature of botulinum toxin in pain treatment is that the neurotoxin is thought to act only on motor nerve endings while sparing sensory nerve fibers from its effects. Subsequently, however, effects of botulinum toxin on nociceptive neurons were demonstrated in preclinical studies. [4, 5, 6, 7] Thus, analgesic effects are likely to occur, but not as a consequence of blocking afferent sensory fibers at the site of injection; rather, they have been attributed to secondary effects that may be the result of muscle paralysis, improved blood flow, the release of nerve fibers under compression by abnormally contracting muscle, and, perhaps more importantly, the effects of the toxin on nociceptive neurons.
Median lethal dose (LD50)
Botulinum toxin's median lethal dose (LD50) has been determined across several animal species but not in humans. A unit of BoNT-A usually is defined in terms of its biologic potency. One mouse unit (MU) of BoNT-A equals the LD50 for a 20-g Swiss-Webster mouse. Yet BoNT-A sensitivity varies among different species. LD50 in monkeys has been determined as 39 U/kg. Based on these findings from primate studies, human LD50 is estimated at approximately 3000 U for a 70-kg adult. Typical doses for larger muscle groups range from 60-400 total units given in a single treatment; however, because of inadequate understanding of the complete dose response curve in humans, a relative ceiling dose of 360 U, given no sooner than 12 weeks apart, is recommended.
Adverse effects
Since the mechanism of action of BoNT-A is so specific, adverse effects are uncommon and systemic effects rare. Flulike syndrome has been reported, but it is generally short-lived. Other adverse effects have been reported, but they are not necessarily a result of BoNT-A treatment. They include muscle soreness, headaches, light-headedness, fever, chills, hypertension, weakness, diarrhea, and abdominal pain.
Muscular weakness, the predominant and desirable effect of botulinum toxin injection, also may be considered an adverse effect when weakness occurs in an unintended area or is greater than intended. Clinicians must understand the functional consequences of unintended weakness caused by botulinum toxin injection. While overweakening the muscles that curl the toes may have few, if any, undesirable consequences, spread of toxin into the muscles that control swallowing, which can occur when injecting muscles near the larynx (for instance, the proximal part of the sternocleidomastoid muscle), may result in difficulty swallowing. Patients, therefore, should be informed of the potential for either too much weakness in the injected area or weakness in nearby muscles.
Use of Botulinum Toxin in Painful Neuromuscular Disorders
Previous studies of conditions with involuntary muscular contractions have provided some indirect evidence of the analgesic effects of botulinum toxin. A summary of a MEDLINE search for clinical studies with the headings "botulinum toxin," and "pain" performed from 1966 to September 2005 resulted in more than 40 studies that included "pain" within the article title or abstract.
In the report, pain response to treatment with botulinum toxin was cited within the context of treatment for a number of conditions, including tennis elbow, chronic anal fissure, pain attributed to mastectomy and hemorrhoidectomy, headaches (including migraine), piriformis syndrome, facial pain, myofascial pain, temporomandibular joint syndrome (TMJ), low back pain, chronic prostatic pain, and whiplash. [8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24]
Variables in these studies included dosing, concentration, injection techniques, use of concurrent therapeutic modalities, varying diagnoses, and chronicity of neurologic dysfunction. Some patients treated for disorders that included involuntary muscle contraction (eg, dystonia) also reported benefits in pain reduction in muscles injected with botulinum toxin. Variables in the studies cited included the presence or absence of concurrent therapy, diagnoses, length of time since onset of pain, dosing and concentration, and methodology for measurement of outcome. [25] In 2016, the US Food and Drug Administration approved onabotulinumtoxinA to decrease the severity of stiffness in ankle and toe muscles among adults with lower limb spasticity. [26]
Another review of botulinum toxin studies was performed by the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. [27] Evidence of the toxin's effectiveness was examined for a variety of conditions, including chronic tension-type headache, episodic migraine, chronic daily migraine, [28] and chronic low back pain.
According to the subcommittee's report, the evidence indicated that botulinum toxin may be useful in the treatment of lower back pain but that it is probably not effective against episodic migraine and chronic tension-type headache. The report also stated that the available evidence was not strong or consistent enough to determine botulinum toxin's usefulness in the treatment of chronic daily headache (primarily, transformed migraine).
A German report also investigated botulinum toxin's effectiveness against tension-type headache. [29] In a double-blind, randomized, placebo-controlled study, researchers compared the number of headache-free days experienced by patients 4 weeks prior to injections of BoNT-A with the number of such days occurring 4-8 weeks after treatment. The number of headache-free days increased for the study's placebo and nonplacebo groups, but the difference in increase between the 2 groups was not significant.
The researchers did find, however, that in comparison with the placebo group, the patients who received BoNT-A injections experienced a significant reduction in the duration of their headaches.
A study by Naik et al reported that the use of botulinum toxin to treat painful cutaneous leiomyomas was associated with improved quality of life and with a trend toward improved pain at rest. [30]
Botulinum Toxin and Myofascial Pain
Many therapies are available to patients with myofascial pain syndrome. Much of the variation in forms of treatment (and diagnoses) of this disorder probably results from differences in culture, training, and recognition of an often undiagnosed syndrome of pain, dysfunction, and autonomic dysregulation. The etiology of myofascial pain syndrome associated with trigger points is incompletely understood. Some clinicians believe that it characteristically results from either an acute episode of muscle overload or from chronic and/or repetitive muscle overload. Active myofascial trigger points (MTrPs), which cause pain, exhibit marked localized tenderness and often refer pain to distant sites and disturb motor function. In addition, MTrPs may produce autonomic changes.
For clinical identification of MTrPs, the clinician palpates a localized tender spot in a nodular portion of a taut ropelike band of muscle fibers. Pressure over a trigger point elicits pain at that area and also may elicit pain at a site distant from the point under the fingertip (in a phenomenon known as referred pain). Upon palpation, MTrPs also elicit pain that mirrors the patient's experience. Applied pressure often evokes from the patient the response, "That's my pain!" Insertion of a needle, abrupt palpation, or even a brisk tap with the fingertip directly over the trigger point may result in a brief muscle contraction that is detectable by the examiner. This rapid contraction of muscle fibers of the ropelike taut band is termed a local twitch response.
In muscles that move a relatively small mass or are large and superficial (eg, finger extensors, gluteus maximus), the response is seen easily and may cause the limb to jump when the examiner introduces a needle into the trigger point. Localized abnormal response from the autonomic nervous system may cause piloerection, localized sweating, or regional temperature changes in the skin, attributed to altered blood flow.
Injection of muscles with botulinum toxin has been reported to be effective for myofascial pain caused by trigger points (TrPs) in a few small prospective studies. However, strong evidence of efficacy in larger, multicenter trials is lacking. [8, 31, 32]
A systematic review by Leonardi et al showed mixed results for botulinum toxin injections for upper back myofascial pain syndrome. The researchers suggested, however, that cautious use of botulinum toxin may be warranted, especially for patients with moderate to severe chronic pain and active trigger points. [33]
Botulinum Toxin and the Muscle Spindle: Clinical Issues
Little evidence exists that painful muscle areas, such as TrPs, are associated with structural change or sensory structures, such as the muscle spindle; however, the spindle is intimately involved in certain conditions of abnormal muscle activity. In the spastic condition, for example, the stretch reflex is enhanced for a variety of reasons, such as lack of inhibition from spinal cord interneurons. Whatever the reason, muscle spindle physiology is an important regulator of muscle tone in the spastic condition.
BoNT-A has been recognized to reduce pain associated with various clinical conditions, including craniocervical dystonia, tension headaches, cervicogenic headaches, and migraine, an effect that has been observed independently of the toxin's effect on muscle relaxation. (As stated above, however, controversy exists regarding botulinum toxin's effectiveness in the treatment of headache.) [27, 29, 34, 35, 36, 37, 38]
Importantly, BoNT-A has been shown to inhibit release of neurotransmitters involved in pain transmission, including glutamate and substance P in rats. A formalin-induced pain model in rats has helped to show that a local peripheral injection of BoNT-A can significantly reduce glutamate release, signs of pain, and local edema without inducing muscle weakness. These preclinical observations have yet to be definitively confirmed in human patients; however, they provide a possible rationale for BoNT-A's use in chronic painful conditions, including chronic myofascial pain syndromes.
When to Consider Botulinum Toxin
Indications for botulinum treatment are not entirely clear for patients with myofascial pain syndrome. These patients may be considered candidates for botulinum toxin if they have not responded to traditional forms of treatment, have had a chronic refractory problem for 3 months or longer, have had a complete medical workup to rule out other nonmuscular causes for their pain, and have clearly defined TrPs.
The clinician should proceed with caution before considering using botulinum toxin in the treatment of a patient with myofascial pain. Remember that use of BoNT-A for the treatment of pain is only approved in the United States for pain related to cervical dystonia. Use of BoNT-A for myofascial pain, therefore, is an off-label use and may be considered most appropriate only for patients with a condition that does not respond to, or is judged inappropriate for, more conservative treatment. Factors that may identify a myofascial pain syndrome as potentially responding favorably to botulinum toxin injections include muscle hypertrophy, neurogenic and/or vascular compression, anatomic localization that isolates the target muscle from other structures, and more than 1 outcome measure to determine the efficacy of treatment. One such condition that meets these criteria is termed piriformis muscle syndrome (PMS).
Botulinum Toxin Use in Piriformis Muscle Syndrome
PMS is a controversial myofascial pain condition that presents with seemingly bizarre symptoms. Patients typically are female, have a recent history of trauma to the buttocks or pelvis (usually from a fall), and complain of deep pain in the buttocks and hip, radiating into the thigh or even into the leg and foot. These characteristic signs and symptoms may be from sciatic nerve compression by a contracted piriformis muscle as the nerve passes through the pelvis. Although some clinicians believe this diagnosis is controversial, several peer-reviewed articles cite clinical, anatomic, and electrophysiologic evidence for this distinct condition causing low back and leg pain.
On clinical examination, pressure over the buttocks at a point midway between the sacrum and greater trochanter of the hip reproduces the patient's pain complaint. Since the piriformis muscle is so deep, some clinicians say that palpation of this TrP can be performed properly only by rectal or vaginal examination. Palpation of the TrP on the posterolateral portion of the rectal (or vaginal) vault elicits pain at the site of compression and refers pain either into the thigh or down the leg.
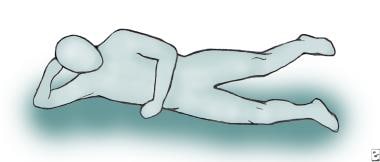
The Beatty maneuver (see image below) also is a helpful clinical method of reproducing the patient's pain in this condition. [39] The patient is asked to lie on the nonpainful side and abduct the thigh by moving the painful leg off the table. This maneuver effectively contracts the piriformis muscle and should reproduce the patient's pain in the buttocks; however, since the syndrome essentially causes sciatic nerve compression at the level of the hip, other causes of sciatica should be ruled out (eg, herniated lumbar disc).
One helpful diagnostic aid is electromyography. In a patient with radiculopathy and sciatica, an electromyographic examination should reveal abnormal spontaneous electrical activity in the extensor muscles of the back. In piriformis syndrome, the electromyogram (EMG) is classically normal. If there is enough sciatic nerve compression to cause axon loss, the abnormalities should be in the muscles distal to the piriformis, and no electrical activity should be seen in the back muscles. A special nerve conduction test, H reflex, has been reported to demonstrate abnormalities in piriformis syndrome when abduction, internal rotation, and flexion of the thigh compress the sciatic nerve; however, this result has not been reproduced by other clinicians. Making a reliable diagnosis in piriformis syndrome is almost impossible; thus, treatment also is difficult.
In some patients, if conservative treatment of piriformis syndrome fails, local injections of anesthetics and/or steroids should be considered. Surgical resection of the piriformis muscle is an additional option; however, some patients may gain short-term benefits from local TrP injections into the muscle without responding to other treatment for long-term pain control. This subset of patients may benefit from treatment with BoNT-A. (See image below.)
 Left piriformis muscle, posterior view. Inject 100 U botulinum toxin type A (BOTOX®) diluted in 3 mL saline into the area marked with an 'X' when guided by fluoroscopy.
Left piriformis muscle, posterior view. Inject 100 U botulinum toxin type A (BOTOX®) diluted in 3 mL saline into the area marked with an 'X' when guided by fluoroscopy.
A limited number of studies assess the efficacy of botulinum toxin in the treatment of piriformis syndrome. [8] For example, Childers and colleagues reported findings from a double-blind placebo-controlled crossover pilot study of BoNT-A injection for refractory piriformis syndrome in 9 subjects. [40] All patients in this study reported pain intensity greater than 3/10 on visual analog pain scales (VASs) after at least 3 months of failed conservative treatment for PMS prior to enrollment. Symptomatic muscle in each patient was injected with 100 U BoNT-A or placebo (saline), using fluoroscopic and electromyographic guidance. Ten weeks later, saline or BoNT-A injections were repeated. The main outcome measures were VAS of pain intensity, distress, spasm, and interference with daily activities.
At baseline, no differences were detected between groups, yet significant (P< .05) differences were observed between the average of 2 minimum VAS at baseline and the average of 2 minimum VAS (in all categories) under the 10-week treatment (BoNT-A) arm, but not the 10-week placebo arm. In addition, BoNT-A treatment average was improved significantly (P = .0273), from baseline/washout average in VAS of daily activities. Data also suggested that a significant (P = .0547) improvement in VAS in muscle spasm (P = .0547) occurred in the BoNT-A group but not in the placebo group. Taken together, these findings demonstrated that, compared to intramuscular saline, BoNT-A injections reduced some, but not all, reports of pain attributed to chronic PMS.
A meta-analysis by Hilal et al that compared botulinum toxin injection with local anesthetic plus corticosteroid, local anesthetic, and corticosteroid injection therapy showed that injection of local anesthetics plus a corticosteroid provided the most effective pain relief in patients with piriformis syndrome. [41] The results of a systematic review by Koh and Tan suggested that botulinum toxin is a safe option for pain reduction in patients with piriformis syndrome; however, insufficient data exist to quantify pain relief, and the optimal dose of botulinum toxin is unclear. [42]
Injection Methods
Therapy with botulinum toxin should be individualized for the patient and the clinician. The equipment needs should be determined according to the needs of the patient, the clinician's training, and the anatomic target for injection. For example, treatments for blepharospasm usually are given by simple subcutaneous injections around the eye without the use of special equipment; however, injections into the deep compartments of the low back, such as the psoas major muscle compartment, may require the use of special imaging techniques.
A 1.0 mL tuberculin-type syringe with 5/8-inch 25-gauge needle is adequate for superficial muscles. For small muscles (eg, facial muscles), a 1-inch 30-gauge needle is sufficient. For larger muscles, such as the hamstrings, a 1-inch or 1.5-inch 25-gauge needle is adequate.
For most limb muscles, the use of electromyography or motor point stimulation (e-stim) is recommended to identify muscles, particularly the smaller muscles in the forearm. For example, a commonly injected finger flexor muscle, the flexor digitorum sublimis (FDS), is nearly impossible to locate without electromyographic guidance. For the clinician who is developing his or her skills in identifying specific muscles for injection with botulinum toxin, the use of simple, audio-only electromyography may enhance the clinician's understanding of functional anatomy and aid the clinician in making decisions on injection localization. For muscles requiring electromyographic guidance, a cannulated monopolar needle cathode, through which botulinum toxin can be injected, is used. Surface reference (anode) and ground electrodes should be placed near the cathode needle.
After placing the patient in a position where the desired muscle can be relaxed, the motor point should be located. Botulinum toxin then can be given after aspiration to prevent intravascular injection. Alcohol, if used to clean the skin, should be allowed to dry completely to prevent toxin deactivation. The use of operating rooms or special procedure (sterile) rooms equipped with monitoring devices for the purpose of intramuscular injections using small caliber needles is not necessary. Most patients can be treated safely in an office setting by experienced clinicians.
Postinjection follow-up
If any discomfort or pain occurs over 24-48 hours after injection, muscle relaxants or acetaminophen may be given. Stronger analgesics usually are not required.
Questions & Answers
Overview
What is the role of botulinum toxin in pain management?
What are the FDA approved indications for botulinum toxins?
What are the mechanisms of action for botulinum toxins in pain management?
What is the median lethal dose (LD50) of botulinum toxin?
What are the possible adverse effects of botulinum toxin?
What is the role of botulinum toxin in pain management for neuromuscular disorders?
What is the efficacy of botulinum toxin in the treatment of myofascial pain?
What is the role of botulinum toxin in the treatment of muscle spindle-related conditions?
When is botulinum toxin indicated in the treatment of myofascial pain syndrome?
What is the role of botulinum toxin in the treatment of piriformis muscle syndrome?
How is botulinum toxin administered for pain management?
What is included in the postinjection care following administration of botulinum toxin?
-
The Beatty maneuver.
-
Left piriformis muscle, posterior view. Inject 100 U botulinum toxin type A (BOTOX®) diluted in 3 mL saline into the area marked with an 'X' when guided by fluoroscopy.
Tables

What would you like to print?
- Overview
- Pharmacology of Botulinum Toxin
- Use of Botulinum Toxin in Painful Neuromuscular Disorders
- Botulinum Toxin and Myofascial Pain
- Botulinum Toxin and the Muscle Spindle: Clinical Issues
- When to Consider Botulinum Toxin
- Botulinum Toxin Use in Piriformis Muscle Syndrome
- Injection Methods
- Questions & Answers
- Show All
- Media Gallery
- References





