Overview
Botulinum toxin (abbreviated either as BTX or BoNT) is produced by Clostridium botulinum, a gram-positive anaerobic bacterium. [1] The clinical syndrome of botulism can occur following ingestion of contaminated food, from colonization of the infant gastrointestinal tract, or from a wound infection.
BoNT is broken into 7 neurotoxins (labeled as types A, B, C [C1, C2], D, E, F, and G), which are antigenically and serologically distinct but structurally similar. Human botulism is caused mainly by types A, B, E, and (rarely) F. Types C and D cause toxicity only in animals.
The various botulinum toxins possess individual potencies, and care is required to assure proper use and avoid medication errors. Recent changes to the established drug names by the FDA were intended to reinforce these differences and prevent medication errors. The products and their approved indications include the following:
-
OnabotulinumtoxinA (Botox®, Botox Cosmetic®)
See the list below:
- Botox® - Cervical dystonia, severe primary axillary hyperhidrosis, strabismus, blepharospasm, neurogenic detrusor overactivity, chronic migraine, upper limb spasticity
- Botox Cosmetic® - Moderate to severe glabellar lines, moderate to severe lateral canthal lines, known as crow’s feet
-
AbobotulinumtoxinA (Dysport®) - Upper and lower limb spasticity, cervical dystonia, and moderate-to-severe glabellar lines in adults; it is also indicated for lower limb spasticity in children aged 2 years or older
-
IncobotulinumtoxinA (Xeomin®) - Upper limb spasticity, cervical dystonia, blepharospasm, moderate to severe glabellar lines, chronic sialorrhea
-
PrabotulinumtoxinA (Jeuveau®) - Moderate-to-severe glabellar lines
-
DaxibotulinumtoxinA (Daxxify®) - Moderate-to-severe glabellar lines
-
LetibotulinumtoxinA (Letybo®) - Moderate-to-severe glabellar lines
-
RimabotulinumtoxinB (Myobloc®) - Cervical dystonia
The BoNT molecule is synthesized as a single chain (150 kD) and then cleaved to form the dichain molecule with a disulfide bridge (see image below).
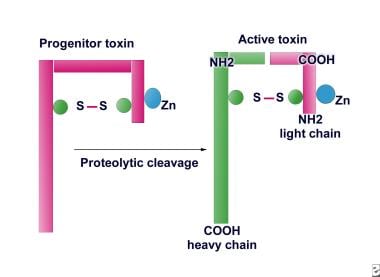
The light chain (~50 kD - amino acids 1-448) acts as a zinc (Zn2+) endopeptidase similar to tetanus toxin with proteolytic activity located at the N-terminal end (see image below). The heavy chain (~100 kD - amino acids 449-1280) provides cholinergic specificity and is responsible for binding the toxin to presynaptic receptors; it also promotes light-chain translocation across the endosomal membrane.
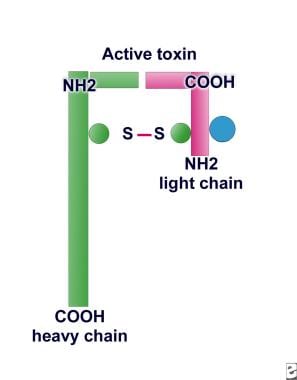 Proteolytic activity is located at the N-terminal end of the light chain of botulinum toxin type A.
Proteolytic activity is located at the N-terminal end of the light chain of botulinum toxin type A.
History
The German physician and poet Justinus Kerner (1786-1862) first developed the idea of a possible therapeutic use of botulinum toxin, which he called "sausage poison." [2]
-
In 1870, Muller (another German physician) coined the name botulism. The Latin form is botulus, which means sausage.
-
In 1895, Professor Emile Van Ermengem, of Belgium, first isolated the bacterium Clostridium botulinum.
-
In 1928, Dr. Herman Sommer, at the University of California, San Francisco, first isolated in purified form botulinum toxin type A (BoNT-A) as a stable acid precipitate.
-
In 1946, Dr. Edward J Schantz succeeded in purifying BoNT-A in crystalline form–cultured Clostridium botulinum and isolated the toxin.
-
In 1949, Dr. Burgen's ASV group discovered that botulinum toxin blocks neuromuscular transmission.
-
In the 1950s, Dr. Vernon Brooks discovered that when BoNT-A is injected into a hyperactive muscle, it blocks the release of acetylcholine from motor nerve endings.
-
In 1973, Dr. Alan B. Scott, of Smith-Kettlewell Eye Research Institute, used BoNT-A in monkey experiments; in 1980, he used BoNT-A for the first time in humans to treat strabismus.
-
In December 1989, BoNT-A (BOTOX®) was approved by the US Food and Drug Administration (US FDA) for the treatment of strabismus, blepharospasm, and hemifacial spasm in patients aged younger than 12 years.
-
On December 21, 2000, BoNT-A received US FDA approval for treatment of cervical dystonia.
-
In 2001, the United Kingdom approved BOTOX®, synthesized by Allergan, for axillary hyperhidrosis (excessive sweating). Canada approved BOTOX® for axillary hyperhidrosis, focal muscle spasticity, and cosmetic treatment of wrinkles at the brow line.
-
On April 15, 2002, the US FDA announced the approval of BOTOX® Cosmetic to temporarily improve the appearance of moderate-to-severe frown lines between the eyebrows (glabellar lines). On July 21, 2011, the US FDA approved incobotulinumtoxinA (Xeomin) for temporary improvement in the appearance of moderate-to-severe glabellar lines, or frown lines between the eyebrows, in adult patients.
-
In July 2004, the US FDA approved BOTOX® to treat severe underarm sweating, known as primary axillary hyperhidrosis that cannot be managed by topical agents, such as prescription antiperspirants.
-
The acceptance of BoNT-A use for the treatment of different chronic pain disorders is growing. However, it has not been approved by the US FDA for any chronic pain conditions except for chronic migraine.
-
The clinical use of BoNT-B has been studied, and several products currently are available commercially (eg, MyoBloc, in the United States; NeuroBloc, in Europe). MyoBloc was approved by the US FDA on December 8, 2000, for treatment of cervical dystonia, to reduce the severity of abnormal head position and neck pain.
-
Use of BoNT-F also is under investigation in patients who have become immunologically resistant to serotypes A and B.
-
On April 29, 2009, abobotulinumtoxinA (Dysport) was approved by the US FDA for the treatment of adults with cervical dystonia to reduce the severity of abnormal head position and neck pain in both toxin-naïve and previously treated patients.
-
On March 9, 2010, the US FDA approved onabotulinumtoxinA (BOTOX®) to treat spasticity in the flexor muscles of the elbow, wrist, and fingers in adults with stroke, traumatic brain injury, or the progression of multiple sclerosis.
-
On August 2, 2010, the US FDA announced the approval of incobotulinumtoxinA (Xeomin®) for the treatment of adults with cervical dystonia, to decrease the severity of abnormal head position and neck pain in both botulinum toxin-naïve and previously treated patients and for blepharospasm in adults previously treated with BOTOX®.
-
On October 15, 2010, the US FDA approved onabotulinumtoxinA (BOTOX®) injection to prevent headaches in adult patients with chronic migraine. Chronic migraine is defined as having a history of migraine and experiencing a headache on most days of the month.
-
On August 24, 2011, the US FDA approved onabotulinumtoxinA (BOTOX®) injection for the treatment of urinary incontinence due to detrusor overactivity associated with a neurologic condition (eg, spinal cord injury, multiple sclerosis) in adults who have an inadequate response to or are intolerant of an anticholinergic medication.
-
On September 11, 2013, the US FDA approved onabotulinumtoxinA (BOTOX®) for the temporary improvement in the appearance of moderate to severe lateral canthal lines, known as crow’s feet. This is the only FDA-approved drug treatment option for lateral canthal lines.
-
On July 16, 2015, the US FDA approved Dysport® (abobotulinumtoxinA) for the treatment of upper limb spasticity (ULS) in adult patients to decrease the severity of increased muscle tone in elbow flexors, wrist flexors and finger flexors.
-
On December 23, 2015, the US FDA approved Xeomin® (incobotulinumtoxinA) for the treatment of upper limb spasticity (ULS) in adult patients.
-
On February 1, 2019, the US FDA approved Jeuveau® (prabotulinumtoxinA) for the temporary improvement in the appearance of moderate-to-severe glabellar lines associated with corrugator and/or procerus muscle activity in adults. [3]
Mechanism of Action
Botulinum toxin acts by binding presynaptically to high-affinity recognition sites on the cholinergic nerve terminals and decreasing the release of acetylcholine, causing a neuromuscular blocking effect. This mechanism laid the foundation for the development of the toxin as a therapeutic tool.
Recovery occurs through proximal axonal sprouting and muscle re-innervation by formation of a new neuromuscular junction. De Paiva and colleagues suggest that eventually the original neuromuscular junction regenerates. [4]
-
BoNT-A and BoNT-E cleave synaptosome-associated protein (SNAP-25), a presynaptic membrane protein required for fusion of neurotransmitter-containing vesicles. [5]
-
BoNT-B, BoNT-D, and BoNT-F cleave a vesicle-associated membrane protein (VAMP), also known as synaptobrevin.
-
BoNT-C acts by cleaving syntaxin, a target membrane protein.
Table 1. Botulinum Toxin Types, Target Sites, Discoverers, and Year Discovered (Open Table in a new window)
Type |
Target |
Discoverer |
Year |
A |
SNAP-25 |
Landman |
1904 |
B |
VAMP |
Ermengem |
1897 |
C1 |
Syntaxin |
Bengston and Seldon |
1922 |
D |
VAMP |
Robinson |
1929 |
E |
SNAP-25 |
Gunnison |
1936 |
F |
VAMP |
Moller and Scheibel |
1960 |
G |
VAMP |
Gimenez and Ciccarelli |
1970 |
Preparations
The different preparations of BoNT-A, onabotulinumtoxinA (BOTOX®; Allergan; Irvine, Calif), abobotulinumtoxinA (Dysport®; Ipsen; Paris, France), incobotulinumtoxinA (Xeomin®; Merz Pharmaceuticals, Frankfurt, Germany), prabotulinumtoxinA (Jeuveau®; Evolus Inc, Santa Barbara, Calif), CS-BOT (Chiba Serum Institute; Chiba, Japan), and Chinese BTX-A (Prosigne ®; Lanzhou Biological Products Institute, China) differ in potency. [6]
-
BoNT-A is prepared by laboratory fermentation of C botulinum cultures. Crude botulinum toxin is a protein with a molecular weight of about 190,000 Daltons. After purification, the toxin is diluted with human serum albumin, bottled in vials, lyophilized (freeze-dried), and sealed.
-
Each freeze-dried vial containing 100 units (U) of BoNT-A is reconstituted with preservative-free normal saline (1-5 mL) just before use. The manufacturer recommends that the toxin be used within 4 hours of reconstitution.
-
The potency of BoNT-A is measured in mouse units (MU). One MU of BoNT-A is equivalent to the amount of toxin that kills 50% of a group of 20 g Swiss-Webster mice within 3 days of intraperitoneal injection (LD50).
-
According to one report, 1 nanogram of toxin contains approximately 20 U of BOTOX® (ie, 1 U of BOTOX® is equal to approximately 0.05 nanogram of the toxin).
-
According to another report comparing the 3 different preparations of BoNT-A, 1 nanogram of Dysport contains approximately 40 MU, whereas 1 nanogram of the BOTOX® contains approximately 4 MU, and 1 nanogram of CS-BOT contains approximately 15.2 MU.
-
Median paralysis unit (MPU) is thought to be a more pharmacologically relevant unit of biologic activity. Comparison of the potency ratio based on the MPU values for Dysport and BOTOX® revealed a 2.44-fold difference in potency between these formulations. [7]
-
LD50 of BoNT-A for a 70-kg adult male has been calculated to be 2500-3000 U (35-40 U/kg).
-
Minimum lethal dose of BoNT-B in monkeys is 2400 U/kg.
-
Clinically, 1 U of BoNT-A (BOTOX®) is approximately equivalent to 3 U of Dysport®. [8]
-
DaxibotulinumtoxinA (Daxxify®) is the first peptide-formulated, long-acting botulinum toxin; it has a median duration of effect of 6 months. [9]
-
An animal study that found that Xeomin® contains the highest specific neurotoxin activity, followed by Dysport®, with BOTOX® having the lowest specific activity. [12]
-
Standardization efforts are underway using measurements of the toxin's pharmacologically relevant actions (eg, median paralysis unit).
-
BOTOX® vials contain sodium chloride (0.9 mg) and human albumin (0.5 mg), and the protein load is 5 ng/100 units; Prosigne® vials contain porcine gelatin (5 mg), dextran (25 mg), and sucrose (25 mg), and the protein load is 4-5 ng/100 units of BoNT-A. [13] BOTOX® is thought to be about 1.5 times more potent than Prosigne®.
-
BoNT-B is marketed in the United States as RimaBotulinumB (MyoBloc®). This preparation is a ready-to-use solution that does not require reconstitution; it is available in 3 vial sizes (ie, 2500 U, 5000 U, and 10,000 U) and is stable for up to 21 months in refrigerator storage.
Therapeutic Uses
Therapeutic uses of botulinum toxin injection [14] [15]
-
Focal dystonias - Involuntary, sustained, or spasmodic patterned muscle activity
-
Chronic pain and disorders of localized muscle spasms
-
Sweating, salivary, and allergy disorders
Botulinum Toxin Use in Dystonia
Use of BoNT-A in different types of focal dystonias has been well studied and has proven to be very effective. Botulinum toxin injection is the treatment of choice for cervical dystonia (spasmodic torticollis). [16, 17, 89] . A Cochrane review concluded that a single injection of BoNT-B was effective and safe for treating cervical dystonia. [90] This injection benefits the highest percentage of patients in the shortest time and has been proven effective in many double-blind, placebo-controlled trials.
BoNT has fewer side effects than do other pharmacologic treatments. The efficacy and safety of BoNT injections for the treatment of certain movement disorders, including blepharospasm, hemifacial spasm, oromandibular dystonia, cervical dystonia, focal limb dystonias, laryngeal dystonia, tics, and essential tremor is ongoing. [91]
In a double-blind, placebo-controlled trial by Greene and colleagues, 55 patients who previously had failed to find relief in 2 trials of medication received either BoNT or placebo in a double-blinded fashion and were tracked for 12 weeks. [92] Four weeks of open phase then followed when all patients received BoNT. By 6 weeks, 61% of patients showed improvement in head posture, and 39.5% reported reduction of pain. Both measures significantly improved (P< .05) compared to controls. During the open phase, patients who previously received placebo exhibited a similar response. Overall, 74% of patients improved by the end of the study.
A study by Brans and colleagues showed that in 64 patients with cervical dystonia, 84% reported long-term benefits in terms of impairment, disability, handicap, and quality of life (QOL). [93] Mezaki et all described their experience with a Japanese type A toxin for the treatment of cervical and axial dystonias. [94] Injections were given repeatedly at intervals of 28-30 days to carefully chosen muscles with increased activities, with a maximum dose per session of 300 units. The maximum improvements in subjective and objective ratings were obtained only after repeated injections.
Procedure
Treatment dosages of BoNT-A in the United States have been reported to range from 100-300 U per patient. In a double-blind, placebo-controlled study, Poewe and colleagues demonstrated that magnitude and duration of improvement were greatest after injections of 1000 U of Dysport, but the injections caused significantly more adverse effects. [95] The researchers recommended a lower starting dose of 500 U of Dysport (1 U of BoNT-A = 3 U of Dysport). One hundred U of toxin per mL of preservative-free normal saline are commonly used.
Injections are performed with a Teflon-coated, 24-gauge needle connected to an electromyographic (EMG) machine. Those muscles with highest clinical and EMG activity are injected. Usually, 2-4 separate muscles are injected in 1 session and, in larger muscles, 2-4 sites per muscle are injected.
No general consensus exists among users of BoNT regarding the need for EMG guidance while injecting the compound for cervical dystonia. EMG guidance, however, is helpful, particularly in obese patients whose neck muscles cannot adequately be palpated.
Identifying the specific muscles involved in cervical dystonia prior to the injection is important. Those most commonly injected are the sternocleidomastoid, trapezius, splenius capitis, and levator scapulae muscles. An EMG study of 100 patients found that 2 or 3 muscles commonly are abnormal. Eighty-nine percent of patients with rotating torticollis had involvement of the ipsilateral splenius capitis and contralateral sternocleidomastoid with or without the additional involvement of the contralateral splenius capitis. Patients with laterocollis had ipsilateral sternocleidomastoid, splenius capitis, and trapezius involvement, while retrocollis was produced by bilateral splenius capitis activity.
Beneficial effect from toxin injection usually is apparent in 7-10 days. Maximum response from the toxin is reached in approximately 4-6 weeks and lasts for an average of 12 weeks. Injections usually are repeated every 3-4 months.
Complications
Neck weakness, dysphagia, and local pain at the injection site are the most commonly reported side effects. Other adverse effects (eg, local hematoma, generalized fatigue, lethargy, dizziness, dry mouth, dysphonia, flulike syndrome, pain in neighboring muscles) also have been reported.
Most studies have reported side effects in 20-30% of patients per treatment cycle. The incidence of adverse effects varies based on the dosage used (ie, the higher the dose, the more frequent the adverse effects); however, Jankovic and Schwartz reported that incidence of complications was not related to the total dose of BoNT used. [96] Women and patients who received injections into the sternocleidomastoid muscles had significantly higher rates of complications.
Dysphagia has been the most prevalent significant complication and most probably is related to diffusion of the toxin into nearby pharyngeal muscles. In the study by Comella and colleagues, 33% of patients receiving their first dose of botulinum toxin experienced dysphagia. [97] This complication most commonly occurs with injections of the sternocleidomastoid and can be reduced significantly when the dose of toxin administered is 100 U or less.
Botulinum Toxin Use in Spasticity
Spasticity is defined as a velocity-dependent increase in muscle tone. Intramuscular injections of BoNT have been studied and found to be useful in the treatment of spasticity in multiple sclerosis (MS), cerebral palsy (CP), stroke, traumatic brain injury (TBI), and spinal cord injury (SCI). Different studies have shown the effectiveness of BoNT-A injection in the management of spasticity. [25]
Table 2. Studies of Botulinum Toxin in the Treatment of Spasticity in Different Disorders (Open Table in a new window)
Clinical Diagnosis |
Author |
Study Design |
Multiple Sclerosis |
Benecke Borg-Stein et al [98] Snow et al [99] Hyman et al [100] |
Open-label Open-label Double-blind, placebo-controlled, randomized, crossover Double-blind, placebo-controlled, randomized, dose-ranging |
Spinal Cord Injury |
Bohlega et al Takenaga et al |
Open-label Open-label |
Cerebral Palsy |
Koman et al [101] Koman et al [102] Cosgrove et al [103] Chutorian and Root Chutorian, Root, and the BTA study group Corry et al [104] Fehlings et al [105] Wissel et al [106] Baker et al [107] Edwards et al [108] |
Open-label Double-blind, placebo-controlled Open-label Open-label Double-blind, placebo-controlled, randomized Double-blind, placebo-controlled Single-blind, randomized, controlled Double-blind, randomized, placebo-controlled Double-blind, randomized, placebo-controlled Double-blind, randomized, placebo-controlled |
Stroke |
Das and Park Memin et al Grazko et al Dengler et al Jabbari et al Simpson et al Bhaktha et al [109] Smith et al [110] Childers et al [111] Pittock et al [112] Brashear et al [113] Bakheit et al [114] |
Open-label Open-label Double-blind, placebo-controlled, crossover Open-label Double-blind, placebo-controlled, crossover Double-blind, placebo-controlled Double-blind, placebo-controlled, randomized Double-blind, placebo-controlled, randomized Double-blind, placebo-controlled, randomized Double-blind, placebo-controlled, randomized Double-blind, placebo-controlled, randomized |
Traumatic Brain Injury |
Yablon et al [115] Pavesi et al [116] |
Open-label Open-label |
Pain Management
Use of BoNT-A in the management of different pain disorders is being studied. [117] At this time, indications for the use of BoNT in managing muscle pain disorders still are controversial. The exact mechanism of action behind BoNT's analgesic effect is not known; however, a study by Purkiss and colleagues showed that BoNT inhibits calcium-dependent release of substance P in embryonic dorsal root ganglia. [118] Hence, BoNT may, by blocking the release of substance P, produce an analgesic effect through peripheral inhibition of C and A delta fibers. Based on the research with animal models, BoNT-A in peripheral nociceptive neurons plays a direct role in its peripheral analgesic effect and an indirect role in its central analgesic effect because of retrograde transport. [119]
In a double-blind, randomized, placebo-controlled study, Foster and colleagues showed the efficacy of 200 U of BoNT-A injection, using 40 U per site at 5 lumbar paravertebral levels on the side of maximum discomfort, in chronic low back pain patients. [120]
A Cochrane review regarding the use of BoNT-A injection for chronic low back pain has concluded evidence that BoNT injections improved pain, function, or both better than saline injections was limited, as was evidence this was better than acupuncture or steroid injections. [121] They recommend further high quality randomized controlled studies.
BoNT-A injection has also been studied for chronic neck pain, cervicogenic headache, and whiplash-associated neck pain; however, a Cochrane review and systematic review and meta-analysis by Langevin et al concluded that current evidence fails to confirm either a clinically important or a statistically significant benefit of BoNT-A injection for whiplash-associated neck pain and chronic neck pain associated with or without cervicogenic headache. [122, 123]
BoNT-A has been studied to treat different neuropathic pain disorders such as postherpetic neuralgia, [124] trigeminal neuralgia, [125, 126] and diabetic peripheral neuropathic pain, [127] and has shown to be effective in managing pain in these conditions.
Different studies on the use of BoNT in the management of different pain disorders are listed in Table 3.
Table 3. Studies on the Use of Botulinum Toxin in Pain Management (Open Table in a new window)
Author(s) (Year) |
Clinical Condition |
Study Type |
N |
Results |
Zwart et al (1994) [128] |
Tension headache |
Open-label |
6 |
Unilateral temporal injection not effective |
Sherman et al (1995) [129] |
Chronic pancreatitis |
Open-label |
7 |
Not effective |
Paulson et al (1996) [130] |
Fibromyalgia |
Randomized, controlled |
5 |
Not effective |
Wheeler et al (1998) [131] |
Myofascial pain [132] |
Randomized, double-blind, controlled |
33 |
No significant difference, second injection effective? |
Wheeler (1998) [133] |
Tension headache |
Open-label |
4 |
Effective in 4 patients |
Schulte-Mattler et al (1999) [134] |
Tension headache |
Open-label |
9 |
Effective in 8 of 9 patients |
Freund et al (1999) [135] |
Temporomandibular disorders |
Open-label |
15 |
Effective |
Freund et al (2000) [136] |
Temporomandibular disorders |
Open-label |
46 |
Effective |
Silberstein et al (2000) [137] |
Migraine headache |
Double-blind, vehicle-controlled |
123 |
Effective prophylaxis |
Rollnik et al (2000) [138] |
Tension headache |
Double-blind, placebo-controlled |
21 |
Not effective |
Freund et al (2000) [139] |
Cervicogenic Headache |
Randomized, double-blind, placebo-controlled |
26 |
Effective |
Freund et al (2000) [140] |
Whiplash associated with neck pain |
Randomized, double-blind, placebo-controlled |
26 |
Effective |
Barwood et al (2000) [141] |
Severe postoperative pain and spasm in cerebral palsy |
Randomized, double-blind, placebo-controlled |
16 |
Effective prophylaxis |
Porta (2000) [142] |
Chronic myofascial pain syndrome |
Randomized, controlled, comparative |
40 |
BOTOX® better than methylprednisolone |
For more information, see Medscape Reference article Botulinum Toxin in Pain Management.
Adverse Events
Adverse events due to therapeutic and cosmetic injection of BoNT reported to the FDA include respiratory problems, dysphagia, seizure, flulike syndrome, facial and other muscle weakness, ptosis, and skin and injection site reactions. [143] Of the 406 reports related to therapeutic use, 217 met the FDA's definition of serious, with 28 deaths and 17 seizures reported. Clinical characteristics submitted to the FDA for therapeutic cases differed from those of cosmetic BoNT cases, which were usually less serious. Most of the adverse effects linked to local tissue diffusion of BoNT. Careful attention to drug dose, dilution, handling, storage, and site of injection are required for optimal treatment outcome and to minimize adverse effects.
Questions & Answers
Overview
What is botulinum toxin (BoNT)?
What are the FDA approved indications for botulinum toxin (BoNT)?
What is the molecular structure and proteolytic activity of botulinum toxin (BoNT)?
What was the evolution of therapeutic botulinum toxin (BoNT)?
What is the mechanism of action in botulinum toxin (BoNT)?
How does the potency vary among different commercial preparations of botulinum toxin (BoNT)?
Which focal dystonias are treated with botulinum toxin injection?
In which conditions is spasticity treated with botulinum toxin (BoNT) injection?
Which smooth muscle hyperactive disorders are treated with botulinum toxin (BoNT) injections?
Which cosmetic procedures use botulinum toxin (BoNT) injections?
Which sweating, salivary, and allergy disorders are treated with botulinum toxin (BoNT) injections?
What is the efficacy of botulinum toxin (BoNT) in the treatment of focal dystonias?
How is botulinum toxin (BoNT) administered in the treatment of focal dystonias?
What are the possible complications of botulinum toxin (BoNT) in the treatment of focal dystonias?
What is the efficacy of botulinum toxin (BoNT) injections for the treatment of spasticity?
What is the role of botulinum toxin (BoNT) in pain management?
-
Botulinum toxin structure (schematic diagram).
-
Proteolytic activity is located at the N-terminal end of the light chain of botulinum toxin type A.
Tables
Type |
Target |
Discoverer |
Year |
A |
SNAP-25 |
Landman |
1904 |
B |
VAMP |
Ermengem |
1897 |
C1 |
Syntaxin |
Bengston and Seldon |
1922 |
D |
VAMP |
Robinson |
1929 |
E |
SNAP-25 |
Gunnison |
1936 |
F |
VAMP |
Moller and Scheibel |
1960 |
G |
VAMP |
Gimenez and Ciccarelli |
1970 |
Clinical Diagnosis |
Author |
Study Design |
Multiple Sclerosis |
Benecke Borg-Stein et al [98] Snow et al [99] Hyman et al [100] |
Open-label Open-label Double-blind, placebo-controlled, randomized, crossover Double-blind, placebo-controlled, randomized, dose-ranging |
Spinal Cord Injury |
Bohlega et al Takenaga et al |
Open-label Open-label |
Cerebral Palsy |
Koman et al [101] Koman et al [102] Cosgrove et al [103] Chutorian and Root Chutorian, Root, and the BTA study group Corry et al [104] Fehlings et al [105] Wissel et al [106] Baker et al [107] Edwards et al [108] |
Open-label Double-blind, placebo-controlled Open-label Open-label Double-blind, placebo-controlled, randomized Double-blind, placebo-controlled Single-blind, randomized, controlled Double-blind, randomized, placebo-controlled Double-blind, randomized, placebo-controlled Double-blind, randomized, placebo-controlled |
Stroke |
Das and Park Memin et al Grazko et al Dengler et al Jabbari et al Simpson et al Bhaktha et al [109] Smith et al [110] Childers et al [111] Pittock et al [112] Brashear et al [113] Bakheit et al [114] |
Open-label Open-label Double-blind, placebo-controlled, crossover Open-label Double-blind, placebo-controlled, crossover Double-blind, placebo-controlled Double-blind, placebo-controlled, randomized Double-blind, placebo-controlled, randomized Double-blind, placebo-controlled, randomized Double-blind, placebo-controlled, randomized Double-blind, placebo-controlled, randomized |
Traumatic Brain Injury |
Yablon et al [115] Pavesi et al [116] |
Open-label Open-label |
Author(s) (Year) |
Clinical Condition |
Study Type |
N |
Results |
Zwart et al (1994) [128] |
Tension headache |
Open-label |
6 |
Unilateral temporal injection not effective |
Sherman et al (1995) [129] |
Chronic pancreatitis |
Open-label |
7 |
Not effective |
Paulson et al (1996) [130] |
Fibromyalgia |
Randomized, controlled |
5 |
Not effective |
Wheeler et al (1998) [131] |
Myofascial pain [132] |
Randomized, double-blind, controlled |
33 |
No significant difference, second injection effective? |
Wheeler (1998) [133] |
Tension headache |
Open-label |
4 |
Effective in 4 patients |
Schulte-Mattler et al (1999) [134] |
Tension headache |
Open-label |
9 |
Effective in 8 of 9 patients |
Freund et al (1999) [135] |
Temporomandibular disorders |
Open-label |
15 |
Effective |
Freund et al (2000) [136] |
Temporomandibular disorders |
Open-label |
46 |
Effective |
Silberstein et al (2000) [137] |
Migraine headache |
Double-blind, vehicle-controlled |
123 |
Effective prophylaxis |
Rollnik et al (2000) [138] |
Tension headache |
Double-blind, placebo-controlled |
21 |
Not effective |
Freund et al (2000) [139] |
Cervicogenic Headache |
Randomized, double-blind, placebo-controlled |
26 |
Effective |
Freund et al (2000) [140] |
Whiplash associated with neck pain |
Randomized, double-blind, placebo-controlled |
26 |
Effective |
Barwood et al (2000) [141] |
Severe postoperative pain and spasm in cerebral palsy |
Randomized, double-blind, placebo-controlled |
16 |
Effective prophylaxis |
Porta (2000) [142] |
Chronic myofascial pain syndrome |
Randomized, controlled, comparative |
40 |
BOTOX® better than methylprednisolone |






