Practice Essentials
Scheuermann, or Scheuermann's, disease (juvenile kyphosis) is a deformity in the thoracic or thoracolumbar spine in which pediatric patients have an increased kyphosis along with backache and localized changes in the vertebral bodies. [1, 2] See the image below.
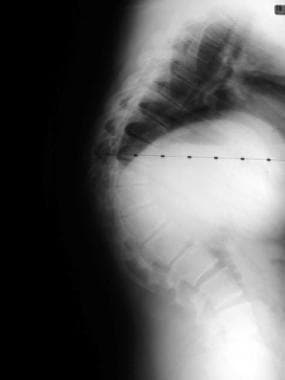 Preoperative lateral of a patient with an 85º thoracic deformity secondary to Scheuermann's disease.
Preoperative lateral of a patient with an 85º thoracic deformity secondary to Scheuermann's disease.
Scheuermann's disease refers to osteochondrosis of the secondary ossification centers of the vertebral bodies. The lower dorsal and upper lumbar vertebrae are involved initially. The process may be limited to several bodies or may involve the entire dorsal and lumbar spine.
Scheuermann's disease probably is heterogeneous (ie, not a single entity but a group of conditions sharing similar features).
Signs and symptoms of Scheuermann’s disease
Signs and symptoms of Scheuermann’s disease include the following:
-
Patients with upper thoracic Scheuermann's disease present with a kyphotic deformity best demonstrated in the forward flexed position
-
Decreased flexibility of the spine is noted, indicating the structural nature of the kyphotic deformity, in contrast with patients with flexible postural kyphosis
-
Patients may have tenderness to palpation above and below the apex of the kyphosis
-
A high association exists between scoliosis and Scheuermann's disease; patients also may have a hyperlordosis in the lumbar spine
-
Lower thoracic kyphosis is localized at the thoracolumbar junction; in general, any kyphotic deformity present at this level must be considered abnormal
-
Hamstring tightness may be present in these patients
-
Neurologic deficits can occur but are extremely rare
Diagnosis and management of Scheuermann's disease
Lateral radiography of the spine demonstrates diagnostic changes in Scheuermann's disease. [3, 4] Sorenson suggested the following radiologic criteria for the diagnosis of the condition:
-
Hyperkyphosis greater than 40°
-
Irregular upper and lower vertebral endplates with loss of disk space height
-
Wedging of 5° or more in three consecutive vertebrae
The treatment of Scheuermann's disease is controversial. [5, 6] Some authors think that the natural history of thoracic Scheuermann's disease is benign and that therefore the condition needs no treatment. Whether orthotics or surgical treatments prevent any of the consequences that may occur is uncertain.
When the kyphosis is relatively severe, recommendations include casting, a spinal brace, or rest and recumbency on a rigid bed. Orthotic management of Scheuermann's disease usually requires 12-24 months of treatment.
Surgery rarely is indicated in patients with Scheuermann's disease. Probably the two most common indications for surgery are spinal pain and unacceptable cosmetic appearance. These criteria are subjective, so it is wise to be cautious in counseling these patients. [7]
In patients with curves greater than 75° and with pain that is unresponsive to nonoperative measures, consider spinal fusion. Spinal fusion consists of an anterior release and fusion, as well as a posterior instrumentation and fusion performed under the same anesthesia on the same day.
Cord decompression is indicated for the rare patients who have neurologic deficits secondary to epidural cysts or increased kyphotic angulation.
Pathophysiology
Scheuermann's disease refers to osteochondrosis of the secondary ossification centers of the vertebral bodies. The lower dorsal and upper lumbar vertebrae are involved initially. The process may be limited to several bodies or may involve the entire dorsal and lumbar spine.
Scheuermann's disease probably is heterogeneous (ie, not a single entity but a group of conditions sharing similar features). The etiology and pathogenesis are a matter of debate. Many theories have been advanced, including mechanical, metabolic, and endocrinologic causes.
A definite hereditary component is involved in the development of the condition, but the mode of inheritance has been debated. [8] Reports of identical radiologic changes in monozygotic twins and transmission over 3 generations suggested underlying heritability. In study by McKenzie and Sillence, 12 probands were referred, and upon radiologic examination of their parents and siblings, 7 were shown to have familial Scheuermann's disease with an autosomal dominant pattern of inheritance. [9] Of the remaining 5 probands, 4 had chromosomal anomalies.
Patients with Scheuermann's disease generally are affected at age 13-16 years, are taller [10] than comparably aged peers, and have advanced skeletal versus chronologic age. Some affected children have disproportionate limb lengths.
A Greek research report, however, found that although, in the study, children with Scheuermann's disease tended to be taller and weigh more than did other children, there seemed to be no correlation in children with the disease between these 2 factors and the magnitude and morphology of the main kyphotic curve. [10] The authors suggested that hormonal disturbances may be impacting the development of Scheuermann's disease and also causing, as a secondary result, height and weight increases.
A study by Hershkovich et al, however, suggested that height and body mass index (BMI) are associated with the risk and severity of spinal deformities in adolescents. The study, which involved the medical records of 829,791 males and females aged 17 years, including 103,249 who had been diagnosed with some degree of kyphosis or scoliosis, found a significantly higher rate of spinal deformities, and a greater likelihood of such deformities being severe, in underweight males and females. Greater height was also found to be associated with increased risk and greater severity of spinal deformities in males and females. [11]
In a Finnish study, left-handedness was found to be a powerful determinant of hyperkyphosis in school children before puberty. [12] An increased incidence of spondylolysis and spondylolisthesis also was reported in patients with Scheuermann's disease, and scoliosis in the region of kyphosis is reported in 20-30% of patients as well. [13]
According to some authors, the presence of an adjacent area of lordoscoliosis below the region of hyperkyphosis testifies to the common nature of the pathogenesis of idiopathic scoliosis and Scheuermann's disease. Scheuermann's disease may be associated with an epidural cyst with an ensuing neurologic deficit.
A retrospective study by Tyrakowski et al found no significant difference between skeletally mature and skeletally immature patients with Scheuermann’s disease with regard to radiographic sagittal spinopelvic parameters, including sagittal vertical axis, thoracic kyphosis, thoracolumbar kyphosis, lumbar lordosis, pelvic incidence, pelvic tilt, and sacral slope. However, both groups (33 patients each) had a significantly lower pelvic incidence and sacral slope than did children, adolescents, and adults without Scheuermann’s disease, causing the investigators to question the use of pelvic incidence in predicting the desired lumbar lordosis in Scheuermann’s disease cases. [14]
A study by Peleg et al suggested that a greater horizontal orientation of the sacrum may lead to a change in spinal biomechanics that in turn contributes significantly to the development of Scheuermann’s disease. The study involved the evaluation of the sacral anatomical orientation in 183 persons with Scheuermann’s disease and 185 controls. [15]
Epidemiology
Frequency
United States
The prevalence rate of Scheuermann's disease is thought to be 0.4-8%.
International
A study by Armbrecht et al using found the prevalence of Scheuermann’s disease in Europe to be 8% in persons aged 50 years and above, with no difference between males and females. The sample, consisting of more than 10,000 individuals, came from 27 centers across Europe that participated in the European Vertebral Osteoporosis Study. [16]
Mortality/Morbidity
Many authors believe that there are few adverse long-term sequelae of Scheuermann's disease, despite a paucity of available natural history data. Lowe suggests that if residual kyphosis remains less than 60º at skeletal maturity, the patient has an excellent prognosis for minimal problems in adult life.
Pain may be present but generally ceases when growth is complete. Minimal spinal malalignment may persist when the disorder becomes quiescent. Early development of marginal osteophytes may occur. Acute myelopathy secondary to cord compression at the apex of the thoracic kyphosis has been reported.
Using the exercise tolerance test, a prospective, comparative study by Lorente et al found that adolescent Scheuermann’s disease patients with kyphosis of over 75° displayed significant respiratory inefficiency, with ventilation capacity and maximum oxygen uptake being lower than in healthy controls. [17]
A study by Liu et al suggested that a link exists between Scheuermann’s disease and thoracolumbar disk herniation (disk herniation between T10/11 and L1/2). The investigators found that the radiographic signs of Scheuermann’s disease, as well as the diagnosis of Scheuermann’s disease itself, were significantly more prevalent in the 63 patients in the study with symptomatic thoracolumbar disk herniation than they were in a group of 57 patients who underwent surgery for lower lumbar disk herniation. Moreover, in the patients with thoracolumbar disk herniation, the herniation was significantly more prevalent at segments displaying the radiographic signs of Scheuermann’s disease than at segments that did not. [18]
A study by Garrido et al of patients with untreated kyphosis in Scheuermann’s disease found, at mean 27-year follow-up, that a correlation existed between increases in the sagittal vertical axis (SVA) and declining health-related quality of life. Greater SVA was associated with worse function, pain, disability, and mental health scores, as measured using the Scoliosis Research Society-22 (SRS-22) questionnaire, the 36-item Short-Form Health Survey (SF-36), and the Oswestry Disability Index (ODI). Kyphosis in the patients, which had a mean value of 66° at skeletal maturity, had increased to 78° at follow-up. [19]
Sex
Scheuermann's disease affects boys more frequently than it does girls.
Age
Scheuermann's disease affects children aged 13-16 years, and the diagnosis is rarely made in patients younger than 10 years.
-
Preoperative lateral of a patient with an 85º thoracic deformity secondary to Scheuermann's disease.
-
Postoperative lateral demonstrating a 2-rod leverage technique after an anterior release allowing reduction of the deformity to 47º.
