Background
In planning for nasal reconstruction requiring an implant, careful decisions need to be made regarding the types of materials to substitute for support. Final soft-tissue coverage of the planned reconstruction is of paramount importance in the preparation.
The nose is critically involved in appearance, both to oneself and to others, and it is significantly involved in the perception of beauty both publicly and privately. Because of its central location on the face, plane of projection, and relatively weak chondrocutaneous support structure, the nose is susceptible to injury, and deformities are readily apparent.
Whatever the circumstances that lead to the nasal deformity, the complex tasks of assessing the patient's nasal anatomy, pathologic defect, aesthetic qualities, baseline perception, planning the reconstruction, and preparing the patient for the possible positive and negative outcomes can be daunting.
History of the Procedure
In northern India, during the 6th century BC, Susruta focused on soft-tissue augmentation for amputation injuries and nasal reconstruction. [1] See the image below.
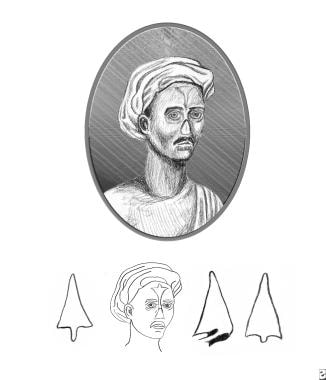 Reproduction of plate from Susruta showing style of nasal reconstruction. Note that support for the nasal bridge is absent. The intrinsic rigidity of the dermis was relied upon for structural support. (Susruta, An English Translation of the Susrita Samhita, based on original Sanskrit text. Edited and published by Kaniraj Kunjabal Blushagratna. Calcutta: Bose, 1916).
Reproduction of plate from Susruta showing style of nasal reconstruction. Note that support for the nasal bridge is absent. The intrinsic rigidity of the dermis was relied upon for structural support. (Susruta, An English Translation of the Susrita Samhita, based on original Sanskrit text. Edited and published by Kaniraj Kunjabal Blushagratna. Calcutta: Bose, 1916).
In the 16th and 17th centuries, Tagliocozzi used a tubed pedicle flap and Carpue, an Englishman, reinstituted the forehead flap. [2, 3] See the images below.
 Reproduction of plate from Tagliocozzi as depicted by Gnudi and Webster. Skin of the inner upper arm has minimal intrinsic rigidity and always requires internal structural support.
Reproduction of plate from Tagliocozzi as depicted by Gnudi and Webster. Skin of the inner upper arm has minimal intrinsic rigidity and always requires internal structural support.

Various nonautogenous materials have been employed over the centuries to improve reconstruction of the nose by providing bridge support. Early attempts at finding the ideal or most suitable nasal implant for bridge construction included trials of materials such as paraffin, gold, silver, aluminum, ivory, cork, stones from the Black Sea, polyethylene, rubber, silicone, lead, and a toothbrush handle.
Currently, general categories of available materials include autografts, homografts, and allografts. This article covers the variety of materials commonly employed. The pros and cons of various materials are detailed and illustrated.
Problem
The choice of nasal implants to be placed in reconstructive surgery of the nose is a difficult but important component in the patient's care. The degree of loss noted in tip support, bridge contour, or nasal valve collapse may mandate implant use in nasal reconstruction. Each of the various materials has benefits and pitfalls, which must be balanced against the surgeon's familiarity with each material. Because of the nose's central location, minor defects of reconstruction may be particularly noticeable to any casual observer but may play a much larger role psychologically in the patient's perception of self. Based on the authors' review of the literature and clinical experience, autogenous cartilage and/or bone are recommended as the primary choices for nasal implants.
Indications
Although the major underlying cause of nasal reconstruction is trauma, a number of pathologic entities traditionally have required surgical nasal reconstruction (eg, congenital malformations, malignant destruction, septal perforations, granulomatous disease, congenital syphilis, leishmaniasis, leprosy). Whatever the cause of the defect, nasal reconstruction with or without various implant materials allows restoration of function along with restoration of an aesthetically critical component of the face.
Relevant Anatomy
A prerequisite to nasal reconstruction is familiarity with nasal anatomy and proportions. The nose is generally divided by anatomic units into thirds. The upper third of the nose, or bony vault, is represented by the paired nasal bones that overlie the nasal spine of the frontal bone. The cartilaginous vault represents the lower two thirds of the nose, with the middle third being the region of the upper lateral cartilages, and the lower third involving the nasal tip, septum, and lower lateral (alar) cartilages. The general function of the nose is to warm and humidify incoming air. To achieve both form and function, the nasal vestibule should comprise approximately one half to two thirds of the nasal lobule as viewed from the basal projection. Attention should be dedicated to reconstructing the columella, tip, and ala to form an adequate nostril internally while incorporating aesthetics externally.
Contraindications
Ongoing infection or conditions requiring further therapy (eg, serial débridements) are examples of contraindications to reconstruction. Address patient stabilization and optimization, including nutritional status when possible, prior to surgical intervention. Therapies such as radiation or chemotherapy should be completed prior to reconstruction.
-
Reproduction of plate from Susruta showing style of nasal reconstruction. Note that support for the nasal bridge is absent. The intrinsic rigidity of the dermis was relied upon for structural support. (Susruta, An English Translation of the Susrita Samhita, based on original Sanskrit text. Edited and published by Kaniraj Kunjabal Blushagratna. Calcutta: Bose, 1916).
-
Reproduction of plate from Tagliocozzi as depicted by Gnudi and Webster. Skin of the inner upper arm has minimal intrinsic rigidity and always requires internal structural support.
-
Reproduction of plate from Carpue manuscript. Note refinements in flap design.
-
Rib cartilage graft and Proplast bridge graft. A 46-year-old woman with a congenital deficiency of the nasal bridge underwent a series of reconstruction attempts using septal and conchal cartilage grafts. Front view.
-
Rib cartilage graft and Proplast bridge graft. A 46-year-old woman with a congenital deficiency of the nasal bridge underwent a series of reconstruction attempts using septal and conchal cartilage grafts. Right side view.
-
Rib cartilage graft and Proplast bridge graft. A 46-year-old woman with a congenital deficiency of the nasal bridge underwent a series of reconstruction attempts using septal and conchal cartilage grafts. Harvesting of the rib graft.
-
Rib cartilage graft and Proplast bridge graft. A 46-year-old woman with a congenital deficiency of the nasal bridge underwent a series of reconstruction attempts using septal and conchal cartilage grafts. Postoperative right side view.
-
Rib cartilage graft and Proplast bridge graft. A 46-year-old woman with a congenital deficiency of the nasal bridge underwent a series of reconstruction attempts using septal and conchal cartilage grafts. Removal of deformed rib cartilage 6 years after reconstruction.
-
Rib cartilage graft and Proplast bridge graft. A 46-year-old woman with a congenital deficiency of the nasal bridge underwent a series of reconstruction attempts using septal and conchal cartilage grafts. Tailored carved Proplast bridge graft to replace deformed rib cartilage.
-
Rib cartilage graft and Proplast bridge graft. A 46-year-old woman with a congenital deficiency of the nasal bridge underwent a series of reconstruction attempts using septal and conchal cartilage grafts. Postoperative right side view 4 years after Proplast bridge graft.
-
Calvarial bone graft and auricular conchal cartilage. A 61-year-old man required a subtotal nasal reconstruction of a septal squamous cell carcinoma and left cervical radical lymphadenectomy. Reconstruction began with a forehead flap of tissue expanded skin. Right lateral view.
-
Calvarial bone graft and auricular conchal cartilage. A 61-year-old man required a subtotal nasal reconstruction of a septal squamous cell carcinoma and left cervical radical lymphadenectomy. Reconstruction began with a forehead flap of tissue expanded skin. Calvarial bone graft harvest site.
-
Calvarial bone graft and auricular conchal cartilage. A 61-year-old man required a subtotal nasal reconstruction of a septal squamous cell carcinoma and left cervical radical lymphadenectomy. Reconstruction began with a forehead flap of tissue expanded skin. Sculpted calvarial bone graft.
-
Calvarial bone graft and auricular conchal cartilage. A 61-year-old man required a subtotal nasal reconstruction of a septal squamous cell carcinoma and left cervical radical lymphadenectomy. Reconstruction began with a forehead flap of tissue expanded skin. Calvarial bone graft in place and anchored to glabellar area of frontal bone.
-
Calvarial bone graft and auricular conchal cartilage. Harvest of auricular conchal cartilage graft from anterior approach. A 61-year-old man required a subtotal nasal reconstruction of a septal squamous cell carcinoma and left cervical radical lymphadenectomy. Reconstruction began with a forehead flap of tissue expanded skin.
-
Calvarial bone graft and auricular conchal cartilage. A 61-year-old man required a subtotal nasal reconstruction of a septal squamous cell carcinoma and left cervical radical lymphadenectomy. Reconstruction began with a forehead flap of tissue expanded skin. Sculpted conchal cartilage graft on nasal tip.
-
Calvarial bone graft and auricular conchal cartilage. Postoperative frontal view at 1 year. A 61-year-old man required a subtotal nasal reconstruction of a septal squamous cell carcinoma and left cervical radical lymphadenectomy. Reconstruction began with a forehead flap of tissue expanded skin.
-
Silastic graft and rib bone graft. Preoperative frontal view. A 37-year-old woman presented 10 years following reconstruction of an unreduced naso-orbitoethmoid fracture with silastic H-shaped graft.
-
Silastic graft and rib bone graft. Preoperative oblique view demonstrating the distortion of the silastic graft secondary to scar tissue. A 37-year-old woman presented 10 years following reconstruction of an unreduced naso-orbitoethmoid fracture with silastic H-shaped graft.
-
Silastic graft and rib bone graft. Harvest of the rib bone graft. A 37-year-old woman presented 10 years following reconstruction of an unreduced naso-orbitoethmoid fracture with silastic H-shaped graft.
-
Silastic graft and rib bone graft. A 37-year-old woman presented 10 years following reconstruction of an unreduced naso-orbitoethmoid fracture with silastic H-shaped graft. Fabrication of the osseous H-shaped graft. Removed silastic graft serves as a pattern.
-
Silastic graft and rib bone graft. A 37-year-old woman presented 10 years following reconstruction of an unreduced naso-orbito-ethmoid fracture with silastic H-shaped graft. Postoperative frontal view at 10.5 years postreconstruction.
-
Silastic graft and rib bone graft. A 37-year-old woman presented 10 years following reconstruction of an unreduced naso-orbitoethmoid fracture with silastic H-shaped graft. Postoperative side view at 10.5 years postreconstruction.
-
Fascial grafts. A 55-year-old woman sought improvement of radix and upper nasal bridge following an aesthetic rhinoplasty. Preoperative side view. Note the shallow glabella.
-
Fascial grafts. A 55-year-old woman sought improvement of radix and upper nasal bridge following an aesthetic rhinoplasty. Temporal fascial graft prior to placement.
-
Fascial grafts. A 55-year-old woman sought improvement of radix and upper nasal bridge following an aesthetic rhinoplasty. Right temporal donor site closure.
-
Fascial grafts. A 55-year-old woman sought improvement of radix and upper nasal bridge following an aesthetic rhinoplasty. Postoperative side view at 3 months.
-
Proplast nasal grafts. A 20-year-old man with a posttraumatic nasal deformity with septal collapse. Preoperative side view.
-
Proplast nasal grafts. A 20-year-old man with a posttraumatic nasal deformity with septal collapse. Carved Proplast graft prior to insertion.
-
Proplast nasal grafts. A 20-year-old man with a posttraumatic nasal deformity with septal collapse. Postoperative side view.
-
Proplast nasal grafts. A 20-year-old man with a posttraumatic nasal deformity with septal collapse. Carved Proplast graft to place on alveolar ridge to augment the columellar base.
-
Proplast nasal grafts. A 20-year-old man with a posttraumatic nasal deformity with septal collapse. Proplast alveolar graft in place.





