Background
Congenital malformations of the male genitalia include a wide range of clinical conditions such as hypospadias, epispadias (in females, bifid clitoris) with bladder exstrophy, and hidden penis. Epispadias is an uncommon congenital malformation of the penis and is often part of the condition termed epispadias-exstrophy of the bladder. [1, 2, 3]
Problem
Epispadias is a rare congenital malformation of the male or female urogenital apparatus that consists of a defect of the dorsal wall of the urethra. The extent of the defect can vary from a mild glandular defect (see first image below) to complete defects as are observed in bladder exstrophy, diastasis of the pubic bones, or both (see second image below). Simple epispadias occurs less commonly than the more severe form associated with exstrophy of the bladder.
 Wide diastasis of the pubic bone and external displacement of the hips in epispadias.
Wide diastasis of the pubic bone and external displacement of the hips in epispadias.
Epidemiology
Frequency
Epispadias occurs more commonly in males than in females, with a prevalence of 1 case in 10,000-50,000 persons. The male-to-female ratio is 2.3:1.
Etiology
Unlike hypospadias, epispadias can be explained by defective migration of the paired primordia of the genital tubercle that fuse on the midline to form the genital tubercle at the fifth week of embryologic development. Epispadias and exstrophy of the bladder are considered varying degrees of a single disorder.
Another hypothesis relates the defect to the abnormal development of the cloacal membrane.
Epispadias is rarely observed in 2 members of the same family.
Pathophysiology
In males, epispadias causes impotentia coeundi, which results from the dorsal curvature of the penile shaft, and impotentia generandi, which results from the incomplete urethra.
Also reported are frequent ascending infections to the prostate or bladder and kidneys and psychological problems related to the deformity. If epispadias is distal to the bladder neck, urinary continence may not be present.
Presentation
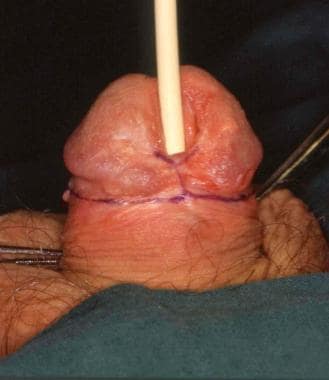
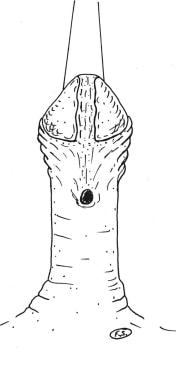
The deformity manifests in males. The normal urethra is replaced by a broad mucosal strip lying on the dorsum of the corpora cavernosa; the meatus is divided dorsally between the tip of the glans and the pubis, the penile shaft is curved dorsally with the absence of the preputial apron, and a cleft is present on the upper surface of the penis (see following image).
 Distal epispadias. Outlining of local flaps from the glans to reconstruct the distal urethra.
Distal epispadias. Outlining of local flaps from the glans to reconstruct the distal urethra.
Epispadias vary in severity according to the time of the pathognomic insult during embryologic development and can be classified as glandular, penile, or complete (ie, penopubic).
With the glandular type, the malformation affects the distal part of the urethra. With the penile type, the entire penile urethra is affected, with an external meatus on the dorsal shaft of the penis. With the complete or penopubic type, a total deficiency of the dorsal wall of the urethra and the anterior wall of the bladder is present. The glans is often spatulated, and the prepuce is clefted dorsally with ventral transposition. All forms of epispadias are associated with chordee. The extent of chordee varies.
In females, epispadias consists of bifid clitoris with diastases of the corpora cavernosa, flattening of the mons, and separation of the labia.
Associated defects are usually limited to the genital tract and diastases of the pubic bones. In exstrophy of the bladder, the lower abdominal wall is absent, with diastasis of the rectus abdominis muscle. Reflux develops in approximately 40% of patients.
Indications
Correction of glandular epispadias with reposition of the distal urethra and creation of a symmetric glans (glanuloplasty) is indicated in childhood or adolescence at the patient's request for cosmetic or psychological reasons.
Penile epispadias is corrected in childhood with penile straightening by resection of the chordee and creation of a new urethra of adequate caliber and length (urethroplasty).
In females, bifid clitoris and normal genitalia appearance can be restored during adolescence.
The aim is to permit normal voiding and erection and to avoid urinary tract infections.
The complete (penopubic) form of the malformation is treated early in childhood to close the abdominal wall and the bladder exstrophy.
Relevant Anatomy
Normally, the male urethra runs through the penile shaft, ventrally to the corpora cavernosa, and meets with the meatus at the tip of the glans.
The penis is formed by the corpus spongiosum surrounding the urethra and by 2 corpora cavernosa; these structures are composed of erectile tissue surrounded by the tunica albuginea (Buck fascia) and the dartos fascia more superficially, which contains terminal branches of external pudendal arteries and veins and the superficial lymphatics.
The vascular axial pattern of the skin-dartos complex originating from the external pudendal vessels is present, but it is dislocated on the ventral aspect of the penile shaft. Additional vascular supply to the prepuce comes from collateral vessels of the terminal glanular branches of the dorsal penile artery. The Buck fascia surrounds the corpora cavernosa and splits to encircle the neurovascular bundle. [4]
Contraindications
Urethroplasty and restoring the normal appearance of the genitalia are contraindicated in infancy because of the small size of the structures.
-
Distal penile epispadias.
-
Wide diastasis of the pubic bone and external displacement of the hips in epispadias.
-
Distal epispadias. Outlining of local flaps from the glans to reconstruct the distal urethra.
-
Reconstruction of distal penile urethra using local flaps (arrows).
-
Vertical island flap drawn on the ventral aspect of the penis.
-
Island flap transferred dorsally and anastomosed to the urethra.
-
Island flap sutured into a tube to reconstruct the missing portion of the urethra.
-
Urethral reconstruction is completed.
-
Drawing of the final appearance at the end of the operation.
-
Photograph of the final appearance at the end of the operation.



