Practice Essentials
Autonomic dysreflexia is a potentially dangerous and, in rare cases, lethal clinical syndrome that develops in individuals with spinal cord injury (SCI), resulting in acute, uncontrolled hypertension. All caregivers, practitioners, and therapists who interact with individuals with spinal cord injuries must be aware of this syndrome, recognize the symptoms, and understand the causes and treatment algorithm. [1, 2, 3]
Briefly, autonomic dysreflexia develops in individuals with a neurologic level of SCI at or above the sixth thoracic vertebral level (T6). Autonomic dysreflexia causes an imbalanced reflex sympathetic discharge, leading to potentially life-threatening hypertension. It is considered a medical emergency and must be recognized immediately. If left untreated, autonomic dysreflexia can cause seizures, retinal hemorrhage, pulmonary edema, renal insufficiency, myocardial infarction, cerebral hemorrhage, and, ultimately, death. Complications associated with autonomic dysreflexia result directly from sustained, severe peripheral hypertension. (See the image below.)
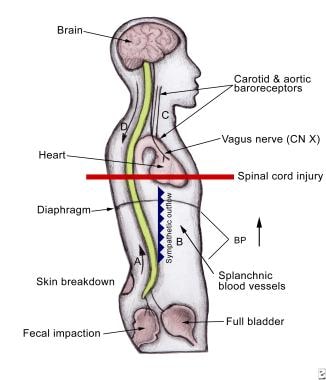 (A) A strong sensory input (not necessarily noxious) is carried into the spinal cord via intact peripheral nerves. The most common origins are bladder and bowel. (B) This strong sensory input travels up the spinal cord and evokes a massive reflex sympathetic surge from the thoracolumbar sympathetic nerves, causing widespread vasoconstriction, most significantly in the subdiaphragmatic (or splanchnic) vasculature. Thus, peripheral arterial hypertension occurs. (C) The brain detects this hypertensive crisis through intact baroreceptors in the neck delivered to the brain through cranial nerves IX and X. (D) The brain attempts two maneuvers to halt the progression of this hypertensive crisis. First, the brain attempts to shut down the sympathetic surge by sending descending inhibitory impulses. These impulses are unable to travel to most sympathetic outflow levels because of the spinal cord injury at T6 or above. Inhibitory impulses are blocked in the injured spinal cord. In the second maneuver, the brain attempts to bring down peripheral blood pressure by slowing the heart rate through an intact vagus (parasympathetic) nerve; however, this compensatory bradycardia is inadequate and hypertension continues. In summary, the sympathetics prevail below the level of neurologic injury, and the parasympathetic nerves prevail above the level of injury. Once the inciting stimulus is removed, reflex hypertension resolves.
(A) A strong sensory input (not necessarily noxious) is carried into the spinal cord via intact peripheral nerves. The most common origins are bladder and bowel. (B) This strong sensory input travels up the spinal cord and evokes a massive reflex sympathetic surge from the thoracolumbar sympathetic nerves, causing widespread vasoconstriction, most significantly in the subdiaphragmatic (or splanchnic) vasculature. Thus, peripheral arterial hypertension occurs. (C) The brain detects this hypertensive crisis through intact baroreceptors in the neck delivered to the brain through cranial nerves IX and X. (D) The brain attempts two maneuvers to halt the progression of this hypertensive crisis. First, the brain attempts to shut down the sympathetic surge by sending descending inhibitory impulses. These impulses are unable to travel to most sympathetic outflow levels because of the spinal cord injury at T6 or above. Inhibitory impulses are blocked in the injured spinal cord. In the second maneuver, the brain attempts to bring down peripheral blood pressure by slowing the heart rate through an intact vagus (parasympathetic) nerve; however, this compensatory bradycardia is inadequate and hypertension continues. In summary, the sympathetics prevail below the level of neurologic injury, and the parasympathetic nerves prevail above the level of injury. Once the inciting stimulus is removed, reflex hypertension resolves.
Signs and symptoms of autonomic dysreflexia
A patient with autonomic dysreflexia may have one or more of the following findings on physical examination:
-
Significant rise in systolic and diastolic blood pressure greater than 20 mm Hg systolic or 10 mm Hg diastolic, above baseline
-
Profuse sweating above the level of lesion - Especially in the face, neck, and shoulders; rarely occurs below the level of the lesion because of sympathetic activity
-
Goose bumps below the level of the lesion
-
Flushing of the skin above the level of the lesion - Especially in the face, neck, and shoulders; this is a frequent symptom
-
Blurred vision
-
Nasal congestion - A common symptom
Management of autonomic dysreflexia
This includes the following:
-
Check the patient's blood pressure; if the blood pressure is elevated, have the person sit up immediately and loosen any clothing or constrictive devices
-
If an indwelling urinary catheter is not in place, catheterize the patient
-
If the individual has an indwelling urinary catheter, check the system along its entire length for kinks, folds, constrictions, or obstructions and for correct placement
-
If the catheter appears to be blocked, gently irrigate the bladder with a small amount of fluid, such as normal saline at body temperature
-
If the catheter is draining and blood pressure remains elevated, suspect fecal impaction, the second most common cause of autonomic dysreflexia, and check the rectum for stool, using lidocaine jelly as lubricant; if impacted, gentle manual evacuation is recommended
-
Monitor blood pressure and pulse every 2-5 minutes until the patient has stabilized
-
Use of an antihypertensive agent is recommended when the systolic blood pressure is at or above 150 mm Hg; once the offending agent is identified and corrected, the autonomic dysreflexia subsides and blood pressure returns to normal (systolic, 90-110 mm Hg), so medicating with a short-acting antihypertensive is of utmost importance
-
Monitor the individual's symptoms and blood pressure for at least 2 hours after resolution of the autonomic dysreflexia episode to ensure that elevation of blood pressure does not recur
Pathophysiology
The autonomic nervous system is the division of the peripheral nervous system that carries motor information to the visceral organs and glands. It includes the sympathetic and parasympathetic autonomic nervous systems. The sympathetic fibers are responsible for the fight-or-flight response and divert blood flow away from the gastrointestinal tract and skin through the process of vasoconstriction. As a result, blood flow to skeletal muscles and lungs is significantly enhanced (by as much as 1200% in the case of skeletal muscles). [6] This also causes bronchiolar dilatation of the lung, which allows for greater alveolar oxygen exchange and increases the heart rate and contractility of cardiac myocytes.
The parasympathetic fibers typically act in opposition of the sympathetic autonomic nervous system through negative feedback control. This action is a complementary response, causing a balance of sympathetic and parasympathetic responses. Overall, the parasympathetic outflow results in conservation and restoration of energy, reduction in heart rate and blood pressure, facilitation of digestion and absorption of nutrients, and excretion of waste products. This parasympathetic response is primarily mediated through cranial nerve X, the vagus nerve, and the S2, S3, and S4 spinal nerves.
In individuals with intact central and peripheral nervous systems, a noxious stimulus results initially in a sympathetic response, leading to elevation in heart rate and blood pressure primarily through spinal reflexes. This response is modulated by the central nervous system and peripheral baroreceptors through the parasympathetic nervous system; this results in heart rate and blood pressure control both through direct responses by the vagus nerve and through inhibitory spinal cord signals. An appropriate balance of sympathetic and parasympathetic outflow is attained and modulated by both the central and peripheral nervous systems.
In those with an SCI at the level of T6 and above, a noxious (or otherwise strong) stimulus below the level of injury results in an unbalanced physiologic response. The strong stimulus causes a peripheral sympathetic response through spinal reflexes, resulting in vasoconstriction below the level of injury. This reflex response ascends and descends the spinal cord and paraspinal sympathetic ganglia, causing both direct vasoconstriction through activation of perivascular receptors and systemic/indirect vasoconstriction through stimulation of the adrenal medulla, resulting in epinephrine and norepinephrine release into the systemic circulation. This therefore results in hypertension, primarily through splanchnic and peripheral vasoconstriction.
The baroreceptors in the carotid sinus and aortic arch convey appropriate responses to hypertension through the petrosal ganglion to the nucleus ambiguous and result in strong vagal (CN X) outflow, bradycardia, and vasodilatation above the level of injury. The central nervous system cannot directly detect the strong or noxious signal below the level of injury (owing to the lack continuity of the ascending sensory fibers from the underlying SCI), and, therefore, responds to hypertension by sending a strong inhibitory response through the spinal cord aimed at reducing the sympathetic response. However, because of the lack of spinal cord continuity, the descending inhibitory response only travels as far as the level of neurologic injury and does not cause the desired response in the sympathetic fibers below the injury; therefore, the hypertension remains uncontrolled.
As a result, there is flushing and sweating only above the level of injury, bradycardia, pupillary constriction, and nasal congestion (unopposed parasympathetic responses); and below the level of injury, there is pale, cool skin and piloerection due to sympathetic tone and lack of the descending inhibitory parasympathetic modulation. [7] (However, a study by Solinsky et al of 78 male patients with SCI who had incidents of autonomic dysfunction found that out of 445 episodes, relative tachycardia occurred in 68.0%, far more frequently than relative bradycardia [0.3%]. [8] )
T6 is of particular importance in the pathogenesis of autonomic dysreflexia. The splanchnic vascular bed is one of the body’s largest reserves of circulatory volume and is controlled primarily by the greater splanchnic nerve. This important nerve derives its innervation from T5-T9. Lesions to the spinal cord at or above T6 allow the strong and uninhibited sympathetic tone to constrict the splanchnic vascular bed, causing systemic hypertension. Lesions below T6 generally allow enough descending inhibitory parasympathetic control to modulate the splanchnic tone and prevent hypertension.
The underlying pathophysiological changes that occur in the spinal cord and in the periphery that cause autonomic dysreflexia have not been fully elucidated in a human model. It has been postulated that peripheral alpha-adrenergic receptors associated with blood vessels become hyperresponsive below the level of the spinal cord lesion. This hyperresponsiveness is secondary to a low resting catecholamine state associated with SCI. The orphaned receptors have a decreased threshold to react to adrenergic stimuli and react with an increased responsiveness. [9, 10, 11]
Another possible mechanism includes loss of supraspinal inhibitory control from the medulla oblongata–bulbospinal pathways; this loss of supraspinal control may cause a loss of the bulbospinal pathway’s inhibitory effect over serotonin in the intermediolateral nucleus of the spinal cord. The unabated serotonin then causes strong vasoconstriction. [12]
A study by Phillips et al suggested that the brain may buffer moderate instances of autonomic dysreflexia. During spontaneous episodes of autonomic dysreflexia in four patients with motor-complete cervical SCI, the report found that although the mean arterial blood pressure rose from 66 to 83 mm Hg, the cerebral blood flow and end-tidal partial pressure of carbon dioxide remained approximately the same. [13]
Causes of Autonomic Dysreflexia
Episodes of autonomic dysreflexia can be triggered by many potential causes. [14] Essentially, any painful, irritating, or even strong stimulus below the level of the injury can cause an episode of autonomic dysreflexia. Bladder distention or irritation is responsible for 75-85% of the cases. [15] Bladder irritation is commonly caused by a blocked or kinked catheter or failure of a timely intermittent catheterization program. The second most common cause of autonomic dysreflexia is bowel distention, usually due to fecal impaction. This accounts for 13-19% of cases. [15] Although the list is not comprehensive, the following events or conditions all can cause episodes of autonomic dysreflexia:
-
Bladder distention
-
Urinary tract infection
-
Calculus
-
Cystoscopy/instrumentation
-
Epididymitis or scrotal compression
-
Bowel distention
-
Fecal impaction
-
Bowel instrumentation/colonoscopy
-
Reflux or gastritis
-
Gallstones
-
Gastric ulcers
-
Invasive testing
-
Hemorrhoids
-
Gastrocolic irritation
-
Appendicitis or other intra-abdominal pathology/trauma
-
Anal fissure
-
Menstruation
-
Pregnancy - Especially labor and delivery
-
Vaginitis
-
Sexual intercourse [17]
-
Ejaculation
-
Deep vein thrombosis
-
Pulmonary emboli
-
Pressure ulcers
-
Ingrown toenail
-
Burns or sunburn
-
Blisters
-
Insect bites
-
Contact with hard or sharp objects
-
Temperature fluctuations
-
Constrictive clothing, shoes, or appliances
-
Heterotopic bone
-
Fractures or other skeletal trauma
-
Surgical or diagnostic procedures
Michael et al reported that maladaptive propriospinal neuron plasticity below complete high thoracic SCI may be essential to the development of autonomic dysreflexia. [18]
A literature review by Liu et al indicated that in patients with SCI, autonomic dysreflexia triggers from the lower urinary tract are often associated with clinical urologic procedures, suggesting that blood pressure monitoring should be routinely performed during such procedures. The study found, for example, that 36.7-77.8% of patients undergoing urodynamic testing experienced autonomic dysreflexia, with the problem also occurring in most patients when cystoscopy, transurethral litholapaxy, or extracorporeal shock-wave lithotripsy were performed without anesthesia. The investigators also found that autonomic dysreflexia occurred more often in patients with cervical SCI than in those with thoracic SCI. [19]
A study by Vírseda-Chamorro et al indicated that in performing a urodynamic exam in patients with an SCI above T6, independent risk factors for sudden onset of autonomic dysreflexia consist of patient age of 45 years or above and a maximum detrusor voiding pressure of 31 cm H2O or above. [20]
A study by Xiong et al of 89 patients indicated that in individuals with SCI who undergo cystolitholapaxy, autonomic dysreflexia is more likely to occur in those with larger or a greater number of bladder stones, an injury level above T6, a greater hydraulic irrigation height, and a longer surgical time. [21]
Prognosis
Complications and morbidity associated with autonomic dysreflexia result directly from sustained, severe peripheral hypertension and include retinal/cerebral hemorrhage, myocardial infarction, and seizures. Mortality is rare.
Using an autonomic dysreflexia questionnaire scored from 0 to 24, a cross-sectional study by Stoffel et al reported that in adults with SCI, every point added to the score increased the likelihood of more severe bowel symptoms by 5 percent. [22]
In a literature review, Wan and Krassioukov identified the prevalence of various causes of life-threatening complications and death from autonomic dysreflexia in SCI, determining that central nervous system (CNS)–related causes were the most frequent. The investigators found that out of 32 patients identified as having either died or suffered life-threatening complications from autonomic dysreflexia, the prevalence of CNS-, cardiovascular-, and pulmonary-related causes were as follows [23] :
-
CNS: 23 patients (72%)
-
Cardiovascular: Seven patients (22%)
-
Pulmonary: Two patients (6%)
Seven patients in the study died directly owing to complications from an attack of autonomic dysreflexia. [23]
Patient education
All medical professionals should educate the patient and family members or caregivers about this potentially life-threatening complication of SCI. [24] Such instruction should include prevention strategies, signs and symptoms of autonomic dysreflexia, and proper management of the condition. Patients should be encouraged to carry a wallet-sized card explaining symptoms and treatment for autonomic dysreflexia. Such cards can be found from multiple sources, including the following:
Consultations
If the cause of the episode of autonomic dysreflexia is not found and blood pressure remains elevated, emergency department care is recommended for medication management, close monitoring, and further investigation of the possible cause. Consult an ICU specialist for ICU monitoring and treatment of the hypertension. Physicians specializing in physical medicine and rehabilitation are well-acquainted with the diagnosis and management of autonomic dysreflexia and can be of assistance in both acute management and prevention strategies of this syndrome.
Prevention
Proper bladder and bowel care (ie, preventing fecal impaction, bladder distention) are mainstays in preventing episodes of autonomic dysreflexia. Regulation of the bladder routine via indwelling Foley catheter or intermittent catheterization and regular urologic follow-up is highly recommended for autonomic dysreflexia prevention. A regular bowel program to ensure appropriate fecal movement and prevent constipation is important. (A study by Inskip et al found that among patients with SCI at T7 or above, 74% experienced autonomic dysreflexia symptoms during bowel care. [25] )
Autonomic dysreflexia caused by anorectal procedures, including the bowel program, or from intermittent bladder catheterization may be diminished with the use of prophylactic lidocaine or dibucaine. [14]
However, a study by Lucci et al indicated that lidocaine lubricant, by hindering reflex bowel emptying, lengthens the duration of at-home bowel care in patients with SCI and increases the burden of autonomic dysreflexia. The higher burden was indicated by a greater level and longer duration of high systolic arterial pressure in the lidocaine lubricant group than in patients treated with a placebo. [26]
Patients with SCI should be educated to recognize the early symptoms of autonomic dysreflexia and understand the common causes and management. Those with recurrent symptoms should be educated on home blood pressure monitoring.
Epidemiology
Reported prevalence rates vary for autonomic dysreflexia in the United States, but the generally accepted rate is 48-90% of all individuals who are injured at T6 and above. Patients who have a complete injury (no motor or sensation below the level of the spinal cord lesion) have a much higher incidence of autonomic dysreflexia (91% with complete injury vs 27% with incomplete injury 27%). [27] In a Korean study, by Lee and Joo, 26 out of 28 patients (93%) with SCI above T6 were found to have autonomic dysreflexia, as measured using ambulatory blood pressure monitoring. However, several individuals with autonomic dysreflexia appeared to be asymptomatic. Twenty-four patients had motor-incomplete SCI, while four had motor-complete injury. [28]
The occurrence of autonomic dysreflexia increases as the patient evolves out of spinal shock. With the return of sacral reflexes, the possibility of autonomic dysreflexia increases. [24] Autonomic dysreflexia occurs during labor in approximately two thirds of pregnant women with an SCI above the level of T6. Spinal epidural anesthesia can help reduce the risks of autonomic dysreflexia during pregnancy.
The male-to-female ratio for sustaining SCI is 4:1; however, autonomic dysreflexia has no sexual predilection.
History and Physical Examination
History
The patient with autonomic dysreflexia generally gives a history of one or many of the following symptoms: Headaches, blurry vision, spots in the visual field, nasal congestion, blotchy skin above the level of injury, and a sense of anxiety or malaise. Feelings of apprehension or anxiety over an impending physical problem commonly are exhibited.
Physical examination
A patient with autonomic dysreflexia may have one or more of the following findings on physical examination:
-
Significant rise in systolic and diastolic blood pressure greater than 20 mm Hg systolic or 10 mm Hg diastolic, above baseline (The sudden rise in blood pressure in autonomic dysreflexia is usually associated with bradycardia. Normal systolic blood pressure for an individual with an SCI above T6 is 90-110 mm Hg; blood pressure of 20-40 mm Hg above the reference range for such patients may be a sign of autonomic dysreflexia. However, patients with autonomic dysreflexia may display no symptoms, despite elevated blood pressure.)
-
Profuse sweating above the level of the lesion - Especially in the face, neck, and shoulders; rarely occurs below the level of the lesion because of sympathetic activity
-
Goose bumps below the level of the lesion
-
Flushing of the skin above the level of the lesion - Especially in the face, neck, and shoulders; this is a frequent symptom
-
Blurred vision
-
Nasal congestion - A common symptom
Physical Therapy
Physical therapists who treat patients with SCI need to have a good understanding of autonomic dysreflexia and be familiar with the signs and symptoms of this potentially life-threatening condition. [24] Throughout the physical therapy sessions, the therapist needs to monitor the urinary catheter for any blockage or twisting.
If the patient becomes hypertensive during therapy and autonomic dysreflexia is the suspected cause, the therapist should place the patient in an upright position immediately. This takes advantage of an orthostatic response and helps with the pooling of blood in the lower extremities. The therapist needs to complete careful inspection to identify the source of painful stimuli (eg, catheter, restrictive clothing, leg bag straps, abdominal supports, orthoses). [14] A less common cause of autonomic dysreflexia during physical therapy sessions may originate with muscle stretching, either from range-of-motion or passive stretching.
If the patient develops autonomic dysreflexia, the physical therapist needs to treat it as a medical emergency and be familiar with established protocols for medical management within his or her particular setting. The individual therapy session then must be discontinued to allow the patient to stabilize and recover. Please refer to Guidelines of the Consortium for Spinal Cord Medicine for the management of autonomic dysreflexia if no guidelines are available at your facility.
Occupational Therapy
Occupational therapy is another discipline involved extensively in the rehabilitation of individuals with SCI. The occupational therapist also must be familiar with the signs and symptoms of autonomic dysreflexia and be able to respond quickly if the condition develops during a therapy session. [24]
Occupational therapists perform extensive training in the performance of activities of daily living with patients who have sustained SCI. Such activities include proper bowel and bladder management, which can help to prevent to the occurrence of autonomic dysreflexia. The occupational therapist may be involved in establishing a regular bowel program and may complete patient and family/caregiver education on this aspect of care.
Both occupational and physical therapists should educate the patient and family members about autonomic dysreflexia and ensure that they are familiar with prevention strategies, signs and symptoms, and proper management of the condition.
Recreational and Speech Therapies
Recreational therapy
Recreational therapists also are important members of the rehabilitation team, as they help patients with SCI to become involved in recreational, community, and social activities. As members of the SCI team, they also must be knowledgeable about autonomic dysreflexia and know how to respond appropriately if the patient develops symptoms during a recreational therapy session. [24]
Speech therapy
Generally, the treatment provided by the speech therapist is not associated with any painful stimuli below the lesion that may precipitate an autonomic dysreflexia response. However, as health care providers involved in the treatment of individuals with SCI, speech therapists must be familiar with the manifestations of this potentially life-threatening condition. [24]
Treatment of Autonomic Dysreflexia
Check the patient's blood pressure. If the blood pressure is elevated, have the person sit up immediately and loosen any clothing or constrictive devices. Sitting allows some gravitational pooling of blood in the lower extremities and reduces blood pressure. Survey the person for instigating causes, beginning with the urinary system, the most common cause of autonomic dysreflexia. [4, 5]
If an indwelling urinary catheter is not in place, catheterize the patient. If the individual has an indwelling urinary catheter, check the system along its entire length for kinks, folds, constrictions, or obstructions and for correct placement.
If the catheter appears to be blocked, gently irrigate the bladder with a small amount of fluid, such as normal saline at body temperature. Avoid manually compressing or tapping on the bladder. If the catheter is draining and blood pressure remains elevated, suspect fecal impaction, the second most common cause of autonomic dysreflexia, and check the rectum for stool, using lidocaine jelly as lubricant. If impacted, gentle manual evacuation is recommended.
Monitor blood pressure and pulse every 2-5 minutes until the patient has stabilized; impaired autonomic regulation can cause blood pressure to fluctuate quickly during an episode of autonomic dysreflexia.
Use of an antihypertensive agent is recommended when the systolic blood pressure is at or above 150 mm Hg. Once the offending agent is identified and corrected, the autonomic dysreflexia subsides and blood pressure returns to normal (systolic, 90-110 mm Hg). For this reason, medicating with a short-acting antihypertensive is of utmost importance.
The most commonly used agents are nifedipine and nitrates (eg, nitroglycerine paste or sublingual nitroglycerine). [29] Nifedipine should be in the immediate-release form; bite and swallow is the preferred method of administering the drug, not sublingual administration. Other agents used are prazosin, captopril, terazosin, mecamylamine, diazoxide, and phenoxybenzamine. Use antihypertensives with extreme caution in older persons or in people with coronary artery disease. Note that men with SCI often use cGMP-specific phosphodiesterase type 5 (PDE5) inhibitors (eg, sildenafil, vardenafil, tadalafil.) for sexual dysfunction. Use of nitrates is contraindicated in this situation.
If there is poor response to treatment and/or if the cause of the autonomic dysreflexia has not been identified, the patient should be seen in an emergency department for monitoring and pharmacologic control of blood pressure. The emergency department has better access to the necessary tests to investigate the possible etiology of the autonomic dysreflexia.
Monitor the individual's symptoms and blood pressure for at least 2 hours after resolution of the autonomic dysreflexia episode to ensure that elevation of blood pressure does not recur. Autonomic dysreflexia may resolve because of medication, not because of resolution of the underlying cause. Unless the underlying cause is identified and addressed, recurrence should be expected.
There is evidence that electrical stimulation of the spinal cord may be a useful therapy for autonomic dysreflexia as well as for orthostatic hypotension. Although it is not completely clear why such stimulation can aid autonomic dysreflexia, the treatment may activate inhibitory circuits, reducing the overactive sympathetic response. [30] Research has suggested, for example, that a net inhibitory response results from epidural spinal cord stimulation in the lumbosacral region, serving as a preventative for autonomic dysreflexia and occurring “either through inhibition of dorsal neuron firing and activation or activation of inhibitory interneurons.” [31]
Prevention of Autonomic Dysreflexia
Patients who have previously experienced autonomic dysreflexia may be able to prevent the reoccurrence by using simple prevention strategies. The prevention strategies may mitigate further episodes of autonomic dysreflexia. Common triggers are as follows.
Bladder
Intermittent catheterization should be regular and timely; only clean catheters should be used. Indwelling catheters should be changed routinely and regularly checked for blockage or kinking. Detrusor sphincter dyssynergia causing autonomic dysreflexia may be treated with intravesicular onabotulinumtoxinA or intravesicular capsaicin. [32] A study by Fougere et al indicated that onabotulinumtoxinA injections into the detrusor of patients with high-level SCIs (one cycle of 200 U) can reduce the severity and frequency of episodes of bladder-related autonomic dysreflexia. The study included 17 patients with chronic, traumatic SCIs at the sixth thoracic level or above. Following injection, autonomic dysreflexia was found to be less severe during urodynamic study and to occur less frequently over a monitored 24-hour period. [33]
Other successful methods trialed to help prevent autonomic dysreflexia are sacral denervation and sphincterotomy.
Bowels
A regular bowel program is essential for the prevention of constipation, impaction, and ileus. Prior to a bowel procedure, an anal block helps prevent autonomic dysreflexia. [34] Topical lidocaine may be of help.
Labor and delivery
Spinal anesthesia can help to prevent autonomic dysreflexia.
Pressure ulcers
Routine weight shifts and skin checks are necessary to prevent ulceration. Any skin breakdown should be addressed early by a knowledgeable wound care team or physician.
A prospective cohort study by Neuhauser et al found that in patients with spinal cord injury/disorder (SCI/D) who had hospital-acquired pressure injuries, those whose SCI/D had occurred less than a year prior were more likely to develop autonomic dysreflexia than were patients whose SCI/D was older. [35]
Other
A retrospective study by Del Fabro et al indicated that an intrathecal baclofen (ITB) pump can reduce the incidence of autonomic dysreflexia in patients with SCI. The investigators found that prior to ITB pump placement, 25 out of the 34 patients (73.5%) in the study experienced autonomic dysreflexia, compared with two patients (5.9%) following pump placement. [36]
Questions & Answers
Overview
What is autonomic dysreflexia?
What is the autonomic nervous system?
What is the parasympathetic nervous system?
How do the central and peripheral nervous systems interact?
What is the pathophysiology of spinal cord injury leading to autonomic dysreflexia?
What is the role of the central nervous system in the pathogenesis of autonomic dysreflexia?
Which events or conditions cause autonomic dysreflexia?
Which urologic procedures may trigger autonomic dysreflexia?
What are the risk factors for autonomic dysreflexia in a patient who undergo cystolitholapaxy?
What are the morbidities associated with autonomic dysreflexia?
What are complications of autonomic dysreflexia with spinal cord injury?
What information about autonomic dysreflexia should patients with spinal cord injury be given?
How is autonomic dysreflexia prevented?
What is the prevalence of autonomic dysreflexia?
When is autonomic dysreflexia most likely to occur?
How does the prevalence of autonomic dysreflexia vary by sex?
What are the signs and symptoms of autonomic dysreflexia?
Which physical findings are characteristic of autonomic dysreflexia in spinal cord injury?
How should autonomic dysreflexia be managed during physical therapy?
What is the role of occupational therapy in the management of autonomic dysreflexia?
What is the role of a recreational therapist in the management of autonomic dysreflexia?
What is the role of speech therapy in the treatment of autonomic dysreflexia?
What is the role of blood pressure monitoring in the treatment of autonomic dysreflexia?
When is an indwelling urinary catheter indicated in the treatment of autonomic dysreflexia?
Why is it important to monitor BP and pulse during an episode of autonomic dysreflexia?
What is the role of antihypertensive agents in the treatment of autonomic dysreflexia?
Which medications are used in the treatment of autonomic dysreflexia?
When is an emergency department treatment indicated in autonomic dysreflexia?
What monitoring is needed following an episode of autonomic dysreflexia?
How can recurrence of autonomic dysreflexia be prevented?
What is the role of bladder management in the prevention of autonomic dysreflexia?
What is the role of bowel management in the prevention of autonomic dysreflexia?
How is autonomic dysreflexia prevented during labor and delivery?
What is the role of pressure ulcer management in the prevention of autonomic dysreflexia?
What is the role of intrathecal baclofen pump in the prevention of autonomic dysreflexia?
-
(A) A strong sensory input (not necessarily noxious) is carried into the spinal cord via intact peripheral nerves. The most common origins are bladder and bowel. (B) This strong sensory input travels up the spinal cord and evokes a massive reflex sympathetic surge from the thoracolumbar sympathetic nerves, causing widespread vasoconstriction, most significantly in the subdiaphragmatic (or splanchnic) vasculature. Thus, peripheral arterial hypertension occurs. (C) The brain detects this hypertensive crisis through intact baroreceptors in the neck delivered to the brain through cranial nerves IX and X. (D) The brain attempts two maneuvers to halt the progression of this hypertensive crisis. First, the brain attempts to shut down the sympathetic surge by sending descending inhibitory impulses. These impulses are unable to travel to most sympathetic outflow levels because of the spinal cord injury at T6 or above. Inhibitory impulses are blocked in the injured spinal cord. In the second maneuver, the brain attempts to bring down peripheral blood pressure by slowing the heart rate through an intact vagus (parasympathetic) nerve; however, this compensatory bradycardia is inadequate and hypertension continues. In summary, the sympathetics prevail below the level of neurologic injury, and the parasympathetic nerves prevail above the level of injury. Once the inciting stimulus is removed, reflex hypertension resolves.
Tables

What would you like to print?
- Practice Essentials
- Pathophysiology
- Causes of Autonomic Dysreflexia
- Prognosis
- Patient education
- Consultations
- Prevention
- Epidemiology
- History and Physical Examination
- Physical Therapy
- Occupational Therapy
- Recreational and Speech Therapies
- Treatment of Autonomic Dysreflexia
- Prevention of Autonomic Dysreflexia
- Questions & Answers
- Show All
- References






